
Abstract
Background:
There has been much debate as to the importance of mechanical bowel preparation (MBP) and oral antibiotic agents (OAB) prior to elective colorectal surgery over the past two decades. There is no consensus between international guidelines.
Methods:
The Australia and New Zealand Mechanical Bowel Preparation and Oral Antibiotics (ANZ-MBP-OAB) questionnaire was distributed to colorectal surgeons after institutional board approval assessing specialist attitudes toward 18 enhanced recovery after surgery (ERAS) interventions. Data were analyzed using a rating scale and graded response model in item response theory (IRT) on Stata MP, version 15 (StataCorp LP, College Station, TX). Specialist attitudes toward the effectiveness of MBP and OAB strategies in providing better short-term outcomes was ranked alongside other ERAS interventions. This was followed by specific questions examining current practice, perspectives, and trends.
Results:
Ninety-five of 300 (31.7%) colorectal surgeons in Australia and New Zealand participated in the survey. Statistical modeling was achieved in 13 ERAS interventions. Compared with other ERAS interventions, the use of MBP with OAB and MBP alone ranked nine of 13 and 10 of 13, respectively, in order of effectiveness in providing better short-term outcomes after colorectal surgery. Oral antibiotic agents alone was not considered effective. Mechanical bowel preparation with OAB was considered to be the best strategy in both colon (37%) and rectal surgery (48%) but current practice varied substantially from perspective. Mechanical bowel preparation alone was strongly favored in rectal surgery (81%) with only 14% using MBP with OAB. In colon surgery, only 10% used MBP with OAB, with MBP alone (45%) and no preparation (45%) being equally the most commonly used strategies.
Conclusions:
Among Australian and New Zealand colorectal surgeons, MBP with OAB was considered the best bowel preparation strategy. However, despite an awareness of its benefits, MBP with OAB has yet to be widely adopted into clinical practice or guidelines in Australia and New Zealand.
The resurgence of interest in the use of mechanical bowel preparation (MBP) and antibiotic agents (OAB) prior to elective colorectal surgery (CRS) has revealed major differences in international guidelines.
The American guidelines recommend “the routine use of a combined isosmotic mechanical bowel preparation with oral antibiotics before elective CRS” [1]. The National Surgical Quality Improvement Program (NSQIP) studies have demonstrated the increasing uptake of MBP with OAB prior to elective CRS in the United States, as well as the risk reduction in surgical site infections (SSIs) associated with MBP with OAB [2–4] as well as OAB alone [4]. A recent survey of U.S. colorectal surgeons reported more than 80% used OAB routinely and 98.6% routinely use MBP prior to elective CRS, with approximately 80% of respondents using of the combination of MBP with OAB for elective CRS [5].
On the other hand, few surgeons in Europe use OAB with or without MBP. In the 2017 survey of European surgeons, fewer than 10% of European colorectal surgeons indicated that they prescribed OAB. Furthermore, although most colorectal surgeons used MBP alone prior to rectal surgery, only 30% of colorectal surgeons used MBP alone prior to colonic surgery [6].
The current Australian guidelines recommend that “MBP should not be used routinely in colonic surgery” [7]. This guideline is supported by the recommendations of the Cochrane Review by Guenaga et al. [8] in 2011 that compared MBP with no preparation and showed no difference between the two approaches in terms of mortality, anastomotic leak, SSI, and re-operation. However, both the 2011 Cochrane Review and the Australian guidelines do not take into consideration the role of OAB in combination with MBP nor OAB alone [7,8]. In 2014, a survey of members of the Royal Australasian College of Surgeons (RACS) revealed that 31.7% of respondents prescribed MBP routinely with 57.3% using MBP selectively, with the most common reasons for its use improved bowel handling (54.9%), requiring a covering ileostomy (40.8%), and personal preference (33.8%) [9]. This survey did not evaluate the use of OAB. To date, there has not been a nationwide survey on MBP and OAB prior to elective CRS in Australia and New Zealand.
Despite the wide range of current practice and guidelines internationally, recent level 1 and 2 evidence has demonstrated the role of MBP with OAB. A Cochrane Review from 2014 by Nelson et al. [10] demonstrated substantial risk reduction in post-operative SSI when OAB was added to the standard regimen of intravenous antibiotic agents compared with OAB alone and intravenous antibiotic agents alone. In 2018, a meta-analysis by McSorley et al. [11] concluded that MBP with OAB was superior to MBP in reducing SSIs, a finding similar to the meta-analysis by Chen et al. [12] in 2016. In 2019, a meta-analysis by Rollins et al. [13] concluded that MBP with OAB was superior to MBP alone in reducing SSIs but was not able to detect a difference in SSIs between MBP with OAB and OAB alone. A 2018 network meta-analysis compared all four combinations (MBP with OAB, MBP alone, OAB alone, and no preparation) and ranked them based on infectious complications [14]. This study reported that MBP with OAB was the best strategy in reducing SSIs, incisional SSIs, and mortality. Oral antibiotic agents alone were ranked as the best strategy for organ/space SSIs and anastomotic leak (AL) [14]. However, the OAB strategy must be interpreted with caution because there were limited data available on OAB alone based on randomized controlled trial (RCT) evidence, albeit the benefit of OAB alone has been supported by data from NSQIP studies including work by Garfinkle et al. [4].
