
Abstract
Background:
To determine whether degree of anemia at sepsis onset is predictive of inflammatory cytokine trajectory, erythropoietin response, and recovery.
Patients and Methods:
Critically ill patients with sepsis were stratified into three groups based on initial hemoglobin (Hgb): Hgb <8 g/dL (severe); 8–10 g/dL (moderate); and >10 g/dL (mild). Granulocyte colony stimulating factor (G-CSF), interferon (IFN)-γ, tumor necrosis factor (TNF)-α, C-reactive protein (CRP), erythropoietin (EPO), and Zubrod scores were measured serially.
Results:
Thirty-four percent had severe anemia (Hgb, 7.2 ± 0.7g/dL), 35% had moderate anemia (Hgb, 9.1 ± 0.6g/dL), and 31% had mild anemia (Hgb, 11.3 ± 1.1g/dL). All groups experienced persistently high EPO levels without resolution of anemia. IFN-γ and CRP was persistently elevated in all groups. At three, six, and 12 months, the severe anemia group had higher Zubrod scores.
Conclusions:
Degree of anemia at sepsis onset was not associated with a difference in proinflammatory cytokine trajectory but was associated with a worse functional outcome. Despite initial elevated EPO levels, it did not correlate with resolution of anemia.
Multiple organ dysfunction syndrome (MODS) is progressive physiologic dysfunction of two or more organ systems causing a state of immunosuppression and altered metabolism [1]. It emerged in the late 1970s as a result of advances in intensive care that allowed patients to survive what would otherwise have been lethal injuries [1[. Despite tremendous advances in critical care, including the Surviving Sepsis Guidelines, MODS continues to be associated with substantial mortality and morbidity in the population with sepsis [2–4]. In recent years, far fewer patients die early following sepsis, and more patients experience ongoing immune dysregulation known as persistent inflammation, immunosuppression, and catabolism syndrome (PICS) [5]. Following sepsis, survivors either recover rapidly or develop persistent immune dysfunction along with chronic critical illness [6].
Anemia is a common complication of critical illness, whether secondary to traumatic injury or sepsis [7,8]. The etiology of this anemia is multifactorial and includes fluid-related hemodilution, blood loss, decreased red blood cell production, functional iron deficiency, and increased red blood cell destruction. With the use of restrictive transfusion policies, anemia remains present at the time of hospital discharge and can persist for up to six months after discharge [8–10]. It is difficult to determine if the presence of anemia is an independent predictor of poor outcomes or a marker of more severe underlying disease. Anemia, along with associated fatigue, shortness of breath, and cardiac complications, are associated with reduced quality of life after hospitalization [11,12]. The stress of compensatory cardiopulmonary responses to anemia has suggested a causal relation [11,12].
Changes in inflammatory anemia-associated parameters have been associated with 28-day mortality in patients with sepsis [13]. In sepsis survivors, there was chronic anemia along with significant differences in inflammatory markers [14]. These changes correlate with functional outcomes between rapid recovery and chronic critical illness patients [14]. The consequences of anemia in sepsis-related critical illness have not been fully explored. It is unknown if the degree of anemia at onset of sepsis could be used as a prognostic indicator for clinical course, inflammatory markers, and long-term functional outcomes. Utilizing the resources of the Sepsis and Critical Illness Research Center designed to evaluate long-term outcomes after sepsis, we hypothesized that patients who were severely anemic at sepsis onset would have higher inflammatory markers and higher levels of plasma erythropoietin (EPO) that would continue over time and lead to worse long-term functional outcomes.
Patients and Methods
Study site and patients
This was a retrospective case control study of surgical intensive care unit (ICU) patients who developed sepsis. This study was approved by the Institutional Review Board and was performed between January 2015 and June 2019 at an academic quaternary-care referral center. The study was registered with clinicaltrials.gov (NCT02276417) and conducted by the Sepsis and Critical Illness Research Center, whose study design and protocols have been published previously [15]. Two hundred twenty-four patients were who met criteria for the study were enrolled.
