
Abstract
Background:
Institutional programs such as antibiotic stewardship (ABS) programs offer possibilities to monitor and modify antibiotic usage with the aim of reducing antibiotic resistance. In orthopedic units that treat peri-prosthetic joint infections (PJIs), ABS programs are still rare, however, there is extensive use of high-risk antibiotic agents and an increased risk for the occurrence of Clostridium difficile infections (CDIs).
Patients and Methods:
An ABS program was implemented at the Department of Orthopedic Surgery at a university hospital. Quarterly antibiotic consumption was measured in defined daily doses (DDDs) per 100 patient-days (PDs) at 10 quarters before the intervention and seven quarters after the intervention. The effect of the new antibiotic policy on drug use rates was evaluated using an interrupted time-series analysis. Estimated changes over time in the incidence of CDIs (cases per 1,000 PDs) were analyzed.
Results:
A remarkable percentual reduction in second-generation cephalosporin use of 83% (p < 0.001; pre-intervention level, 81.486 DDDs/100 patient-days; post-intervention level, 13.751 DDDs/100 PDs) and clindamycin administration of 78% (p < 0.001; pre-intervention level, 18.982 DDDs/100 PDs; post-intervention level, 4.216 DDDs/100 PDs) was observed after implementation of ABS interventions. Total antibiotic use declined by 25% (p < 0.001; pre-intervention level, 129.078 DDDs/100 PDs; post-intervention level, 96.826 DDDs/100 PDs).
Conclusions:
This research assessed the positive impact of an intensified ABS program at an orthopedic department specializing in PJIs. Antibiotic stewardship program interventions encourage the reduction of total antibiotic usage and especially high-risk antibiotic agents, associated with the development of antimicrobial resistance.
There has been a dramatic emergence of antimicrobial resistance in Europe and the United States in the past decades. According to national and international organizations, such as the U.S. Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO), multi-drug–resistant bacteria are currently a major public health concern [1]. Especially in healthcare settings, the management of multi-drug–resistant infections will become one of the key issues in future years.
Orthopedic surgical units that specialize in septic surgery are disproportionately exposed to this problem. With demographic changes in modern industrial societies, arthroplasty and revision arthroplasty are increasingly performed in older patients with underlying diseases, e.g., diabetes mellitus and rheumatoid arthritis. These patients are at high risk of developing peri-prosthetic joint infection (PJI). With implanted foreign material, only small amounts of bacteria are necessary to induce severe biofilm-associated infections [2–4]. Peri-prosthetic joint infection is a devastating complication, with an impact on patient survival rates; multiresistance patterns decrease the probability of eradication. A multidisciplinary diagnostic, surgical, and antimicrobial concept is necessary for the successful treatment of these complex implant-associated infections [5].
Institutional programs, such as antibiotic stewardship (ABS) programs, aim to optimize antimicrobial use to improve patient care and to achieve the best clinical outcomes possible [6]. These programs monitor and modify the prescription rate of antibiotic agents in hospitals and outpatient settings. Combined with educational measures, active interventions, and restrictive measures in clinical practice characterize the principles of ABS programs [7–9]. Therefore, ABS programs help to influence the incidence of nosocomial infections and prevent the emergence of antimicrobial resistance [10].
Several studies have analyzed the impact of ABS programs in intensive care units and internal medicine departments, however, data on ABS programs in orthopedic surgery departments are rare. Moreover, orthopedic units that specialize in the treatment of PJIs are often characterized by high antibiotic drug use rates especially when administering long-term therapies combining intravenous and oral antibiotics. Orthopedic patients with complex biofilm-associated infections benefit from multidisciplinary teams who prescribe the optimal antimicrobial regimen considering drug selection, dosage, and duration of therapy.
Hospital-acquired Clostridium enteritis [11] is associated with some high-risk antibiotic agents, such as second- and third-generation cephalosporins, fluoroquinolones, and clindamycin. Clostridium difficile infection (CDI) is a modifiable risk factor for morbidity in orthopedic patients [12]. The aim of this study was to determine the effects of an ABS program on changes in antibiotic drug usage with regard to high-risk antibiotics and the incidence of CDIs.