There has been an abundance of evidence-based literature from the international colorectal surgical community assessing the benefit of MBP with OAB over the past few years. These studies have demonstrated the benefits of MBP with OAB or OAB alone. However, the debate continues and a consensus remains elusive.
The purpose of this study was to assess the current practice, perspectives, and trends of colorectal surgeons in Australia and New Zealand regarding MBP with OAB prior to elective CRS. To understand the importance placed by Australian and New Zealand colorectal surgeons on pre-operative MBP and OAB, MBP and OAB strategies have been ranked alongside other peri-operative enhanced recovery after surgery (ERAS) strategies by colorectal surgeons in order of importance in improving short-term outcomes following elective CRS.
Methods
The Australia and New Zealand Mechanical Bowel Preparation and Oral Antibiotics (ANZ-MBP-OAB) questionnaire was distributed to colorectal surgeons in Australia and New Zealand. A 10-scale Likert score was used to assess attitudes toward 18 ERAS features for improving short-term outcomes. The questionnaire received institutional board approval 2019/ETH11810 Australia and New Zealand Mechanical Bowel Preparation and Oral Antibiotics prior to Elective Colorectal Surgery Study and was distributed to members of Colorectal Surgical Society of Australia and New Zealand (CSSANZ).
The questionnaire was divided into two sections. The first section examined the importance placed by members of CSSANZ on well-established peri-operative ERAS interventions as well as MBP and OAB combinations, and ranked the importance placed on pre-operative MBP and OAB alongside other current ERAS strategies. A 10-point Likert scoring system was used to assess attitudes of surgeons toward effectiveness of ERAS strategies on improving short-term outcomes. A Likert score of eight to 10 was considered definitely or very likely effective (Fig. 1); six to seven indicated effective or somewhat effective; five indicated neutral; three to four indicated not really effective and zero to two indicated definitely not effective or very likely not effective (Fig. 2).

Effectiveness of enhanced recovery after surgery (ERAS) strategies in providing better short-term outcomes after colorectal surgery (definitely or very likely effective; Likert score 8/9/10 (percentages as graphed*; effective or somewhat effective, 6/7; neutral, 5; not really effective, 3/4; definitely not effective or very likely not effective, 0/1/2).

Likert plot of specialists' responses to effectiveness of enhanced recovery after surgery (ERAS) interventions in providing better short-term outcomes after colorectal surgery.
The second section examined the current practice and perspectives of colorectal surgeons on pre-operative MBP and OAB, as well as factors that may influence the decision-making for its use. This second part also assessed which oral antibiotic choice was considered the best for selective decontamination as well as willingness to participate in an RCT and feasibility of a large-scale Australia and New Zealand study.
Summary statistics and weighted averages were also calculated where applicable (Table 1). Data in the first section were then analyzed using a rating scale and graded response model in item response theory (IRT) on Stata/MP, version 15 (StataCorp LP, College Station, TX) (Table 1). Item response theory is useful in scoring of tests and questionnaires. Based on IRT, the surgeon's level of performance overall compared with other respondents was incorporated into scaling their responses to each item. Rounding to integer values, we created grades of effectiveness based on the IRT score. We correlated IRT score of ≥7.50 as grade 1; 5.5–7.49 as grade 2; 4.5–5.49 as grade 3; 2.5–4.49 as grade 4; and 0–2.49 as grade 5 in terms of effectiveness.
Item Response Theory Scores and Grade of Effectiveness of ERAS Strategies in Improving Short-Term Outcomes after Elective Colorectal Surgery and Weighted Means and Percent Likert Scores 8–10 for ERAS Interventions
0 - definitely not; 5 - neutral; 10 - definitely. ERAS=enhanced recovery after surgery; IRT=item reponse theory; CI=confidence interval; NGTs=nasogastric tubes; NSAIDs=non-steroidal anti-inflammatory drugs; MBP=mechanical bowel preparation; OAB=oral antibiotic agents.
Results
Ninety-five colorectal surgeons in Australia and New Zealand participated in the survey. The response rate was 31.7% (95/300).