As published previously, screening for sepsis was carried out using the Modified Early Warning Signs-Sepsis Recognition System (MEWS-SRS), which quantifies derangements in vital signs, white blood cell count, and mental status [16,17]. All patients eligible for inclusion in the study were enrolled within 12 hours of sepsis protocol onset. If written informed consent could not be obtained from the patient or their legally assigned representative within 96 hours of study enrollment, the patient was removed from the study. All patients with sepsis were managed using a standardized, evidence-based protocol that emphasizes early goal-directed fluid resuscitation as well as other time-appropriate interventions such as administration of broad-spectrum antibiotics [18].
Patients eligible for participation in the study met the following inclusion criteria: admission to the surgical or trauma ICU; age ≥18 years; clinical diagnosis of sepsis, severe sepsis, or septic shock with this being the patient's first septic episode; and entrance into our sepsis clinical management protocol. Patients were excluded if any of the following were present: refractory shock (i.e., patients expected to die within the first 24 hours); an inability to achieve source control (i.e., irreversible disease states such as unresectable dead bowel); pre-sepsis expected lifespan less than three months; patient/family not committed to aggressive management; severe congestive heart failure (New York Heart Association [NYHA] class IV); Child-Pugh Class C liver disease or pre-liver transplant; known human immunodeficiency virus (HIV) with CD4+ count <200 cells/mm3; organ transplant recipient or use of long-term corticosteroids or immunosuppressive agents; pregnancy; institutionalized patients; chemotherapy or radiotherapy within 30 days; severe traumatic brain injury (i.e., evidence of neurological injury on CT scan and a Glasgow Come Scale <8); spinal cord injury resulting in permanent sensory and/or motor deficits; or inability to obtain informed consent.
Patient classification
Patients were diagnosed with sepsis, severe sepsis, or septic shock using the definitions established by the Society of Critical Care Medicine, the European Society of Intensive Care Medicine, the American College of Chest Physicians, the American Thoracic Society, and the Surgical Infection Society (SCCM/ESICM/ACCP/ATS/SIS) 2001 International Sepsis Definitions Conference [19]. The 224 patients were then subdivided into three different cohorts based on their hemoglobin (Hgb) at the 12-hour time point from sepsis onset. Patients with Hgb ≤8 g/dL were defined as the severe anemia group. Patients with Hgb between 8.1–10 g/dL were defined as the moderate anemia group. Patients with Hgb >10 g/dL were defined as the mild anemia group.
Clinical outcomes
We studied the Hgb trends for these three groups over time. Plasma granulocyte colony stimulating factor (G-CSF), interferon (IFN)-γ, and EPO were evaluated. Packed red blood cells (pRBC) transfused over the first 48 hours after sepsis onset were measured in milliliter. In terms of functional outcomes, the Zubrod score was determined. The Zubrod score ranges from zero to five, with increasing score reflecting worse performance status: zero, asymptomatic (fully active); one, symptomatic but completely ambulatory (restricted in physically strenuous activity); two, symptomatic, <50% in bed during the day (ambulatory and capable of all self-care but unable to perform any work activities); three, symptomatic, >50% in bed, but not bedbound (capable of only limited self-care); four, bedbound (completely disabled, incapable of any self-care); and five, death. Baseline or pre-hospitalization performance status was determined as soon as possible after study enrollment based upon patient or proxy reported four-week recall assessment. Functional outcomes were subsequently measured at three months, six months, and 12 months.
Sample collection and laboratory analysis
Serial blood samples were collected from hospitalized septic patients at 12 hours and on days one, four, seven, 21, 28, 35, and 42. Complete blood counts were performed by a hematology analyzer. Blood samples were then spun down for plasma by centrifuging the blood in a lavender top (ethylenediamimetetraacetic acide [EDTA]) blood collection tube at room temperature (22°C) for 10 minutes at 1,800g, with the brake on low. Plasma G-CSF, IFN-γ, TNF-α, and C-reactive protein (CRP) were measured using multiplex. Luminex® Multiplex Assays (Thermo-Fisher Scientific, Waltham, MA) utilize specialized magnetic microsphere beads coated with analyte specific antibodies. Multiple analyte specific beads of choice are combined with a test sample allowing for the detection and quantification of multiple targets in a single sample. Once the sample and beads have been combined, biotinylated detection antibodies and a streptavidin-phycoerythrin conjugate are added creating a capture sandwich immunoassay on each individual bead. These complexes are then analyzed with the Luminex® MAGPIX® (Luminex, Austin, TX) instrument using Luminex's xMAP® technology. The results are exported to the VigeneTech's MILLIPLEX™ Analyst software (VigeneTech, Carlisle, MA) and a complete detailed report of the data is produced. Plasma EPO (R&D, Minneapolis, MN) was measured by sandwich enzyme linked immunosorbent assay. All samples were run in duplicates according to manufacturer instructions.
