
Abstract
Background:
Breast implant placement is a common operation performed by plastic surgeons, with more than 78,664 implant-based breast reconstructions carried out in the United States in 2016. Infection is a major concern for the reconstructive surgeon, with rates estimated at 2%–4% for implant exchanges. Use of peri-operative antibiotics is variable and provider dependent and is not without risk.
Methods:
Charts for all women undergoing mastectomy and immediate reconstruction at our institution from July 1, 2011–January 1, 2020 by a single plastic surgeon were reviewed. Patient characteristics, operative technique, and history of radiation, chemotherapy, hormonal treatment, and antibiotic protocols were collected for each patient. The data were analyzed using χ2 and Student t-tests.
Results:
Chart review was performed for 234 consecutive patients undergoing exchange of breast implants. Patients received only a single dose of peri-operative antibiotics before the first incision without post-operative antibiotics. In these patients, a total of 407 implant exchanges occurred. Post-operative cellulitis was found in 13 instances in 12 patients (infection rate of 3.1%) and was treated successfully with oral antibiotics in 11 of 13 cases. Two patients required operative washout (0.04%). Most of the infections (69%) were found on the side of the cancer. Patients experiencing post-operative infections were more likely to have had adjuvant chemotherapy (p = 0.007) than patients without infection. There was no significant difference between the two groups with regard to neo-adjuvant chemotherapy, radiation to the affected breast, or hormonal therapy or in terms of age, Body Mass Index, or the presence of diabetes mellitus. Intra-operative povidone–iodine (Betadine) swabbing and antibiotic selection did not have an impact on infection risk.
Conclusions:
A single dose of antibiotics results in sufficiently low rates of infection in patients undergoing breast implant exchange. Adjuvant chemotherapy is a clinically significant risk factor for infection in these patients.
Exchange of breast tissue expanders for permanent implants after mastectomy is one of the most common operations performed by plastic surgeons. Implant-based breast reconstruction accounts for more than 70% of breast reconstructions globally with more than 78,000 implant-based breast reconstructions performed in the United States alone in 2016. Globally, 81% of all breast reconstructions are implant based.
Infection is a common complication associated with these procedures with rates of infection estimated at 2%–4% nationally for implant exchange procedures and is thought to be attributable to contamination of the breast prosthesis with endogenous flora during surgery [1,2]. Once implants are colonized, symptomatic infection can ensue because of the formation of biofilms, most commonly within the first month after surgery [3,4]. Patients typically present with breast pain, swelling, and erythema with or without fever and purulent drainage, symptoms that may reflect superficial cellulitis or deeper implant infection, although the two are hard to distinguish. The most common pathogens associated with implant infections are gram-positive organisms such as Staphylococcus aureus, coagulase-negative Staphylococcus, Streptococcus, and Propionibacterium [2].
Antibiotic use, despite its commonality, is not without risk. Overall, approximately 50% of patients in the inpatient setting receive at least one dose of antibiotics during their hospitalization, with an estimated 20%–30% of administered antibiotic therapy considered to be unnecessary [6]. In breast implant surgery, a 2009 survey of members of the American Society of Plastic Surgeons illustrated that 72% of plastic surgeons surveyed prescribed a course of antibiotics after breast reconstruction, continuing for at least one week or until drains were removed [7]. This is a clear contradiction to the available evidence that suggests that no additional benefit of antibiotics or decrease in infection rate is found in patients undergoing breast reconstruction who receive more than 24 hours of post-operative antibiotics and that a single peri-operative dose results in infection rates similar to those of more prolonged courses [5].
As even a single dose of antibiotics can lead to adverse drug events, allergic reactions, end-organ toxicity, bacterial resistance, and Clostridium difficile infections—all of which can carry significant morbidity—it is especially important that we identify areas in which antibiotics are being over-used [7]. Antibiotic-associated adverse drug events occur in as many as 20% of hospitalized patients receiving at least 24 hours of any parenteral or oral antibiotic therapy and most commonly manifests as gastrointestinal, renal, or hematologic abnormalities [7].