Importance of MBP and OAB ranked with other ERAS interventions
Likert plot analysis with an overview of Likert scores allocated to ERAS interventions by surgeons has been provided in Figure 2. Based on specialists' perspectives, the most effective ERAS strategies in improving short-term outcomes were pre-operative iron infusion for patients with anemia, minimally invasive surgery, early in-dwelling catheter (IDC) removal, and pre-operative smoking cessation. Mechanical bowel preparation with OAB ranked similar in importance to early drain removal in rectal cancer and pre-operative immunonutrition. Mechanical bowel preparation alone was ranked similar to selective non-steroidal anti-inflammatory drugs (NSAIDs) and epidural for open surgery. Use of OAB alone was not considered effective in improving short-term outcomes.
Importance of MBP and OAB ranked by likelihood of improving short-term outcomes
A total of 24.2% of surgeons believed that MBP with OAB was very likely or definitely better than no preparation in providing better short-term outcomes after colorectal surgery; 13.7% preferred MBP alone; and 1.1% preferred OAB alone. Based on a Likert score of eight to 10, MBP and OAB ranked eight of 18, MBP alone ranked 13 of 18, and OAB alone ranked 18 of 18 in order of effectiveness of ERAS strategies considered to definitely or very likely provide better short-term outcomes (Fig. 1). In terms of weighted mean, MBP with OAB ranked 10 of 18, MBP alone ranked 13 of 18, and OAB alone ranked 17 of 18.
Importance of MBP and OAB ranked by statistical modeling
Item response theory modeling was used to analyze the results of this survey statistically. Item response theory modeling was achieved in 13 of 18 ERAS interventions (Fig. 3 and Table 1). Based on IRT scores, MBP with OAB ranked nine of 13 and MBP alone ranked 10 of 13. The use of OAB alone was not computable because of discontinuous regions and based on weighted mean of 3.06 and only 1.1% of surgeons scored OAB alone as definitely or likely to improve short-term outcomes, it was evident that colorectal surgeons did not consider OAB alone to be useful in improving outcomes.
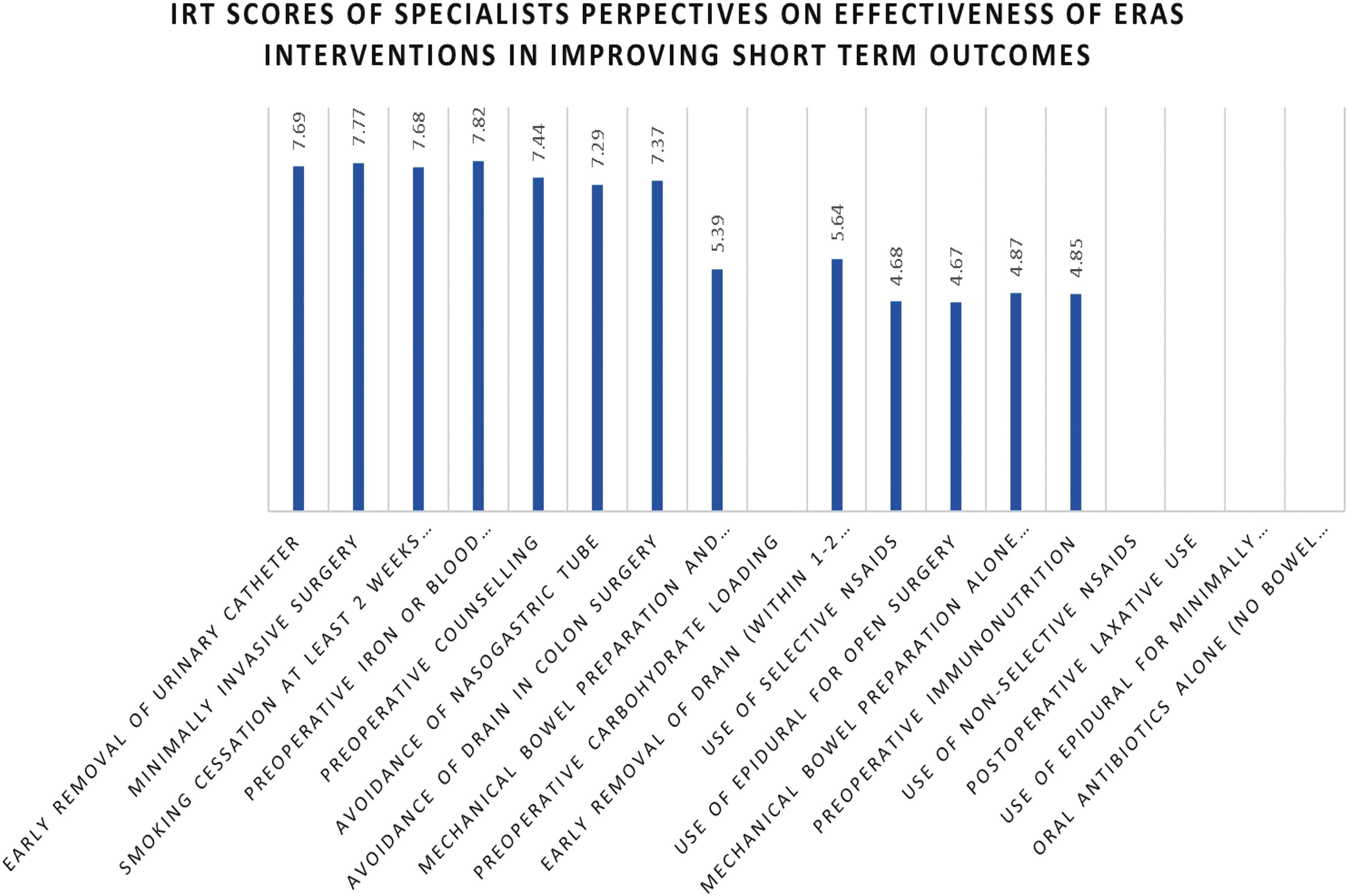
Item response theory (IRT) scores of specialists' perspectives on the effectiveness of enhanced recovery after surgery (ERAS) strategies in providing better short-term outcomes after colorectal surgery.