Statistical analysis
Statistical analysis was performed in GraphPad Prism version 7.05 (GraphPad Software, La Jolla, CA). Figures are illustrated as line graphs over several time points and bar graphs. Variables were compared by two-way analysis of variance using Tukey's multiple comparisons test and reported as mean and standard deviation. Significance was set at p = 0.05 between group.
Results
Patient characteristics
Two hundred fifteen patients with sepsis were included with a mean age of 59 (range, 18–89). Males accounted for 58% of subjects. Nine patients were excluded from study based on exclusion criteria. Seventy-three patients had severe anemia (Hgb, 7.2 ± 0.7 g/dL); 75 patients had moderate anemia (Hgb, 9.1 ± 0.6 g/dL); and 67 patients had mild anemia (Hgb, 11.3 ± 1.1 g/dL) within 12 hours of sepsis onset. Hemoglobin at sepsis onset was not associated with a difference in Hgb on day 28. The severe anemia group had a mean age of 58 ± 16 years and 61% were male. The moderate anemia group had a mean age of 62 ± 13 years and 54% were male. The mild anemia group had a mean age of 56 ± 17 years and 58% were male. These age and gender differences were not statistically significant between groups.
Inflammatory cytokine patterns
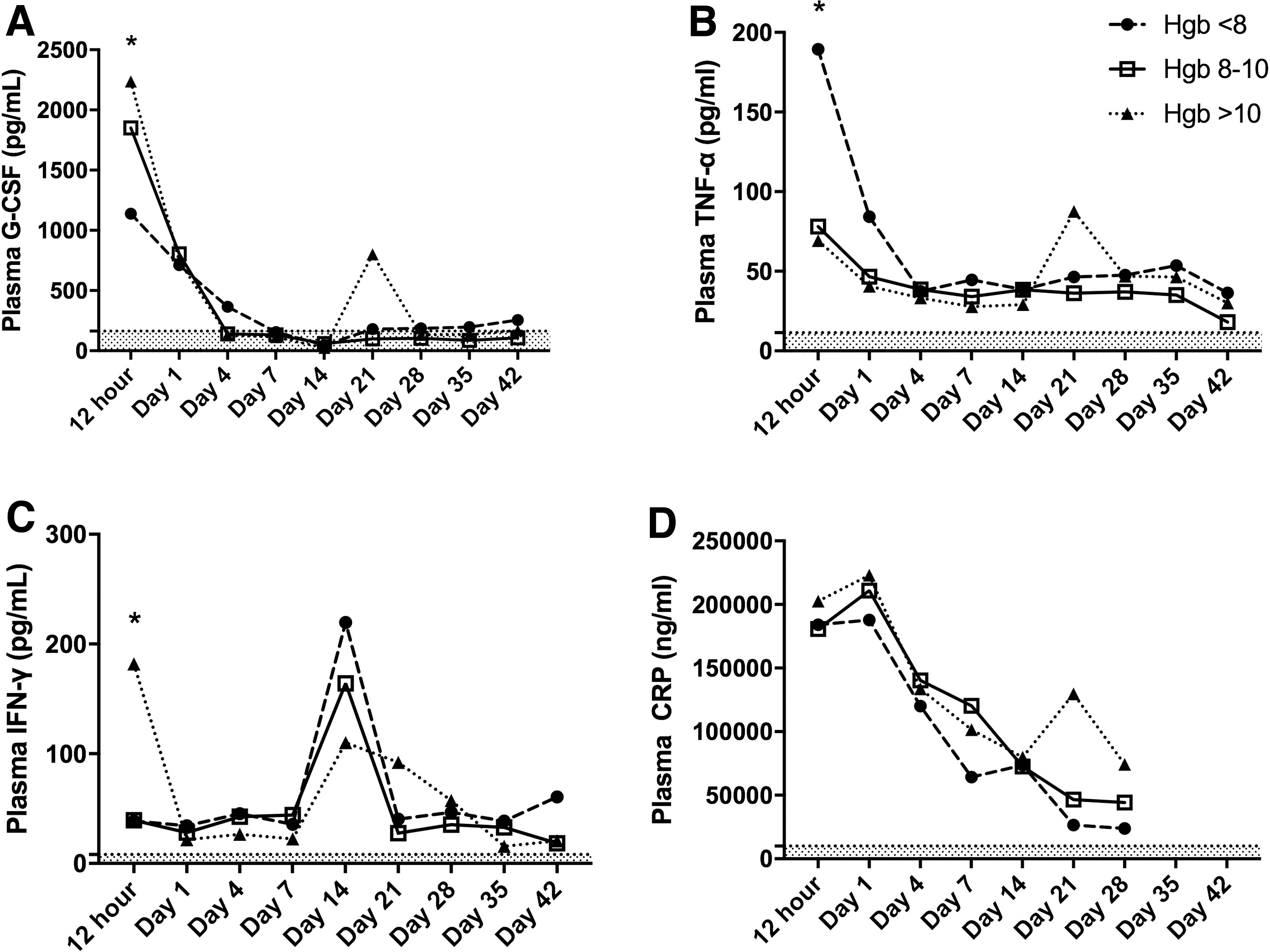
Plasma G-CSF concentrations were lowest in the severe anemia group at 12 hours from sepsis onset, and this was significant compared with plasma G-CSF concentrations in the mild anemia group (*p = 0.0023; Fig. 1A). Plasma G-CSF trended downward in all three groups and reached normal levels by day seven. The mild anemia group experienced a spike in plasma G-CSF on day 21 but this was not a statistically significant increase. By day 42, all three groups had a relatively normal plasma G-CSF concentration with no significant difference in trend among groups.
