
Abstract
Background:
Biliary instrumentation is associated with bactibilia and post-operative infection. Bactibilia incidence over time remains unknown.
Patients and Methods:
Consecutive patients with bilioenteric anastomosis surgery and available surveillance intra-operative bile duct cultures were evaluated for post-operative infection. The study period (2008–2019) was divided into quartiles to examine time-based trends.
Results:
Among 101 cases, 60 intra-operative bile duct cultures had no growth and 41 patients had documented at least one culture-positive isolate in their bile. Frequency of patients with culture-positive intra-operative bile increased over the study period (period 1, 1/28, 3.6% vs. period 2, 7/21, 33.3% vs. period 3, 15/26, 57.7% vs. period 4, 18/26, 69.2%; p < 0.001). Culture-positive post-operative infection (17/101; 16.8%) was not associated with intra-operative bile duct culture (p = 0.552), however, the same micro-organism isolate was identified on post-operative infection and intra-operative culture of bile duct bile among six of 17 patients (35.3%).
Conclusions:
We found an increasing incidence of bactibilia and post-operative culture-positive infections over the last decade. One-third of patients with a positive intra-operative bile duct culture experienced post-operative infection with the same organism, yet a clear link between bile colonization and post-operative infection was not established.
Bactibilia is an important driver of perioperative complications in operations involving the common bile duct [1–7]. A higher incidence of complications was observed among patients with previously instrumented bile duct who underwent pancreatoduodenectomy [8], and bactibilia was more commonly found in the instrumented patient population [1,4]. Peri-operative infectious morbidity of complex biliopancreatic surgery remains high despite strategies aimed to decrease surgical site infections, including prolonged systemic antibiotics [2,9–11] and wound protectors [12].
Prior studies that evaluated bactibilia during pancreatoduodenectomy were done over a relatively short time span, and often included multi-institutional data [3,7,13,14]. A study evaluating bactibilia incidence over a longer time period is needed as reported incidence of nosocomial infections has changed [15] and reports on endoscopy-related infections have increased [1,16].
We hypothesized that biliary bacterial and fungal colonization and subsequent peri-operative infection rates increased over time [15]. Our main objective was to analyze changes of surgically collected surveillance bile duct microbial isolates over a decade of our clinical practice. Furthermore, we analyzed the relation of intra-operative biliary culture isolate to post-operative frequency of clinically indicated cultures (a surrogate measure of clinical suspicion for infection) and culture-positive surgical site infection rate.
Patients and Methods
This is a retrospective longitudinal study approved by our Institutional Review Board (DM2020-48) and its reporting adheres to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guideline. Patients undergoing hepaticojejunostomy between July 2008 and June 2019 with available intra-operative bile duct cultures were included. Intra-operative bile cultures were routinely collected on all patients since 2019, at the time of planned bile duct transection during pancreatoduodenectomy or isolated hepaticojejunostomy, based on our empiric observation of turbid and purulent bile among patients with prior biliary instrumentation. Demographic and clinical characteristics of these patients along with information on prior biliary instrumentation (endoscopic retrograde cholangiopancreatography [ERCP] ± stenting, percutaneous transhepatic cholangiography [PTC]) was collected. For cases in which there were multiple interventional procedures on the bile duct prior to resection, we analyzed type and date of the initial but not subsequent procedures, however, we included the total number of preoperative biliary instrumentations.
The studied time period was approximated into quartiles based on the number of completed cases: period 1 (2008–2010), period 2 (2011–2012), period 3 (2013–2015), and period 4 (2016–2019). Sensitivity analysis was performed by dichotomizing the study duration into early (2008–2012) and late periods (2013–2019). All post-operative cultures were obtained as clinically indicated for a suspicion of infection. Thus, they serve as a proxy for suspicion of clinical infection, even if their final result is no growth. We subsequently compared the microbial profile of intra-operative isolates versus post-operative isolates. Results are expressed as a frequency and proportion of bacterial isolates. Days until post-operative culture order were analyzed using the Kaplan-Meier method. Categorical data are expressed as proportions (tested by χ2 or Fisher test as appropriate). Continuous variables are conveyed as mean ± standard deviation (difference tested by Mann-Whitney test). All analyses were performed using STATA version 15 (StataCorp LP, College Station, TX). p < 0.05 was considered statistically significant.