Mechanical bowel preparation and OAB preferences for colon and rectal surgery
Surgeons were also asked questions related directly to MBP and OAB. For colon surgery, the current practice was 45% no preparation; 45% MBP alone; 10% MBP with OAB; none used OAB alone. When asked about the best bowel preparation strategy for colonic surgery, 37% responded MBP with OAB; 27%, no preparation; 22%, MBP alone; 2%, OAB alone; 2%, no difference between groups; and 10%, not sure (Fig. 4).
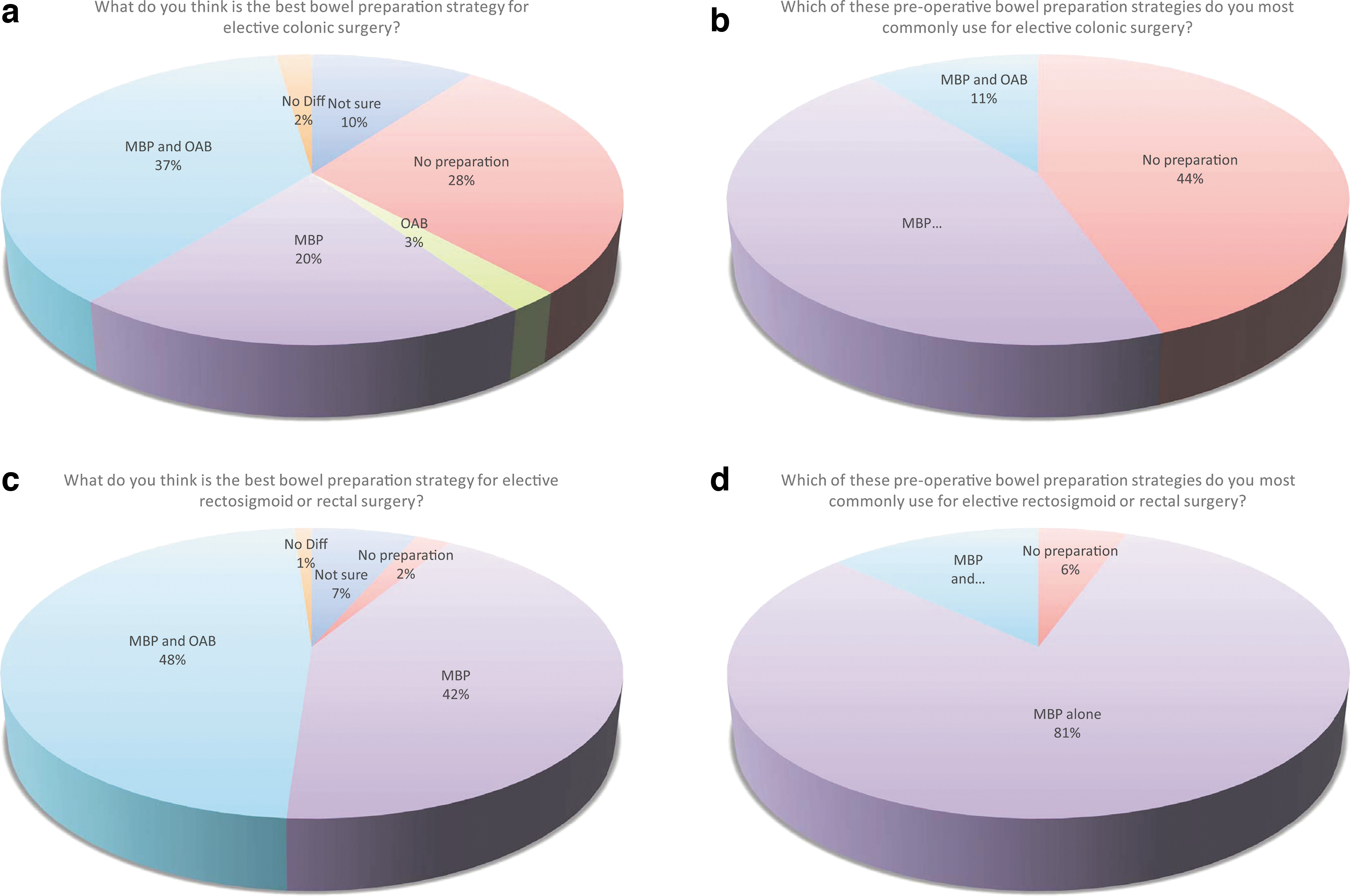
Specialists' perspectives on best bowel preparation strategy for rectal and colonic surgery.