Additionally, antimicrobial resistance is a growing concern that can lead to a delay in administration of effective antibiotics resulting in inferior patient outcomes. Further, these resistant organisms require the use of more potent and toxic drugs, which can cause further patient harm [8]. Antibiotic-resistant “superbugs” are becoming increasingly difficult to eradicate, a problem that is furthered by the dearth of new antimicrobial drugs with bactericidal activity against gram-negative bacteria and enterococci [9]. Published data have shown a positive association between antibiotic-resistant bacterial infections and adverse outcomes including an overall increase in the mortality rate of 1.3–2-fold [8]. In addition to adverse patient outcomes, mean hospital charges are significantly higher for patients with multi-drug–resistant (MDR) infections, specifically methicillin-resistant Staphylococcus aureus (MRSA), compared with those with non-resistant infections.
In a 2012 systematic review of the literature, several factors were identified as increasing the risk of surgical site infection in patients undergoing placement of breast implants: Pre-operative factors included elevated Body Mass Index (BMI), diabetes mellitus, smoking, post-menopausal status, history of breast operations, and increased American Society of Anesthesiologists (ASA) class. Operative factors such as increased duration of the operation, lymph node dissection, higher estimated blood loss, and need for surgical drains were noted in addition to post-operative factors such as elevated serum glucose concentration and the presence of seroma or hematoma [2]. Importantly, appropriate peri-operative antimicrobial prophylaxis and skin antisepsis techniques were associated with a lower infection risk [2].
While peri-operative antibiotic regimens are associated with lower rates of infection in patients undergoing placement of breast implants, there is significant variability across practitioners with regard to the duration of post-operative antibiotic regimens, as prior prospective studies have failed to elucidate an optimal routine. In a 2013 systematic review including 14,947 patients by Phillips et al., the authors concluded that no additional benefit was found in patients undergoing breast reconstruction who received more than 24 hours of post-operative antibiotics and that a single peri-operative dose resulted in infection rates similar to those seen with more protracted courses [5]. Despite these promising data, the majority of reconstructive surgeons still prescribe more than a single dose of peri-operative antibiotics in patients who undergo surgery for placement of permanent breast implants. In this study involving more than 400 breast implant placement procedures, however, all patients received just a single dose of antibiotics without any prophylactic post-operative antibiotics being given. Accordingly, this study aimed to illustrate the sufficiently low risk of infection in patients receiving only a single dose of antibiotics and similarly to address patient- and surgery-related risk factors that may predispose patients to a higher risk of infection. Given the exceedingly high patient, hospital, and societal costs associated with prolonged antibiotic therapy, this study aimed to advance further the paradigm of judicious antibiotic administration for patients undergoing exchange of tissue expanders for permanent breast implants after mastectomy and to encourage reconstructive surgeons to decrease the duration of antibiotic therapy to a single dose of in this patient population. In this retrospective chart review, we hypothesized that a single dose of peri-operative antibiotics results in a sufficiently low rate of infection and that prolonged antibiotic therapy is not necessary for patients undergoing placement of permanent implants for breast reconstruction.
Patients and Methods
Data were collected through a retrospective chart review of all patients who underwent placement of permanent breast implants at a single plastic surgeon's practice between July 1, 2011, and January 1, 2020. Current Procedure Terminology (CPT) codes 19340 and 19342 were used to identify appropriate patients who underwent either implant exchange or direct-to-implant procedures. Demographic information, medical oncologic management, peri-operative procedures, antibiotic use, and post-operative complications were collected for each patient. Demographic information included date of birth, patient age, Body Mass Index (BMI), medical co-morbidities including history of diabetes mellitus, immunosuppression, cancer therapy, hormonal therapy, and neoadjuvant and adjuvant radiation. All patients are being followed indefinitely with frequent visits in the first 3 months after surgery, followed by biannual visits and visits annually thereafter for life.
Data were collected regarding the type and dosing of pre-operative prophylactic antibiotics for each patient, whether the patient was prepared with chlorhexidine gluconate (ChloraPrep) or povidone–iodine (Betadine), whether intra-operative antibiotic irrigation was used, and if intra-operative Betadine swabbing was performed. Peri-operative antibiotic use was defined as a single pre-operative dose in the operating room before the first incision. Post-operative antibiotic use was defined as antibiotics given after completion of the procedure as either prophylactic or therapeutic doses. Infectious complications were defined as cellulitis or other signs of incision infection requiring therapeutic intervention such as surgical washout and explant, interventional radiology drainage, or antibiotic therapy. Cellulitis was defined as post-operative erythema that required antibiotic treatment.