Results
There were 101 patients who underwent pancreatoduodenectomy (n = 94) or extrahepatic bile duct resection (n = 7) that had intra-operative culture obtained during planned bile duct transection (Table 1). Sixty intra-operative bile duct cultures did not grow any organisms, whereas 41 patients had culture-positive isolates. Frequency of patients with culture-positive intra-operative bile increased over the study period (period 1, 1/28, 3.6% vs. period 2, 7/21, 33.3% vs. period 3, 15/26, 57.7% vs. period 4, 18/26, 69.2%; p < 0.001; Fig. 1). When the study time was dichotomized into early and late periods, the rate of bile colonization increased significantly (2008–2012, 8/49 cases, 16.3% vs. 2013–2019, 33/52 cases, 63.5%; p < 0.001). Similarly, we also found increased frequency of post-operative culture-documented infections (period 1, 0/28, 0% vs. period 2, 6/21, 28.6% vs. period 3, 9/26, 34.6% vs. period 4, 2/26, 7.7%; p = 0.002; Fig. 2). When analyzed by early versus late period, post-operative infections (6/49 cases, 12.2% vs. 11/52 cases, 21.1%; p = 0.232) were not statistically more common in the later period. Proportion of patients with pre-operative biliary intervention has not changed on the study period (Table 1).
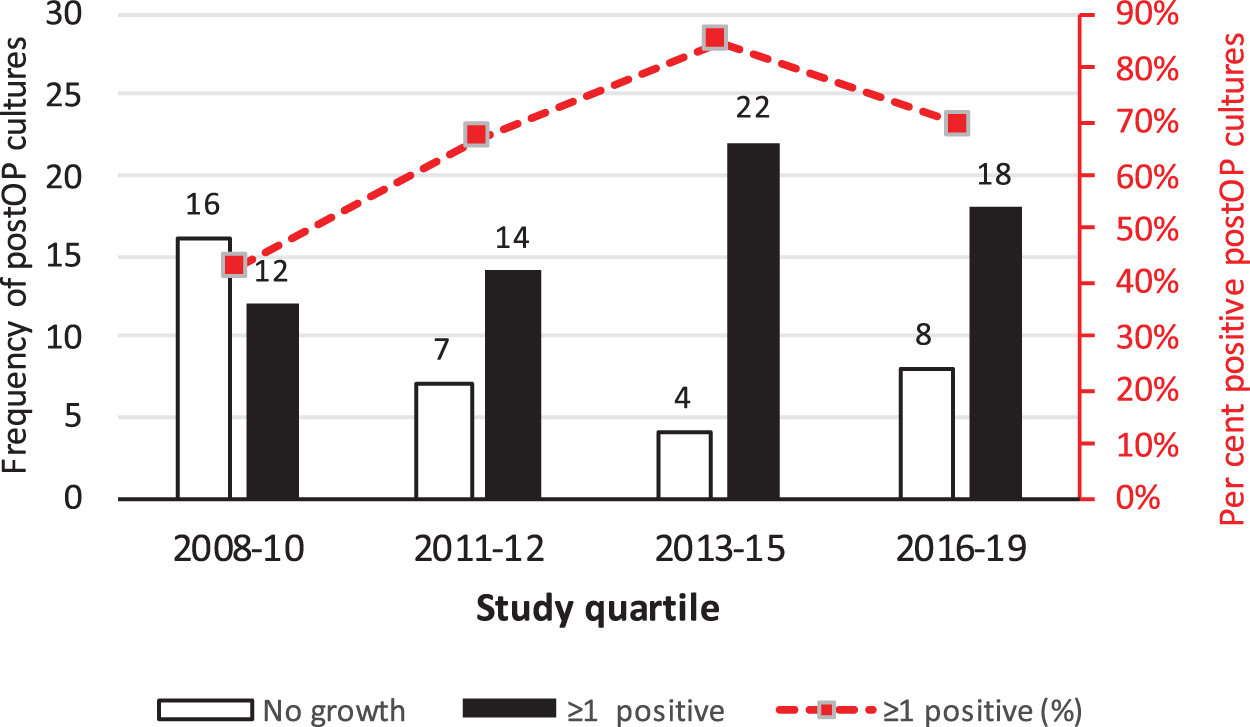
Intra-operative cultures of common bile duct bile over the study period divided into quartiles. Frequency of cultures with no growth has decreased (open bars) while the frequency of cultures with at least one isolate increased (closed bars). Dashed red line indicated percentage of culture positive bile and relates to the secondary y-axis on the right (Pearson χ2 test p < 0.001).