Patients and Methods
Setting
This study was performed at the Department of Orthopedic Surgery, in a large university hospital in southern Germany. The Department of Orthopedic Surgery is a national center for special surgery for PJIs. Approximately 1,000 arthroplasties are performed each year, with a high number of revision arthroplasties. Treating approximately 150 PJIs annually, this hospital is one of the largest centers in Germany. During the observation period the Department of Orthopedic surgery was constantly treating complex cases in orthopedic surgery. The hospital pharmacy and microbiology laboratories are part of the university and are located on the same campus.
Collection of data, ABS program, and interventions
An ABS program was initiated at the university hospital in 2013. The ABS team comprised a pharmacist, a microbiologist, and a clinician from each department. Data regarding antibiotic consumption were collected by the hospital pharmacy and analyzed by the ABS team. Data analysis started in January 2011. Drug use data were extracted from merchandise management program AMOR®3 (Aescudata GmbH, Winsen (Luhe), Germany) in the hospital pharmacy. The antibiotic agents delivered to the orthopedic ward per quarter were used to calculate the antibiotic consumption data. As a unit of measurement defined daily doses (DDDs) per 100 patient-days (PDs) were used. Analysis of DDDs was performed applying WHO ATC classification index.
Patient-days were extracted from the hospital information system. For patient-days, the admission day and each additional day of hospitalization without transfer or discharge day were counted. Antibiotic stewardship interventions targeting antibiotic use and Clostridium difficile-associated infections, especially in the Department of Orthopedic Surgery, were continuously implemented from the beginning of August 2013 (quarter 11 [Q11]). The aim of the new antibiotic policy was a reduction in total antibiotic usage and a decrease in the use of high-risk agents for CDI, such as cephalosporines, clindamycin, and quinolones.
The preferred agent groups were aminopenicillins and narrow-spectrum penicillins. This new policy was realized by the joint development of a local guideline for peri-operative antibiotic prophylaxis, which specifically focused on the duration of prophylaxis and a diagnostic algorithm for implant-associated infection. In addition, antibiotic treatment for PJI was assessed according to previously published treatment recommendations. Guideline adherence was attained by teaching workshops as well as the distribution of electronic and laminated editions of the guideline. A main factor supporting the change in the antibiotic policy was regular interdisciplinary ward rounds to establish antibiotic concepts for patients with infections. Additional patient individual consultations were carried out separately, as needed. The interdisciplinary team comprised an orthopedic surgeon specialized in septic surgery, a clinical microbiologist, and a pharmacist.
Microbiologic analysis
Stool samples from patients with diarrhea were analyzed at the microbiology laboratory. A commercial enzyme-linked immunosorbent assay (ELISA) to detect Clostridium difficile toxins A and B was performed once per day, and specimens were cultured for Clostridium difficile (Brazieres Selective Media, Oxoid, Germany). In toxin-negative cases, cultures were checked for the growth of Clostridium difficile after 48 and 72 hours. Culture-positive samples were tested again with an ELISA for Clostridium difficile toxins A and B. Patients with diarrhea and a toxin A-/B-positive stool sample were defined as CDI cases.
Statistical analysis
Data regarding antibiotic usage were collected quarterly from January 2011 to March 2015 (51 months). Baseline level (Q1) was defined as the value of antibiotic consumption at the beginning of the study. A pre-intervention level was determined before starting the ABS program in the Department of Orthopedic surgery (Q10) and post-intervention level (Q17) after termination of the study. The pre-intervention period was defined as Q1 to Q10 (30 months) and post-intervention period as Q11 to Q17 (21 months). An interrupted time-series (ITS) analysis for slope change was applied to evaluate the effects of the implemented ABS interventions on antibiotic consumption [13,14]. Therefore, a Poisson regression model was fit to the quarterly sums of DDDs as outcome, using the count of months since baseline as continuous predictor variable to estimate the pre-intervention trend and using the count of months since intervention, setting months before intervention to 0, as continuous predictor variable to estimate the change of the trend after intervention. The quarterly sums of PDs served as offset in the Poisson regression model to enable the modeling of DDD rates per PDs. The latter were multiplied by 100 to obtain DDD rates per 100 PDs in the presentation of results. The Newey-West method for autocorrelation consistent covariance matrix estimation with automatic lag selection was applied to account for autocorrelation [15,16]. These parametric models were also used for hypothesis testing and to estimate pre- and post-intervention trends, differences in trends, and average DDDs at specific points in time with corresponding 95% confidence intervals on the log-scale. The latter is specific to Poisson regression models. Back-transformation of effects from the log-scale to the linear scale turns differences into ratios that can also be interpreted as percentage changes. Clostridium difficile infections per 100 PDs were analyzed in the same way. Hypothesis testing was performed on two-sided 5% significance levels. Analyses were conducted in R 3.6.1 (The R Foundation for Statistical Computing, Vienna, Austria) using the packages multcomp [16] for linear hypothesis testing of model parameters and the package sandwich [17] for autocorrelation consistent covariance matrix estimation as described above.