Inflammatory cytokine patterns. (
Plasma TNF-α levels were highest in the severe anemia group at 12 hours from sepsis onset, and this was significant compared with both the moderate and mild anemia groups (*p = 0.0271 and *p = 0.0245, respectively; Fig. 1B). Plasma TNF-α concentrations subsequently decreased and there were no substantial differences between groups at any later time points. The severe anemia group did have higher levels of circulating plasma TNF-α than the other two groups at days 35 and 42, although this was not statistically significant. All groups had concentrations of plasma TNF-α that remained persistently higher than normal at day 42 (two- to three-fold higher).
Plasma IFN-γ concentrations were highest in the mild anemia group at 12 hours from sepsis onset, and this was significant compared with both the moderate anemia and severe anemia groups (*p = 0.0154 and *p = 0.0181, respectively; Fig. 1C). Plasma IFN-γ concentrations decreased in the mild anemia group, down to levels similar to the moderate and severe anemia groups until day seven. All three groups experienced a spike in plasma IFN-γ concentration on day 14, although there was no statistically significant difference among groups, and all three groups trended back down on day 21. At day 42, the severe anemia group had the highest plasma IFN-γ concentration, at almost triple the concentrations seen in the mild and moderate anemia groups. However, this was not statistically significant (mean of 60 pg/mL vs. 18 and 20 pg/mL, respectively).
Plasma CRP concentration was substantially elevated from normal values in all three groups at 12 hours and day one (Fig. 1D). There was no substantial difference between the three anemia groups over time. All groups had persistently elevated concentrations of CRP compared with normal at day 42.