For rectal surgery, the majority used MBP alone (81%); 14% used MBP with OAB; 5% no preparation; and 0% OAB alone. When asked about the best bowel preparation strategy for rectal surgery, 48% responded MBP with OAB; 42%, MBP alone; 2%, no preparation; 0%, OAB alone; 1%, no difference between groups; and 6%, not sure (Fig. 4).
Mechanical bowl preparation and OAB preferences for minimally invasive and open surgery
When asked if the decision to perform minimally invasive surgery or open surgery would influence the decision to use MBP and OAB, 87% of surgeons reported no difference; 9% would more like use MBP with OAB in laparoscopic surgery and 1% in open surgery. Three percent were not sure (Fig. 5).
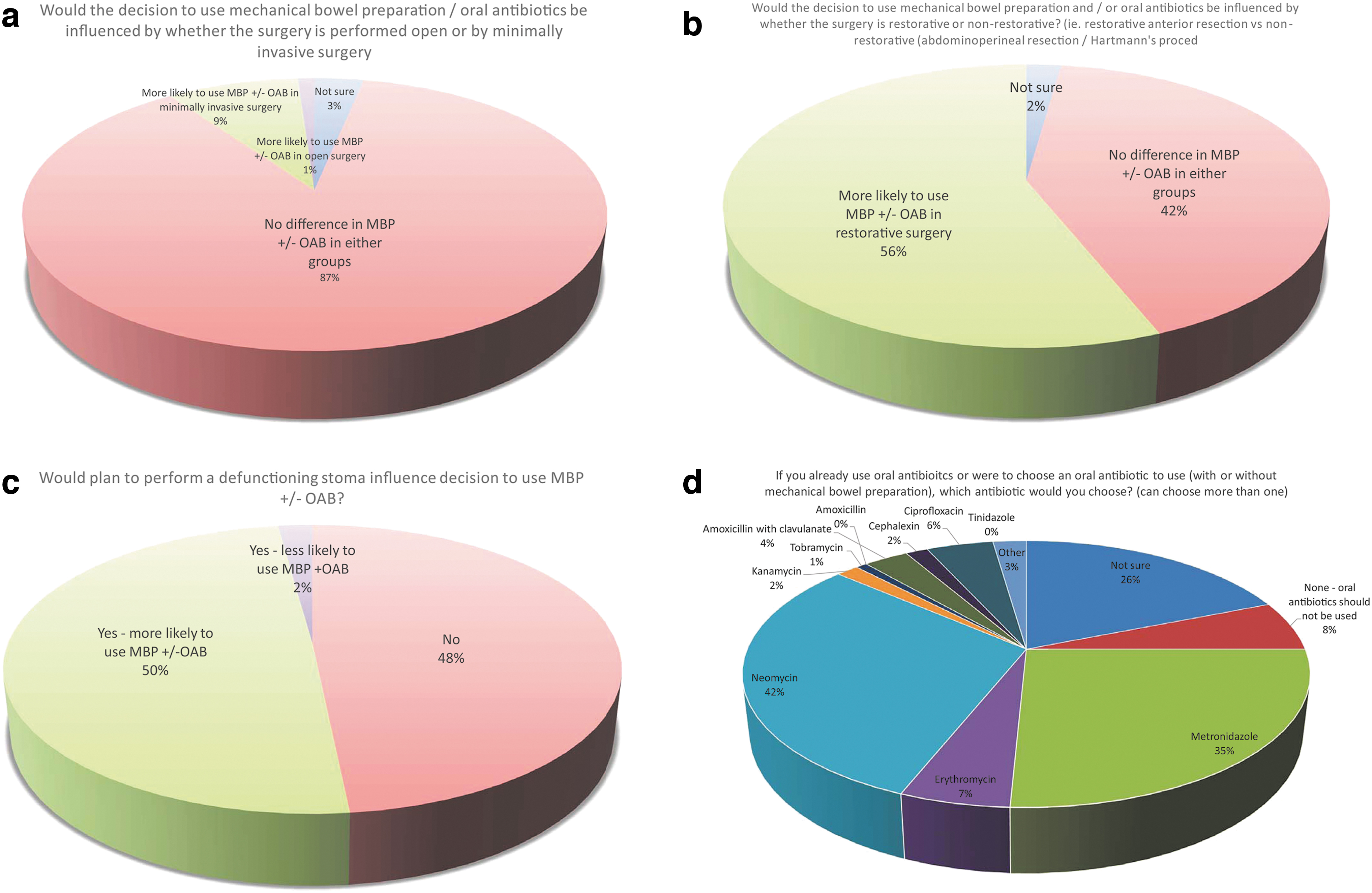
Other considerations regarding bowel preparation and oral antibiotics in colorectal surgery.