Results
Antibiotic use
At the Department of Orthopedic surgery second-generation cephalosporins and clindamycin were the antibiotic classes with the highest consumption before the implementation of an ABS program (Fig. 2 and 3). Both substance classes showed a slightly increasing trend per quarter before the intervention by 0.8% (second-generation cephalosporins: pre-intervention trend, 1.008 DDDs/100 PDs) and 3.3% (clindamycin: pre-intervention trend, 1.033 DDDs/100 PDs). After implementation of an ABS program, antibiotic consumption levels, as well as trends were remarkably reduced. Impact on second-generation cephalosporins and clindamycin was probably strongest after the implementation of a guideline targeting the duration of peri-operative antibiotic prophylaxis with a quarterly percentage decrease in trends by 22.4% (second-generation cephalosporins: post-intervention trend, 0.776 DDDs/100 PDs) and 19.3% (clindamycin: post-intervention trend, 0.807 DDDs/100 PDs), respectively, and a percentage reduction of antibiotic usage by 83.1% for second-generation cephalosporins (pre-intervention level [Q10], 81.486 DDDs/100 PDs; post-intervention level [Q17], 13.751 DDDs/100 PDs; quotient Q17–Q10: 0.169; p < 0.001) and 77.8% for clindamycin (pre-intervention level [Q10], 18.982 DDDs/100 PDs; post-intervention level [Q17], 4.216 DDDs/100 PDs; quotient Q17–Q10: 0.222; p < 0.001). The impressive post-intervention reduction of these two substance classes was also reflected in the total antibiotic use. Trend of total antibiotic use after intervention decreased by 4% per quarter (total antibiotic agents: pre-intervention trend, 1.006 DDDs/100 PDs; postintervention trend, 0.960 DDDs/100 PDs) and a percent decrease of overall antibiotic usage by 25% (pre-intervention level [Q10], 129.078 DDDs/100 PDs; post-intervention level [Q17], 96.826 DDDs/100 PDs; quotient Q17–Q10: 0.750; p < 0.001) was observed reflecting the effectiveness of the interventions.
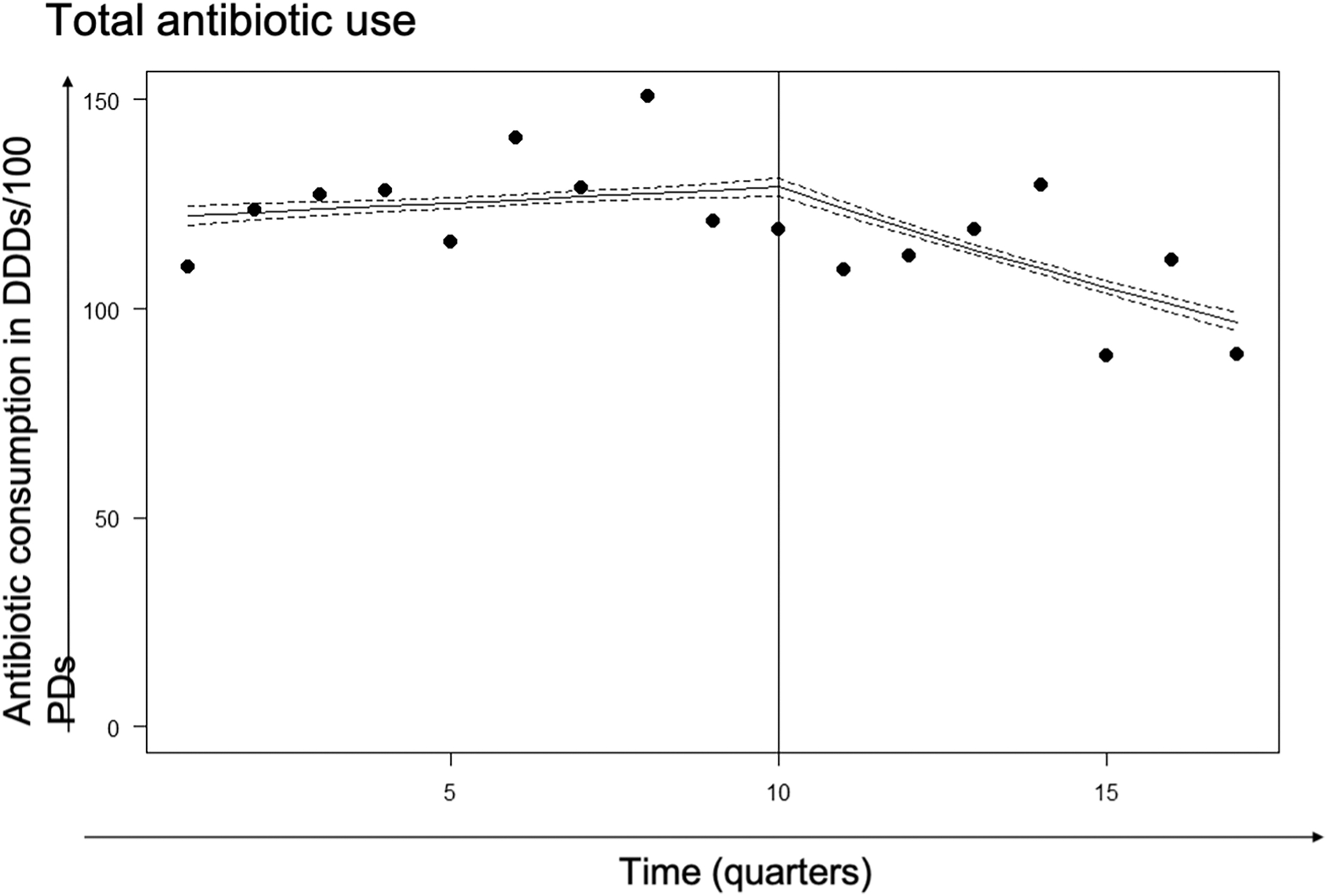