Plasma EPO response and anemia over time
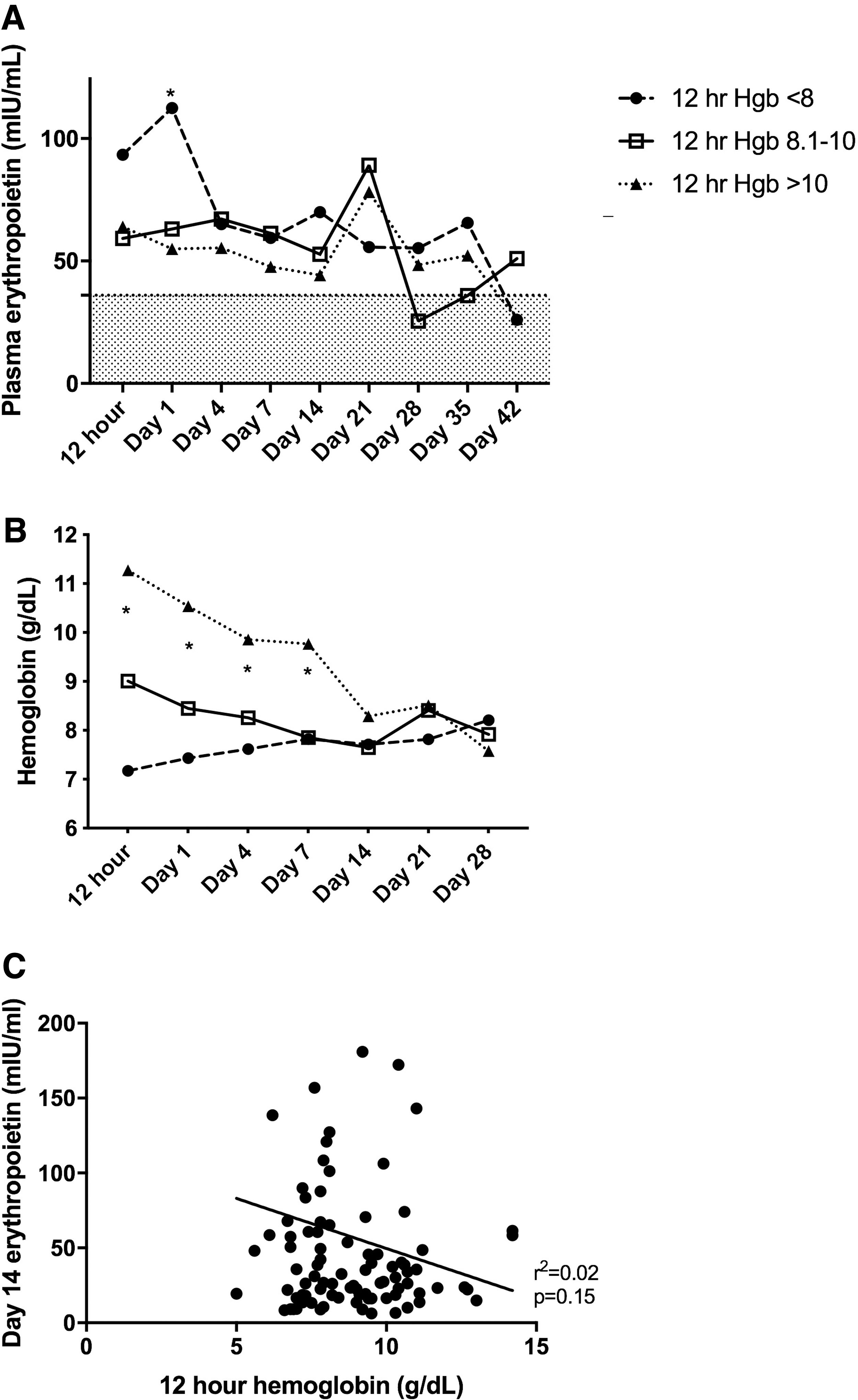
Plasma EPO concentration was highest in the severe anemia group at 12 hours from sepsis onset and peaked at day one (Fig. 2A). This was substantially higher than both the moderate and mild anemia groups (*p = 0.0212 and *p = 0.0142, respectively). All three groups then experienced a downtrend in plasma EPO levels until day 21, at which time plasma EPO levels peaked in the mild and moderate anemia groups. There was no statistically significant difference between groups at day 21. The plasma EPO levels decreased in all groups until day 42, at which point the mild and severe anemia groups had both returned to normal levels.
Ineffective erythropoietin (EPO) response to anemia and lack of anemia recovery. (
All patients with sepsis developed anemia by day one (Fig. 2B). The severe anemia group had a substantially lower Hgb at 12 hours from sepsis onset compared with both mild and moderate anemia groups through day four (*p < 0.005 between groups; Fig. 2B). By day seven, the severe anemia group and moderate anemia group had similar Hgb levels, but the mild anemia group still had substantially higher Hgb than both other groups (*p < 0.0001). By day 14, the mild anemia group's Hgb had decreased to the point that there was no difference between the three Hgb groups through day 28. On day 28, all three groups had a mean Hgb near 8 g/dL. Although there was a weakly negative correlation between day 14 EPO concentrations and 12-hour Hgb levels, this was not statistically significant (r = −0.1505; p = 0.1569; Fig. 2C).