Descriptive statistics were used to characterize the patient population and rates of infection with subsequent rates of complications calculated across the cohort. A two-tailed Student t-test was used to conduct univariable analyses of demographic data and medical comorbidities, and χ2 tests were used to conduct multivariable analyses on medical co-morbidities, medical oncology treatment characteristics, and peri-operative treatment. The results of the analyses are reported with p values; a value of <0.05 being the cut-off for statistical significance. Rates of infection and subsequent complications were calculated across the population.
Results
During this nine-year period, 234 women underwent permanent implant placement with a total of 407 implant exchanges or direct-to-implant procedures being performed. All patients had a history of mastectomy for breast cancer treatment or prophylaxis. No patients in this cohort had drains placed during surgery per attending surgeon preference. The mean age at surgery was 50.49 years. Immediately prior to implant exchange or direct-to-implant surgery, all patients received a single dose of cefazolin (Ancef) (n = 196) except for those with a penicillin allergy, in whom clindamycin was administered (n = 26). Three patients had allergies to both drugs and received either gentamicin or cefoxitin, and in nine patients, the antibiotic was unspecified. None of the patients received post-operative prophylactic antibiotics.
During surgery, 198 of 234 patients underwent Betadine swabbing of the affected breast(s). Both types of antibiotic used (Ancef versus clindamycin) and use of a Betadine swab did not affect the risk of post-operative infection (p = 0.677 and p = 0.899, respectively).
Post-operative cellulitis occurred in 13 breasts in 12 patients for an overall infection rate of 3.19%. One of these 12 patients experienced bilateral infection. Of the 13 infected breasts, two required surgical washout and one required interventional radiology drainage. In the remainder, cellulitis resolved with a course of oral antibiotics alone; no antibiotic-related adverse events were noted in this cohort (Table 1).
Post-Operative Complications of Patients Undergoing Permanent Implant Placement
Comparing the infected group with the remainder of the patients in this study, mean age, BMI, and the presence of diabetes mellitus were similar across the two cohorts (mean age 50.49 years for entire cohort, mean age 50.92 years for infections cohort; p = 0.943), BMI (mean 24.39 for entire cohort, mean 24.46 for the infections cohort; p = 0.715), or diabetes mellitus (p = 0.336).
In the treatment for breast cancer, 43 patients received neoadjuvant chemotherapy, 60 received adjuvant chemotherapy, 131 received hormonal therapy, 43 received neoadjuvant radiation therapy (defined as any radiation to the affected breast prior to implant placement surgery), and 31 patients received adjuvant radiation therapy. Among these therapeutic regimens, only adjuvant chemotherapy was found to be a statistically significant risk factor for developing post-operative cellulitis (p = 0.008) (Table 2; Fig. 1).
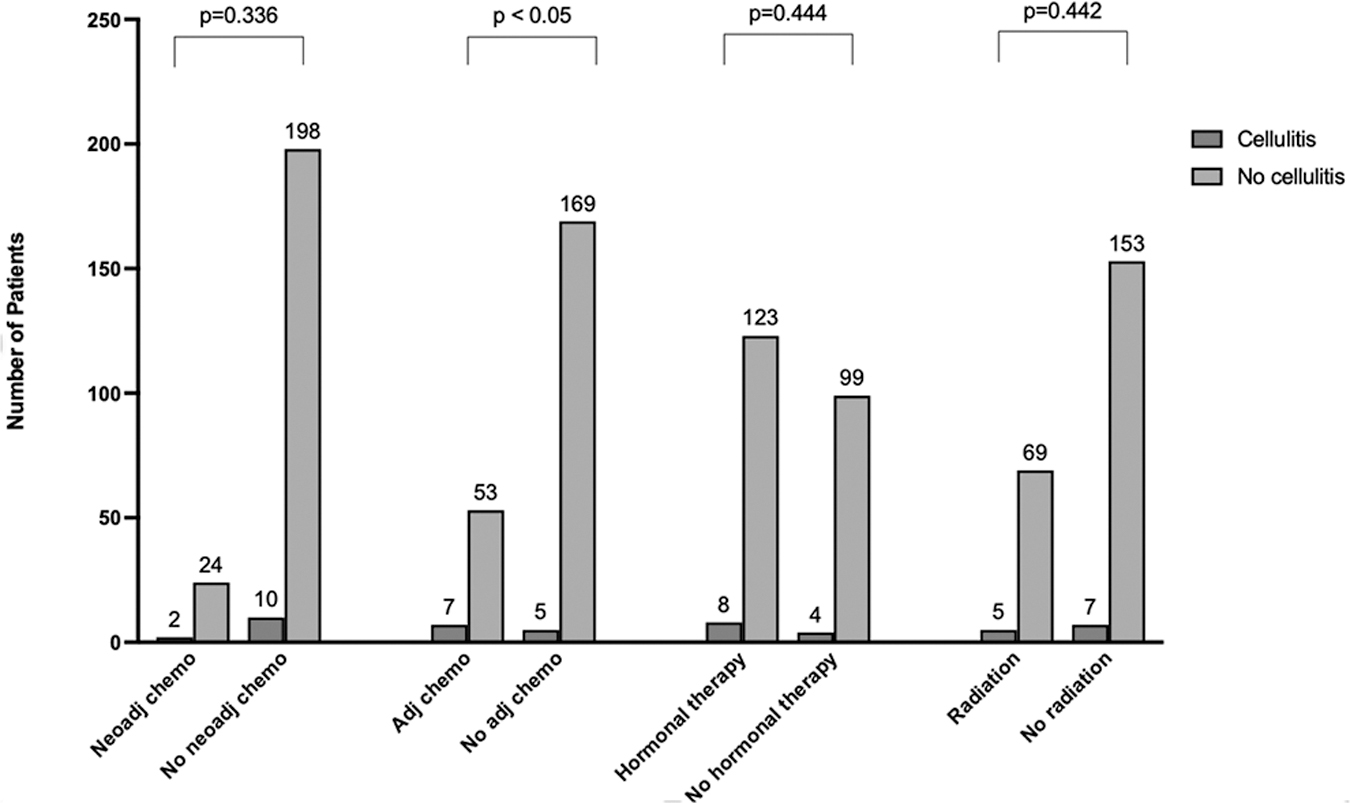
Risk factors for cellulitis according to oncologic treatment.
Correlation between Cellulitis and Type of Oncologic Treatment
Discussion