Quarterly antibiotic use of total antibiotic usage in DDDs/100 PDs before and after implementation of an ABS program. Solid line: pre-, and post-intervention trend. Dashed line: 95% confidence intervals. Dotted line: introduction of ABS interventions. ABS = antibiotic stewardship; DDDs = defined daily doses; PDs = patient-days).

Quarterly antibiotic use of second-generation cephalosporins in DDDs/100 PDs before and after implementation of an ABS program. Solid line: pre- and post-intervention trend. Dashed line: 95% confidence intervals. Dotted line: introduction of ABS interventions. DDDs = defined daily doses; PDs = patient days; ABS = antibiotic stewardship.

Quarterly antibiotic use of clindamycin in DDDs/100 PDs before and after implementation of an ABS program. Solid line: pre- and post-intervention trend. Dashed line: 95% confidence intervals. Dotted line: introduction of ABS interventions. DDDs = defined daily doses; PDs = patient days; ABS = antibiotic stewardship.
Reverse modification of empirical therapy for the treatment of bone and soft tissue infections, with preference for aminopenicillins led to a quarterly post-intervention significant increasing trend by 30% (post-intervention trend, 1.298 DDDs/100 PDs) for this substance class. The effect of implementing de-escalation strategies in regular ward rounds was a continuing increasing trend for narrow-spectrum penicillins with a post-intervention quarterly increase of 21% (post-intervention trend, 1.209 DDDs/100 PDs). Detailed pre-intervention and post-intervention levels and trends of antibiotic use are shown in Table 1 and Table 2, using DDDs/100 PDs.
Interrupted Time Series Analysis: Pre-Interventional and Post-Interventional Trend of Antibiotic Consumption Using DDDs/100 PDs
95% confidence intervals (CI) in parentheses.
DDD = defined daily doses; PDs = patient days; ABS = antibiotic stewardship.
Interrupted Time Series Analysis: Pre-Intervention and Post-Intervention Level of Antibiotic Consumption Using DDDs/100 PDs
95% confidence interval (CI) in parentheses.
DDD = defined daily doses; PDs = patient days; ABS = antibiotic stewardship.