Transfusions
The severe anemia group received significantly more pRBC transfusions in the first 48 hours after sepsis onset, with a mean of 541 ± 801 mL, compared with the moderate and mild anemia groups (mean 137 ± 477 mL and 7 ± 72 mL, respectively; *p < 0.0001; Fig. 3). Despite the use of transfusions, all three groups had a substantial anemia with a mean Hgb near 8 g/dL by day 28.

Difference in transfusions received between groups over 48 hours after sepsis onset. The severe anemia group received substantially more transfusions of packed red blood cells (pRBC) than the moderate or mild anemia groups. *p < 0.05 between groups. Hgb = hemoglobin.
Functional outcomes
At baseline of sepsis onset, there were no substantial differences between groups in terms of Zubrod score (Fig. 4). However, at three, six, and 12 months, the severe anemia group had substantially higher Zubrod scores compared with the mild anemia group (p < 0.03 for all three timepoints). At both six and 12 months, the Zubrod score was a point higher for those patients with severe anemia.

Functional outcomes are substantially worse with severe anemia at sepsis onset. Although there are no differences between groups at sepsis onset, the severe anemia group developed worse Zubrod scores at three, six, and 12 months. *p < 0.05 between groups. Hgb = hemoglobin.
Discussion
This study investigated the impact of the degree of anemia at the time of sepsis onset on the inflammatory cytokine patterns, the EPO response, and functional outcomes. Overall, our data show that the degree of anemia at the onset of sepsis did not correlate directly with inflammatory cytokine patterns or the degree of EPO response. There was, however, a strong association between the degree of anemia at sepsis onset and functional outcome scores at three, six, and 12 months. That is to say, the worse the anemia at sepsis onset, the worse the functional outcome scores over time.
In all groups, patients with sepsis developed anemia quickly. This was evidenced by the decreased Hgb that occurred in tandem with elevations of G-CSF, TNF-α, IFN-γ, and CRP. Inflammation-associated abnormalities in erythropoiesis contribute to early onset anemia, which has previously been demonstrated in patients with septic shock [13]. Persistent systemic inflammation has been linked to acute anemia in humans after severe blunt trauma as well as persistent anemia in translatable rodent models of trauma, hemorrhagic shock, and chronic stress [20–24]. High plasma levels of G-CSF are associated with anemia in humans and rodents, as well as egress of hematopoietic progenitor cells from the bone marrow [25, 26]. Cai et al. [27] demonstrated that although low-dose G-CSF treatment can improve fat graft survival in mice, high-dose G-CSF is associated with prolonged inflammation and can cause severe fibrosis. In this study, plasma G-CSF levels declined faster in the mild and moderate anemia groups than in the severe anemia group and highest in the severe anemia group at days 28–42. High plasma G-CSF levels at 24 hours from sepsis onset have been linked to worsening organ dysfunction [28]. All three groups had similar levels of plasma G-CSF 24 hours after onset of sepsis which did not correlate with anemia resolution.
Interferon-γ is a well-known proinflammatory cytokine that plays an important role in inflammation and has been reported to suppress hematopoietic stem cell self-renewal and multilineage differentiation, thus impairing normal hematopoiesis [29,30]. Tumor necrosis factor-α has been shown to suppress EPO and erythropoiesis both in vivo and in vitro [31,32]. C-reactive protein is a well-known marker of inflammation and has been shown as a predictor of EPO resistance in hemodialysis patients with chronic anemia [33]. In our critically ill patient population with sepsis, both plasma TNF-α and IFN-γ levels remained high in all three groups of patients (two- to six-fold higher than normal levels) until day 42 and were highest in the severe anemia group. This suggests that persistently high IFN-γ and TNF-α levels may suppress normal hematopoiesis long term and also contribute to the lack of EPO activity to improve anemia across all groups, but mostly in the severe anemia group. Our elevated CRP concentrations throughout the study correlate with persistent systemic inflammation and the presence of anemia in all three groups.