Mechanical bowl preparation and OAB preferences for restorative and non-restorative procedures
Fifty-five percent of surgeons would more likely use MBP with OAB in restorative procedures (anterior resection). Forty-two percent responded that whether the procedure is restorative or non-restorative made no difference in decision-making to use MBP with OAB. Three percent were not sure (Fig. 5).
Mechanical bowl preparation and OAB preferences based on plan to perform a defunctioning stoma
For restorative procedures, surgeons were divided on whether the plan to perform a defunctioning stoma would influence the use of MBP with OAB. Forty-eight percent indicated that the plan to perform a defunctioning stoma would not influence decision making on MBP with OAB. Forty-nine percent of surgeons responded that the plan to perform a defunctioning stoma would increase the likelihood to use MBP with OAB. Three percent were less likely to use MBP with OAB for restorative procedures with planned diversional stomas (Fig. 5).
Choice of antibiotic agents
Neomycin (42%) and metronidazole (35%) were the most popular oral antibiotic agents chosen by respondents to be used prior to elective colorectal surgery. Specialists were able to choose more than one OAB of choice because a majority of existing trials have used a combination of OABs to ensure adequate aerobic and anaerobic cover. Twenty-six percent were not sure. Eight percent were resolute that no antibiotic agents would be suitable. Seven percent preferred erythromycin; 6%, ciprofloxacin; 4%, amoxicillin with clavulanate; 1%, tobramycin; 2%, kanamycin; 2%, cephalexin; and 3%, other. None of the surgeons chose amoxicillin or tinidazole (Fig. 5).
Willingness to participate in an RCT in Australia and New Zealand
There was interest demonstrated by colorectal surgeons to take part in an RCT in Australia and New Zealand. Sixty-two percent responded that they would take part in an RCT; 20%, maybe; 11%, no; 7% did not respond to the question about participation in RCT (Fig. 6).
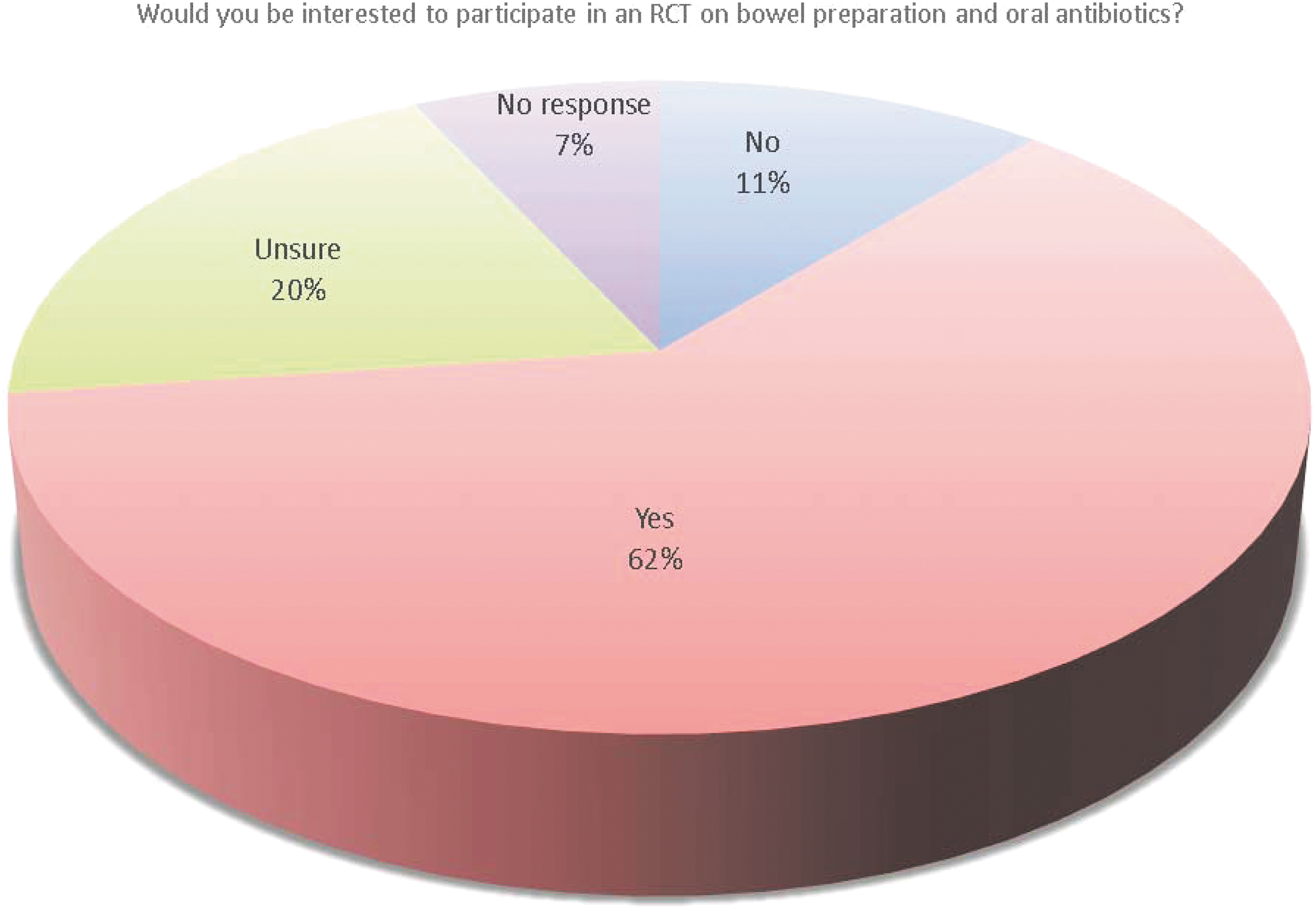
Interest by specialists in Australia and New Zealand in participating in a randomized controlled trial on mechanical bowel preparation and oral antibiotic agents prior to elective colorectal surgery.
Discussion