Post-operative cultures of any site over the study period divided into quartiles. Frequency of cultures with no growth has decreased (open bars) while the frequency of cultures with at least one isolate increased (closed bars). Dashed red line indicated percentage of cases with any culture-positive postoperative occurrence and relates to the secondary y-axis on the right (Pearson χ2 test p = 0.013).
Characteristics of Study Participants by Study Period
p for trend is calculated as appropriate for continuous data. Biliary intervention–pre-operative instrumentation of bile duct by endoscopic or percutaneous means, with or without stenting.
CBD = common bile duct; ASA = American Society of Anesthesiologists.
Culture-positive post-operative surgical site infection (SSI) was observed among 17 patients (16.8%) and was not associated with intra-operative bile duct culture. There were nine of 60 (15.0%) SSIs among 60 patients with no growth on intra-operative common bile duct bile culture versus eight of 41 (19.5%) SSIs among those with culture-positive intra-operative isolate from bile duct (p = 0.552). There was no difference in patient age (65.4 ± 12.1 vs. 62.0 ± 12.9 years; p = 0.292), duration of operation (475 ± 91 vs. 449 ± 119 minutes; p = 0.359), or duration of indwelling biliary stent (79.2 ± 83.3 vs. 115.8 ± 171.1 days; p = 0.675) between those without and with SSI, respectively. There were six patients (35.3%) who experienced post-operative culture-positive infection with the micro-organism identified on the intra-operative culture of bile duct bile (Fig. 3). The remaining patients did not demonstrate this association.

Venn diagram of overlap between intra-operative (OP) bile culture and surgical site infection (SSI) by micro-organism. CNS = central nervous system; MRSA = methicillin-resistant Staphylococcus aureus.
Thirty-one patients had no pre-operative bile duct instrumentation and the remaining 70 had at least one instrumentation (Table 1). There was a strong positive relation between pre-operative biliary intervention and culture-positive isolate (both intra-operative surveillance culture and post-operative infection). Culture-positive intra-operative bile duct isolate was identified among three of 31 (9.7%) non-instrumented patients, but was higher (38/70, 69.3%; p < 0.001) among those with at least one pre-operative biliary instrumentation. In respect to 17 culture-positive post-operative SSIs three of 31 (9.7%) post-operative infections were among those with no biliary intervention compared with 14 of 70 (20%; p = 0.257) among those pre-operatively instrumented. There was no age difference between patients with and without pre-operative biliary instrumentation (65.8 ± 11.8 vs. 62.6 ± 13.1 years; p = 0.287) or number of positive post-operative cultures for any indication (4.1 ± 13.1 [median 0; interquartile range {IQR}, 0–3] vs. 2.1 ± 4.2 [median 0; IQR, 0–3]; p = 0.670). There was a single 30-day peri-operative mortality occurring on day 16 after pancreatoduodenectomy with unplanned mesenterico-portal vein reconstruction (1/94 pancreatoduodenectomies, 1.1%). This patient experienced multiorgan failure associated with sepsis caused by a micro-organism identified intra-operatively in the patient's bile (vancomycin-resistant enterococcus).