The kidneys produce EPO, which is the main regulator of erythropoiesis. Erythropoietin levels are known to increase significantly after burns and trauma [34–37]. Prior research has shown that although EPO levels were high after trauma, this was coupled with decreased expression of the bone marrow EPO receptor and an increase in plasma hepcidin concentration that was associated with a functional iron deficiency [20]. This dysfunctional EPO response was associated with a decrease in erythropoiesis and increased prevalence of injury-associated anemia after critical illness [20,23]. In this study, EPO levels were highest in the severe anemia group at sepsis onset and on day one. However, despite the elevation of EPO, this did not correlate with a substantial improvement in Hgb. Additionally, the degree of anemia at sepsis onset did not appear to help predict Hgb trend over time, all groups remained anemic.
Despite the presence of anemia in all three groups, there was not a prolonged EPO response to anemia over time. The persistently high levels of IFN-γ, TNF-α, and CRP may be contributing to this blunted and ineffective EPO response to severe anemia. Jiang et al. [13] also found a weak correlation between the presence of anemia and EPO levels in sepsis survivors and the authors speculated that the degree of inflammation overwhelmed the EPO response to improve Hgb levels [13]. Although the absence of a spleen was not documented in the patients included in this study, our group demonstrated previously that despite evidence of extramedullary hematopoiesis and elevated expression of splenic EPO after trauma, there was no improvement in Hgb levels [38].
Our study demonstrated that the degree of anemia at sepsis onset was predictive of long-term functional outcomes. Patients with severe anemia at sepsis onset were more likely to have severe long-term disability than those who have moderate or mild anemia at sepsis onset. Iwashyna et al. [39] found that sepsis survivors with no pre-hospitalization physical limitations reported a substantially higher number of new physical limitations after hospitalization compared with those who were hospitalized for non-sepsis reasons. Similarly, Gardner et al. [40] showed that patients with sepsis who develop chronic critical illness, as opposed those who recover rapidly, experience much worse long-term functional outcomes that may affect their ability to live independently.
In our study, there were no differences in pre-hospitalization Zubrod scores between groups, but there were substantial differences between groups at three, six, and 12 months, with the severe anemia group having substantially worse functional status at all subsequent time points, compared with the moderate and mild anemia groups. At both six and 12 months, the Zubrod score was a point higher for those patients with severe anemia. This finding has important clinical meaning. Those patients with mild anemia are now ambulatory and capable of all self-care but unable to perform any work activities compared with those patients with severe anemia who spend more than 50% of time in bed and capable of only limited self-care. This study enabled us to predict which population of patients with sepsis may be high risk for long-term disability and target these patients with earlier and more aggressive physical therapy, occupational therapy, and mobilization in the hospital to help mitigate these poor functional outcomes.
One limitation of this study is that it was a retrospective cohort study, undoubtedly a prospective study would lead to less selection bias. Another limitation of this study was that there were substantial differences in the number of transfusions received by the patients between groups, which may impact cytokine profiles and anemia recovery. In addition, the number of blood draws per patient as well as the timing of nutritional support was not collected, this may influence the degree of anemia as well as the number of cofactors available for red blood cell production. This study was also limited because the data was from a single institution. Because results from a single institution may not be generalizable, external validation is warranted.
Conclusions
Our study demonstrated that the degree of anemia at sepsis onset did not predict inflammatory trajectories or anemia recovery. However, our study did show that degree of anemia at sepsis onset was associated with worse long-term functional outcomes. It is known that patients who are chronically critically ill have worse functional outcomes than those who recover rapidly after sepsis, but the determination between chronic critical illness and rapid recovery is made later in their clinical course. This study helps us identify severely anemic patients at sepsis onset who would benefit from more aggressive mobilization to attempt to mitigate these dismal functional outcomes, thereby improving sepsis survivors' quality of life post-hospitalization.
Footnotes
Funding Information
The authors were supported in part by grants R01 GM105893-01A1 (A.M.M.), R01 GM113945-01 (P.A.E.), and P50 GM111152–01 (P.A.E. and A.M.M.) awarded by the National Institute of General Medical Sciences (NIGMS). L.S.K. and E.S.M. were supported by a post-graduate training grant (T32 GM-008721) in burns, trauma, and peri-operative injury by NIGMS.
Author Disclosure Statement
No competing financial interests exist.