Current guidelines in Australia and New Zealand since 2017 have provided a grade D recommendation for the use of MBP with the evidence-based conclusion that MBP should not be used routinely in colonic surgery but can be used selectively at the surgeon's discretion [7]. This is in line with the 2011 Cochrane Review recommendations [8]. However, a survey of Australian surgeons in 2014 revealed that a substantial proportion of surgeons did not follow the national guidelines with 31.7% prescribing MBP routinely and approximately 60% prescribed MBP selectively for elective colorectal surgery, with the main reason to improve bowel handling [9]. In this survey, approximately 25% of surgeons prescribed MBP for right hemicolectomy whereas less than 50% utilized MBP prior to low anterior resection [9].
Since this survey, there has been abundant level 1 and 2 evidence demonstrating that both no preparation and MBP was inferior to MBP with OAB and OAB alone [2,11–13], but it was unclear as to whether the current practice and perspectives of colorectal surgeons in Australia and New Zealand reflected the changing international landscape on MBP and OAB use prior to elective CRS. For this reason, we decided to ascertain the patterns of practice in Australia and New Zealand as well as understand the perspectives, trends, and factors that influence decision-making on the use of MBP and OAB.
In this survey, the majority (90%) of Australia and New Zealand colorectal surgeons most commonly used no preparation (45%) or MBP alone (45%) for colon surgery. However, MBP with OAB was considered the best approach. Despite this, only 10% prescribed MBP with OAB.
Approximately 80% of Australia and New Zealand colorectal surgeons used MBP alone for rectal surgery, 5% no preparation, and 0% OAB alone. Only 14% prescribed MBP with OAB. However, almost 50% believed that MBP with OAB was the best approach for rectal surgery. Only 2% believed no preparation was the best strategy and no colorectal surgeon thought OAB alone was the best strategy.
The pattern of practice of bowel preparation was similar to the bowel preparation practice used in Europe (for colonic surgery 74.9% used MBP [29.6% routinely, 45.3% selectively] and rectal surgery 94.6% [77% routinely, 17.6% selectively]). Only 11% of respondents used OAB [6]. This contrasted dramatically with the pattern of practice by U.S. colorectal surgeons with 83.2% routinely prescribing pre-operative OAB and 98.6% routinely using MBP, and 79.3% routinely prescribing MBP with OAB [5].