*
Micro-organisms identified both in bile and in post-operative infection include Pseudomonas, Enterococcus (both vancomycin-sensitive and vancomycin-resistant), Klebsiella, Escherichia coli, and α-hemolytic streptococcus (Fig. 3). Among 11 patients who experienced post-operative infection not predicted by intra-operative bile culture, post-operative culture yielded Citrobacter, Staphylococcus (both coagulase-negative and methicillin-resistant), and Candida albicans. One of these 11 patients had culture-positive bile (Enterobacter and Klebsiella), not identified in post-operative SSI cultures (Enterococcus, Streptococcus, and Candida albicans).
Initial biliary instrumentation procedure was PTC (n = 6), ERCP with stent (n = 52), or ERCP without stent (n = 12). Among 52 cases with pre-operative ERCP-placed internal biliary stents as their first biliary intervention, 34 were plastic stents and 14 were self-expanding metal stents, whereas the character of four remaining stents was unknown. There was no age difference among patients receiving different types of initial biliary intervention, but there was a substantial difference in diagnosis to operation time (PTC 20.6 ± 14.1 days vs. endobiliary stent 106.3 ± 113 days; p < 0.001). Duration of biliary stenting prior to biliopancreatic surgery was not related to number of bacterial isolates (Supplementary Figure S1).
There were 113 intra-operative microbiologic isolates among 101 completed cases (Fig. 4 and Supplementary Figure S2): 41 (36.3%) were gram positive, 51 (45.1%) were gram negative, and 21 (18.6%) were fungal. Forty-one (36.3%) isolates were aerobes, 55 (48.7%) facultative anaerobes, and 17 (15.0%) anaerobes. Most common isolates were Enterococcus, Candida, Klebsiella, and Streptococcus. There was no statistical difference in time until post-operative culture was ordered between patients with and without pre-operative biliary instrumentation (p = 0.793; Supplementary Figure S3), suggesting that other unmeasured characteristics may govern surgical infection risk.

Comparison of frequency of culture-positive micro-organism isolates from any post-operative culture (closed bars) compared with intra-operative (OP) bile duct cultures (open/yellow bars). Candida and Enterococcus are frequently found in intra-operative bile duct cultures and in post-operative cultures. Certain intra-operative isolates do not appear frequently in post-operative cultures (Bacteroides, Clostridium, Fusobacterium, Prevotella). SSI = surgical site infection.
Standard clinical laboratory protocols indicated 93 cultured isolates for further microbial sensitivity testing. We classified 67 as low-resistance isolates (resistance to ≤1 tested antibiotic). Another 24 isolates were resistant to two antibiotic classes, whereas two were resistant to three or more antibiotic classes. Among these 26 (28%) multi-drug–resistant isolates, six were vancomycin-resistant enterococci, two were extended-spectrum β-lactamase inhibitor Enterobacteriaceae, and two were multi-drug–resistant pseudomonades.
Discussion
Over the last decade we observed an increasing incidence of micro-organism isolates among patients undergoing biliopancreatic surgery, a finding not reported previously. Bactibilia has been associated with postoperative complications in several studies [3,6,8,17]. On the contrary, we have not demonstrated a clear and direct correlative relation of bactibilia to post-operative infection [4,5,7]. It remains plausible that relation of bactibilia and post-operative infection may be micro-organism–specific. For example, Enterococcus bile isolate was frequently found in post-operative SSIs, a finding in common with Maatman et al. [4]. Increased risk of infectious complications among those with prior biliary instrumentation is generally accepted [8,17], again with a limited evidence suggesting the contrary [18]. Post-operative complications in turn increase peri-operative mortality [3,8,17] as well as long-term survival after pancreatobiliary surgery [19]. Total rate of post-operative infections reported in this study (16.8%) is in agreement with prior reports based on National Surgical Quality Improvement Program (NSQIP) [18,20,21] or randomized trials [8,22].
Similar to other studies, we identified 40% of intra-operative bile duct cultures to have at least one micro-organism isolate, and 22% having three or more isolates [4,7,14]. Those with pre-operative biliary stents were at higher risk of post-operative infectious complications, a finding different from that of a decade-old study by Augenstein et al. [1], but consistent with a prior randomized trial of preoperative biliary stenting [8]. Counterintuitively, a culture-positive isolate from surveillance intra-operative bile duct culture was not clearly associated with a higher risk of post-operative infection. Furthermore, we did not identify a difference in rate of biliary colonization according to the type of biliary stent (PTC, metal vs. plastic biliary stent), although we acknowledge that our subgroup sample size may have been underpowered to detect such differences.