Baseline level: value of antibiotic consumption at the beginning of the study (quarter 1, (Q1))
Pre-intervention level: value of antibiotic consumption before initiation of ABS interventions (quarter 10, (Q10))
Post-intervention level: value of antibiotic consumption at termination of the study (quarter 17, (Q17))
Clostridium difficile infections
During the entire study period a total of 16 CDI cases (12 CDI cases pre-intervention and four CDI cases post-intervention) were observed in 50.161 PDs. In the pre-intervention period, the incidence rate of Clostridium difficile-associated infections decreased from 0.057/100 PDs (95% CI, 0.022–0.145) to 0.031/100 PDs (95% CI, 0.011–0.084). That means a percentage reduction of 45.6% (quotient Q10–Q1, 0.544; 95% CI, 0.108–2.737; p = 0.460). After the implementation of the ABS program, it decreased further to 0.011/100 PDs (95% CI, 0.002–0.070). The post-intervention percentage reduction of 65% was not statistically significant (quotient Q17–Q10, 0.349; 95% CI, 0.033–3.735; p = 0.384). Pre-intervention as well as post-intervention trends were decreasing with 0.935 (95% CI, 0.781–1.118; p = 0.460) and 0.860 (95% CI, 0.613–1.207; p = 0.384) per 100 PDs.
Discussion
In this study, we clearly demonstrated the positive effect of implementation of an ABS program on antibiotic usage in a specialized orthopedic surgery department. We clearly demonstrated substantial improvements in antibiotic use concerning the amount of antibiotic agents used and the reduction in the use of high-risk antibiotic agents. A reduction in the rate of CDIs was observed but change over time was not significant and a decreasing trend was already present in the period before the ABS intervention.
According to Borde et al. [18,19] and Talpaert et al. [20], ITS analysis was applied as statistical tool of choice for analyzing ABS interventions and differentiating between baseline trends and true intervention-related effects [13]. Data of antibiotic consumption were aggregated at a quarterly level as usage of quarterly data is common in interrupted time series analysis of drug utilization [14].
We are aware of limitations of our study. First, our cohort is small compared with other studies because we included only orthopedic patients. Our cohort could not be compared easily with other cohorts because the Department of Orthopedic Surgery is specialized in prosthetic joint infection and special surgery, and therefore treats a rather uncommon patient collective compared with other hospitals and study cohorts. Furthermore, antibiotic usage was analyzed quarterly not monthly, as officially required from our national surveillance program.
Another limitation of this study is that the pre-intervention CDI rate in the department was low; CDI outbreaks are uncommon in our hospital and are not widespread in Germany. Our cohort is too small to prove significant reduction of CDIs post-intervention.
The implementation was associated with a significant reduction in total antibiotic use with a percent decrease of 25% (pre-intervention level [Q10], 129.078 DDDs/100 PDs; post-intervention level [Q17], 96.826 DDDs/100 PDs; quotient Q17–Q10, 0.750; p < 0.001) in the orthopedic wards. As postulated by the Society for Healthcare Epidemiology of America (SHEA), a general reduction in antibiotic usage restricts the selective pressure on bacterial species, which is associated with the emergence of antimicrobial resistance in gram-positive and gram-negative bacteria [6,21]. Currently, vancomycin-resistant enterococci, extended-spectrum β-lactamase-producing Enterobacterales and carbapenem-resistant Enterobacterales are widespread in healthcare settings. This development is associated with increasing patient morbidity and mortality and expanding healthcare costs [6]. The findings in this study obviously indicate the potential of ABS interventions to reduce antibiotic usage in orthopedic departments specializing in PJI treatment. Our results agree with those of Talpaert et al. [20]. In contrast with our study, they determined antibiotic usage in very different subspecialties, such as different fields of internal medicine and in surgical wards. Interestingly, the potential for reducing total antibiotic usage in orthopedic departments that specialize in treating PJIs is the same as that in other departments, as shown by Talpaert et al. [20].
Our study is important in demonstrating the substantial positive effects of ABS interventions in orthopedic special surgery wards. The present work differs from other studies in one important parameter: the time period of follow-up. We clearly demonstrate the long-term effects of ABS interventions in orthopedic surgery cases, with an overall surveillance period of 17 quarters (10 quarters pre-intervention/seven quarters post-intervention). According to Fowler et al. [22], who demonstrated the positive effects of ABS intervention on the CDI rate in an internal medical ward, long-term reduction is one of the main goals of ABS intervention.