A single dose of pre-incision antibiotics is associated with a decreased incidence of post-operative wound infections in reconstructive breast implant surgery [5,6]. However, the evidence concerning the role of extended courses of post-operative antibiotics to reduce the rate of infection after breast implant surgery is far less conclusive. Rather, the data suggest that prolonged courses of antibiotics do not confer any further reduction in the risk of infection. Instead, these therapies can be associated with adverse drug reactions, allergic reactions, bacterial resistance, and C. difficile colonization in as many as 5% of breast surgery patients [8].
Concern for antibiotic resistance has increased in recent years because of widespread drug use. There is a growing prevalence of multi-drug–resistant organisms, some of which are resistant to nearly all or even all available antibiotics, and the major problem contributing to the emergence of resistant bacteria is the misuse and overuse of antibiotics [10]. The Centers for Disease Control and Prevention (CDC) estimates that more than 2 million people annually in the United States experience multi-drug–resistant infections and that at least 23,000 of these people die as a direct consequence of these infections [13]. Antimicrobial resistance also can adversely affect patient outcomes by enhancing virulence which may delay or limit possible available therapies [11].
Further, in a 2009 study by Roberts et al. evaluating both the economic and clinical outcomes of antimicrobial resistance, the authors noted that in a sample of nearly 1,400 patients, 188 patients (13.5%) experienced an antimicrobial drug-resistant infection during admission with associated medical costs ranging from $18,588 to $29,069 per patient with hospital stays increasing by somewhere between 6.4 and 12.7 days. The mortality rate was 6.5% in this group, with overall societal costs of $10.7–$15.0 million [7].
Similarly, a 2017 retrospective review from Johns Hopkins Medical School of 5,579 patients illustrates the widespread prevalence of antibiotic administration and its associated consequences. Of these patients, 1,488, or 27%, received antibiotics for 24 hours or longer with 298 of these patients (20%) experiencing an adverse drug effect (ADE), an overall antibiotic-associated ADE rate of 22.9 per 10,000 person days [7]. Of these ADEs, 27%, or 88 cases, occurred after hospital discharge, indicating that the risk persists beyond the course of hospitalization. In a 2009 retrospective review of 363 patients undergoing breast surgery who received post-operative antibiotic prophylaxis, 15, or 4%, had an antibiotic-related complication with diarrhea, nausea/vomiting, and rashes being most frequently reported. In this study, there was a significantly higher rate of drug-related adverse events among patients who received a course of antibiotics for post-operative prophylaxis compared with those receiving only a single pre-operative dose, with increasing risk associated with longer durations of prophylactic treatment. Extended periods of treatment were related to higher rates of C. difficile colitis with two patients in this study experiencing C. difficile from their post-operative antibiotic regimen alone. However, the authors of this study noted that antibiotic-related complications were uncommon after a single pre-operative prophylactic dose [10].