Similar to prior reports Escherichia, Klebsiella, Pseudomonas, and Enterococcus rank among the most common and clinically relevant organisms encountered in our study [2–4,10,14,16,23,24]. On the other hand, numerous anaerobic bacteria (Prevotella, Clostridium, Bacteroides, Fusobacterium) seen in the intra-operative bile duct cultures have not been associated with any post-operative infections in this study, suggesting that anaerobic bacteria do not pose a substantial risk of infection. Furthermore, Candida species was a common intra-operative bile culture result, but it did not transfer to a high risk of post-operative Candida infection or culture-positive isolate. Although not a subject of the present study, mycobiome has been recognized as a driver of pancreatic ductal oncogenesis [25] and Candida colonization may have non-infectious significance.
Our finding of increasing bile duct culture-positive isolates appears in line with nationally increasing multi-drug resistant isolates [15]. Mechanisms behind this rise of bactibilia remain unclear. We did not observe a change in proportion of pre-operative biliary intervention over the study period, yet nosocomial endoscope-related transmissions remain a plausible driving factor [1,16]. Other studies were designed with a shorter time frame, and consequently did not investigate change of bactibilia rate over time [2,4,5,10,14,26]. Some strategies to alter peri-operative infection including abdominal lavage and change in peri-operative antibiotic therapy did not result in reduced SSIs in some studies [5,14]. Prolonged peri-operative prophylactic antibiotic agents for five days, and subsequent intra-operative bile culture-driven extension to 10-day peri-operative treatment do appear to lower clinically apparent infection in some studies [9,13]. Other infection-reducing strategies relevant for pancreatobiliary procedures include wound protectors [12], and perhaps peri-operative probiotics [27,28].
Intra-operative biliary culture predicts only one-third of the organisms of subsequent post-operative culture-positive infections in this study. Other studies found a more consistent relation of intra-operative bile culture as the causative agent of post-operative infection [1,4]. Nevertheless, we will continue our practice of routine culture of bile, as a method of both surveillance and to identify multi-drug–resistant isolates, which in turn may inform subsequent antibiotic selection, should SSI occur [2,9,14]. We use a single-dose pre-operative antibiotic and have yet to adopt prolonged antibiotic therapy unless clinically evident infection is documented. Such approach is supported by the contemporary 2017 U.S. Centers for Disease Control Guideline for prevention of SSI, which calls for a single-dose pre-incisional antibiotic without redosing [29]. Although further research is needed to adjudicate risk-benefit of peri-operative antibiotic therapy rather than prophylaxis, this study along with several others support development of randomized trial examining this knowledge gap in pancreatoduodenectomy [1,2,4–6,9,26].
The retrospective nature of the present study carries several limitations, including potential biases. Furthermore, we have not accounted for surgical technique evolution over time nor for changes in antibiotic resistance in our institution. On the other hand, a certain consistency was provided by one surgeon conducting or participating in all operations. Given a modest sample size we did not differentiate among superficial surgical site, organ/space, or infection outside of surgical site in contrast to multi-institutional studies [20–22]. We used standard clinical microbiologic culture for isolate identification and characterization, although molecular and DNA-based microbiologic characterization is becoming more frequent. Furthermore, we have not distinguished between benign and malignant cases, whereas it has been shown previously that peri-procedural post-ERCP bacteremia is more frequent among patients with periampullary malignancy [10,23]. Last, we were not able to evaluate prior antibiotic exposure and prior episodes of biliary sepsis, both of which may influence emergence of multi-drug–resistant bacteria [10,14].
Conclusions
In summary, we observed an increasing incidence of bactibilia and post-operative culture-positive infections over the last decade despite unchanged rate of pre-operative biliary intervention. One-third of patients with positive intra-operative bile duct cultures experienced post-operative SSIs with the same organism. Nevertheless, we did not identify a clear link between bactibilia and post-operative infections.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.