Although the reduction in the total amount of prescribed antibiotic agents serves as an indicator for the success of ABS interventions, the reduction in high-risk antibiotic agents, such as second- and third-generation cephalosporins, fluoroquinolones, and clindamycin, is likely associated with a decreased risk for CDI as well as colonization and infection with drug-resistant bacteria [7,8,18,23,24]. The relation between high-risk antibiotic usage and the promotion of drug resistance and CDI has been reported in several studies [7,23,24]. Even the probability of methicillin-resistant Staphylococcus aureus (MRSA) occurrence and its related costs are associated with the use of fluoroquinolones and cephalosporins [25,26].
High-risk antibiotic prescription was a relevant problem in the pre-intervention period in the orthopedic department, as indicated by the excessive use of cephalosporins and clindamycin. After the intervention, second-generation cephalosporin usage was reduced by 83% (pre-intervention level [Q10], 81.486 DDDs/100 PDs; post-intervention level [Q17], 13.751 DDDs/100 PDs; quotient Q17–Q10, 0.169; p < 0.001). The reduction ratio exceeds the ratio of other workgroups. For example, Borde et al. [18] reported a reduction in antibiotic consumption of 51% (249.6 DDD/1,000 PDs pre-intervention to 121.7 DDD/1,000 PDs post-intervention). This substantial reduction in our cohort could be partially explained by the implementation of revised guidelines regarding the duration of peri-operative antibiotic prophylaxis (AMP).
Before the intervention, the AMP agent and duration were inconsistent and were prescribed by the surgeon up to seven days after surgery. The pre-intervention AMP protocol, which was based on second-generation cephalosporins, was changed to a single-shot application before surgery as postulated from Berrios-Torres et al. [27], Allegranzi et al. [28], and Davey et al. [29].
Guideline adherence was attained by teaching workshops as well as dissemination of electronic and laminated editions of the guideline. Additionally, continuous interdisciplinary ward rounds discussing all patients receiving antibiotic agents led to an immediate and substantial reduction in antimicrobial use. These meetings resulted in a feedback loop involving the responsible surgeon. We observed an increase in effectiveness in reducing the administration duration of second-generation cephalosporins as suggested in the Infectious Diseases Society of America (IDSA) guidelines as one of the main objectives [9] for AMP in aseptic surgeries.
Among the high-risk antibiotic agents, the second strongest reduction was in clindamycin, with a reduction of 78% (pre-intervention level [Q10], 18.982 DDDs/100 PDs; post-intervention level [Q17], 4.216 DDDs/100 PDs; quotient Q17–Q10, 0.222; p < 0.001). Compared with the post-intervention decrease in second-generation cephalosporin prescription rates, we detected a substantial decrease in clindamycin prescription rates. These findings far exceeded the rates published in other studies. Yoshida et al. [30] detected a clindamycin reduction of 43.4% (3.87 DDDs/1,000 PDs pre-intervention to 2.19 DDDs/1,000 PDs post-intervention) in a large cohort of 50,970 patients treated by physicians in different medical subspecialties in their study on an “out of control situation” concerning the use of clindamycin in Japan. The difference in the reduction rates may be attributable to the subspecialty of the patients in our cohort.
As mentioned previously, our cohort represented patients in a supra-regional orthopedic department that specialized in the treatment of PJIs. Historically, clindamycin was commonly used in German orthopedic wards because of its pharmacokinetics, with high concentrations in the bone structure and joints exceeding the minimum inhibitory concentrations (MICs) of most gram-positive pathogens responsible for surgical orthopedic infections [31–33] However, the disadvantages of clindamycin as a high-risk agent for CDI have not received attention by orthopedic surgeons in recent decades [34]. Moreover, for implant-associated infections, bactericidal antibiotic agents are preferred, and clindamycin as a bacteriostatic agent is not the first-choice recommendation for PJIs [5]. According to the published recommendations, antibiotic regimens were regularly established for each patient with PJI by the interdisciplinary team to achieve the best patient outcomes in the post-intervention period. This automatically changed the antibiotic policy and led to reduced antibiotic use and the decreased application of clindamycin.
The reduction in fluoroquinolones was much less impressive than the reduction in second-generation cephalosporins. We detected a quasi-stable pre- and post-intervention prescription rate, as shown in Table 2. There are different reasons for this finding: fluoroquinolones do not play an important role in orthopedic surgery in the pre-intervention period, but they become much more important in the post-intervention period as part of a specialized oral antibiotic combination including rifampin, especially for the treatment of staphylococci in the debridement, antibiotic, and implant retention (DAIR) scheme, and in one-stage exchanges and in two-stage exchanges after reimplantation of the new prosthesis [5,35,36]. Moreover, ciprofloxacin plays an important role in the eradication of implant-associated infections caused by gram-negative bacteria.