Herein lies the dilemma for Australia and New Zealand colorectal surgeons. Although there appeared to be an awareness of the benefits of MBP with OAB, the uptake of this strategy was low (10% for colon surgery and 14% for rectal surgery). A large majority still used MBP alone (81% rectal; 45% colon) despite strong evidence in the literature reporting no benefit with MBP alone. Ease of bowel handling has been rationalized for its use [9]. Surgeons who utilize MBP alone argue that MBP alone may improve the ease of performing anastomosis particularly in difficult low pelvic anastomosis even if the scientific evidence does not show any improvement in AL rates.
Perhaps, the difference between perspective and current practice may otherwise be explained by the phenomenon described by Dellinger [15] and Morris et al. [16], namely, the 17-year time lag between the development, dissemination, and understanding of new evidence to its widespread adoption into clinical practice.
One of the major barriers to the uptake of MBP with OAB use may be that neomycin which was the most popular oral antibiotic chosen by colorectal surgeons to use for selective decontamination (42%) does not have Therapeutic Goods Administration (TGA) approval for its use for selective decontamination prior to elective colorectal surgery. For this reason, to use neomycin, surgeons currently must apply for an authorized prescriber application that may need local governance drug committee approval, human research ethics committee approval, and TGA approval. Neomycin, when used with antibiotic agents with broad anaerobic coverage such as erythromycin or metronidazole, is the oral antibiotic that has shown the most evidence of benefit for selective decontamination in a majority of previous RCTs [14]. Oral neomycin alone does not have sufficient anaerobic cover. Neomycin and metronidazole is also the most frequently selected oral antibiotic strategy (58.4%) in the recent U.S. survey [5]. Therapeutic Goods Administration approval for neomycin may help to fast track the use of OAB in Australia and New Zealand and would also reduce potential obstacles in setting up a large-scale RCT in Australia and New Zealand should a trial using neomycin be commenced.
There are currently 12 international trials on MBP/OAB combinations. PreCaution (The Netherlands), COMBINE (France), SELDDEC (Ireland), REaCT-NSQIP (Canada), COLONPREP (France), PREPACOL2 (France), MECCA (Grece), MOBILE2 (Finland), NCT03856671 (China), NCT03436719 (Russia), NCT03042091 (United States), and ORALEV2 (Spain).
Limitations
The response rate of Australian and New Zealand colorectal surgeons was only 31.7% (95/300). This was lower than the response rate of European colorectal surgeons, which was 40.2% (426/1059) [6] but higher than the U.S. colorectal surgeons (11.2%; 359/3206) [5]. This survey did not consider enema administration as part of MBP and did not examine the current practice or perspectives of enema use prior to elective CRS. Although the choice of antibiotic agents was examined, the choice of MBP was not assessed. In the 2014 survey, 66.7% used sodium picosulfate, 37.2% used polyethylene glycol, and 10.3% used sodium phosphate [9]. This was intentional because the focus of this survey was to shift attention to the use of OAB with or without MBP rather than focus on MBP. It is important to note that this survey did not interrogate current practice or perspectives on the use of parenteral antibiotic agents because there is international consensus that parenteral antibiotic agents are essential prior to elective CRS and the recommendations for its use is part of the World Health Organization and U.S. Centers for Disease Control and Prevention guidelines.
Conclusions
This survey summarizes the current practice, perspectives, and trends of Australia and New Zealand colorectal surgeons. The most frequently selected strategy prior to rectal surgery was MBP alone and prior to colon surgery was equally MBP alone or no preparation. Whereas there was an awareness that pre-operative MBP with OAB may be the best bowel preparation strategy prior to elective colorectal surgery, the uptake of this strategy was low and major barriers currently limit its widespread adoption. No respondents used OAB alone, and this was not considered to be an effective strategy. Neomycin and metronidazole were considered the best choice of antibiotic agents. When the importance of MBP with OAB was ranked alongside other ERAS interventions in order of importance in improving short-term outcomes, MBP with OAB ranked similar in importance to early drain removal in rectal cancer and pre-operative immunonutrition. Mechanical bowl preparation alone was ranked similar to the use of selective NSAIDs and epidural for open surgery. Use of OAB alone was not considered effective in improving short-term outcomes.
Footnotes
Authors' Contributions
Dr. Toh made substantial contributions to the design and interpretation of the study including acquisition of data, statistical analysis, drafting and revision of manuscript. Drs. Chen, Yang, Reza, Pathmanathan, El Khoury, Smith, Engel, Rickard, Keshava, Young, and Ctercteko contributed to the interpretation and revision of manuscript. All authors approved the final version to be published.
Funding Information
No funding has been reported.
Author Disclosure Statement
The authors declare no conflict of interest.