In our retrospective chart review, patients undergoing breast implant exchange who received a single dose of antibiotics before the first incision experienced rates of infection close to or lower than the national average of 3%–4% for this procedure at 3.19%. Of those who did experience infection, most had their cellulitis resolve with a course of antibiotics alone, with only three patients requiring invasive procedures (interventional radiology drain placement or surgical washout with implant removal). The overall percentage of patients requiring any type of invasive therapy for treatment of infection was 0.73%, and the rate of implant failure was 0.49% in this cohort. These low rates of complications demonstrate that rates of infection are sufficiently low when a single pre-operative dose of broad-spectrum antibiotics is administered prior to the first incision and serve to reiterate the fact that additional antibiotics are unnecessary in reducing risk of post-operative complications and infections. These data are congruent with those of a 2014 retrospective matched cohort study whereby patients receiving a single dose of pre-operative antibiotics experienced rates of post-operative incision infection similar to that of those who had received post-operative antibiotic prophylaxis with cefalexin (Keflex) until drain removal. In the group receiving only a single dose of peri-operative antibiotics, 94 patients (who collectively underwent a total of 308 implant/tissue expander placements) experienced 11 infections (12%). This is comparable to the other group (94 patients with 297 total implants) who received antibiotic prophylaxis until the drains were removed, among whom 9 infections (10%) were noted. There was no statistically significant difference between these cohorts (p = 0.8) [11].
Age, BMI, and the presence of diabetes mellitus did not influence the risk of infection in our study. This is consistent with the current literature whereby there is a lack of consensus as to whether these factors contribute to an greater risk of surgical site infection [12]. In a 2013 retrospective review by Reich et al. published in Plastic and Reconstructive Surgery, there was no difference in the rate of infection with respect to BMI or age in patients undergoing implant-based reconstruction. However, radiation was associated with a higher risk of post-operative breast cellulitis [13]. In our study, breast radiation of any kind was not associated with an increased risk of infection.
When evaluating patient- and surgery-related risks and protective factors, the only significant risk factor found for post-operative breast infection in this cohort was adjuvant chemotherapy. This coincides with the conclusions of a 2010 retrospective review by Peled et al., which similarly concluded that the highest rate of surgical site infection was found in the group receiving adjuvant chemotherapy compared with neoadjuvant chemotherapy or no chemotherapy at all [14]. Several theories exist as to why this correlation may exist, and several experimental animal models have demonstrated decreased wound strength and impaired wound healing after administration of chemotherapy, especially when given in the early post-operative period [15]. In a landmark study by Devereux et al. published in Cancer in 1979, doxorubicin (Adriamycin) was reported to significantly impair wound healing in a mouse model when given during the early post-operative period [16].
Given the risk of harmful side effects and development of bacterial resistance associated with prolonged antibiotic therapy, this study supports the practice of conservative antibiotic stewardship, whereby antibiotics are used sparingly as a single peri-operative dose prior to the first incision. This study reiterates much of the current literature, which describes no additional benefit to prolonged prophylactic antibiotic therapy. Further, our data suggest that adjuvant chemotherapy may portend a greater risk of post-operative infection. This should alert surgeons pre-operatively to the heightened risk of infectious complication in this patient population. Further inquiry on this subject is indicated to evaluate whether this high-risk group of patients would benefit from a prophylactic course of antibiotics after weighing the not insignificant risk of antibiotic-associated morbidity.
As a retrospective chart review of a single surgeon's practice, this study has inherent limitations related to its design and the relatively small cohort. Further study is needed to define conclusively the patient populations who may be at risk for post-operative infectious complications following mastectomy and implant-based reconstruction to identify these patients early in order to minimize and mitigate risk.
Footnotes
Funding Information
No funding was received for this work.
Author Disclosure Statement
No competing financial interest exist. The authors received no funding for the writing of this manuscript.