A main factor supporting the change in antibiotic policy was regular interdisciplinary ward rounds to establish antibiotic regimens for patients with infections. Because the studied department specialized in the treatment of PJIs, the effect of antibiotic use reduction because of the intervention was counterbalanced by this fact. However, the treatment policy for urinary tract infections, the most common pre-intervention reason for fluoroquinolone administration in orthopedic surgery, was changed by the ABS team. Differentiation between bacteriuria and real infection was emphasized, and in proven infections, substances other than fluoroquinolones were preferably administered, if possible.
As expected, we detected an increase in penicillin consumption, especially narrow-spectrum penicillins, which was threefold increased from 7.692 DDDs/100 PDs pre-intervention (Q10) to 29.071 DDDs/100 PDs post-intervention (Q17) (quotient Q17–Q10, 3780; p < 0.001) and aminopenicillins, which was six-fold increased from 6.225 DDD/100 PDs pre-intervention (Q10) to 38.547 DDDs/100 PDs post-intervention (Q17) (quotient Q17–Q10, 6.192; p < 0.001). Similar results for narrow-spectrum penicillins were detected by Borde et al.18 with a pre-intervention level of 48.2 DDDs/100 PDs that increased to post-intervention level of 124.3 DDDs/100 PDs. Our study was able to demonstrate the substantial potential of ABS interventions in an orthopedic special surgery ward.
A reduction in CDI rate from 0.031/100 PDs pre-intervention (Q10) to 0.011/100 PDs in the post-intervention period was detected. In the pre-intervention period, the rate of CDI in the cohort was already reduced by 46% (quotient Q10–Q1, 0.544; p = 0.460). This was a general trend not obviously affected by the implementation of the ABS policy. However, this steadily decreasing trend remained stable over the entire observed period. Compared with other studies, a generally low CDI rate might explain the absence of an effect on the incidence of CDI [23,37]. An average of 6.6/10,000 PDs was reported by the national German surveillance system [37]. Aldeyab et al. [23] described a pre-intervention CDI rate of 0.8/1,000 PDs in their cohort in Northern Ireland. Price et al. [37] detected a substantial decrease from a pre-intervention rate of 1.30/1,000 PDs to a post-intervention rate of 0.69/1,000 PDs in a large cohort of 200,245 admissions in Great Britain. Moreover, with 50.161 PDs our cohort was relatively small compared with those in large CDI studies that included more than 200,000 admissions [37].
Conclusions
In conclusion, the presented research assessed the positive impact of an intensified ABS program in an orthopedic department specializing in the treatment of PJIs. The ABS program reduced the total amounts of antibiotics following the key objectives of optimized antimicrobial therapy with good clinical outcomes. The effect of ABS interventions on CDI rates was not incisive in our study. However, a pre-intervention decreasing trend of CDI could be maintained in the post-intervention period. Antibiotic stewardship programs are well suited to prevent antimicrobial overuse and thereby reducing the risk for CDI in orthopedic surgery patients.
Footnotes
Authors' Contributions
Conceptualization: Feihl, Mühlhofer, Querbach. Methodology: Mühlhofer, Feihl, Querbach, Busch, von Eisenhart-Rothe. Software: Hapfelmeier, Pohlig. Validation: Mühlhofer, Pohlig, Gebhardt. Formal analysis: Hapfelmeier, Busch, von Eisenhart-Rothe, Gebhardt. Investigation: Feihl, Querbach, Mühlhofer. Resources: Pohlig, von Eisenhart-Rothe, Busch. Data curation: Gebhardt, Querbach, Hapfelmeier. Writing—original draft preparation: Feihl, Mühlhofer, Querbach, Pohlig. Writing—review and editing: Pohlig, Hapfelmeier, Busch, von Eisenhart-Rothe. All authors have read and agreed to the published version of the article.
Funding Information
This research received no external funding
Author Disclosure Statement
The authors declare that they have no financial or non-financial competing interests.
The Institutional Review Board at the Klinikum rechts der Isar approved the study (Faculty of Medicine, Technical University Munich, 507/19 S-SR).
All investigations were conducted in conformity with ethical principles.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.