
Abstract
Background:
Living in deprived areas is associated with poorer outcomes after certain vascular procedures and surgical site infection in other specialties. Our primary objective was to determine whether living in more income-deprived areas was associated with groin wound surgical site infection after arterial intervention. Secondary objectives were to determine whether living in more income-deprived areas was associated with mortality and clinical consequences of surgical site infection.
Methods:
Postal code data for patients from the United Kingdom who were included in the Groin Wound Infection after Vascular Exposure (GIVE) multicenter cohort study was used to determine income deprivation, based on index of multiple deprivation (IMD) data. Patients were divided into three IMD groups for descriptive analysis. Income deprivation score was integrated into the final multivariable model for predicting surgical site infection.
Results:
Only patients from England had sufficient postal code data, analysis included 772 groin incisions (624 patients from 22 centers). Surgical site infection occurred in 9.7% incisions (10.3% of patients). Surgical site infection was equivalent between income deprivation tertiles (tertile 1 = 9.5%; tertile 2 = 10.3%; tertile 3 = 8.6%; p = 0.828) as were the clinical consequences of surgical site infection and mortality. Income deprivation was not associated with surgical site infection in multivariable regression analysis (odds ratio [OR], 0.574; 95% confidence interval [CI], 0.038–8.747; p = 0.689). Median age at time of procedure was lower for patients living in more income-deprived areas (tertile 1 = 68 years; tertile 2 = 72 years; tertile 3 = 74 years; p < 0.001).
Conclusions:
We found no association between living in an income-deprived area and groin wound surgical site infection, clinical consequences of surgical site infection and mortality after arterial intervention. Patients living in more income-deprived areas presented for operative intervention at a younger age, with similar rates of comorbidities to patients living in less income-deprived areas.
Groin wound surgical site infection (SSI) after arterial surgery is common [1], and research into reducing SSIs in vascular surgery is recognized as a priority by both clinicians and patient/caregiver representatives [2]. Despite the substantial potential morbidity and mortality of these SSIs [3,4], the available evidence relating to contributory factors is largely historic or reliant on retrospective data [5–7]. Further research on the epidemiology of SSI in this patient group is needed to allow better risk stratification, improve pre-operative discussions of risk with patients, and to guide targeted SSI prevention strategies that often include expensive prophylactic interventions [8]. However, little is currently known about the impact of socioeconomic characteristics on groin wound SSIs in this population.
Socioeconomic deprivation is linked to health [9], and lifestyle-influenced cardiovascular diseases are more prevalent in more deprived areas [10]. Higher rates of unhealthy lifestyles (smoking, poor diet, and lack of physical exercise) in deprived areas are postulated to cause higher rates of cardiovascular risk increasing comorbidities, such as obesity and hyperlipidemia [10–12]. Several cardiovascular risk factors (e.g., smoking, body mass index, and diabetes mellitus), and peripheral arterial disease itself, are well recognized risk factors for SSI [13–16]. The association between socioeconomic deprivation and SSIs has previously been demonstrated in orthopedic surgery, cardiac surgery, and general surgery [17–19]. It is currently unknown whether living in an income-deprived area is associated with groin wound SSIs after arterial intervention.
It was recently demonstrated in a large registry study in the United Kingdom, that outcomes following endovascular intervention for occlusive peripheral arterial disease were worse for patients living in deprived areas [20]. To the best of our knowledge, this aspect of outcomes after arterial intervention through a groin incision has not been investigated. Furthermore, studies demonstrating higher prevalence of cardiovascular disease risk factors in more deprived areas are now mostly historic and have not specifically investigated those presenting for arterial intervention through a groin incision for demographic differences in relation to deprivation [9–12]. Updated, prospective evidence is required to determine whether health inequalities persist for such patients today.
Our primary objective was to determine whether residing in a more income-deprived area was associated with a higher risk of groin wound SSI after arterial intervention, by analyzing a subset of patients enrolled in the Groin wound Infection after Vascular Exposure (GIVE) multicenter cohort study [1,21]. Secondary objectives were to determine whether living in more income-deprived areas was associated with 30-day mortality and the clinical sequelae of SSI, and whether patients living in more income-deprived areas differed in terms of demographics and comorbidities compared with patients from less income-deprived areas.
Patients and Methods
This study is reported in accordance with The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for observational studies [22].
Summary of the GIVE study
The GIVE study was an international multicenter prospective observational cohort study of patients undergoing a groin incision for arterial intervention. The study protocol and results have been published [1,21], therefore, an abridged summary of the methodology is presented here.
Adult patients undergoing arterial exposure through a groin incision for an arterial procedure (both elective and emergency procedures) were included. Patients with an active infective process in the target groin and those undergoing cardiac procedures were excluded. The primary outcome was groin wound SSI rate, defined according to the U.S. Centers for Disease Control and Prevention (CDC) criteria [23]. Rates of superficial, deep organ/space SSIs, and consequences of SSI (sepsis, re-intervention, critical care re-admission, length of hospital stay, re-admission, and 30-day mortality) were included as secondary outcomes. Follow-up duration was 90 days. A further objective, determined a priori, was to investigate the effect of deprivation on these outcomes.
Income deprivation
An Index of Multiple Deprivation (IMD) was used to quantify income deprivation [24]. Indices of multiple deprivation are calculated for small areas in the United Kingdom, therefore only patients in the United Kingdom from the GIVE cohort were considered for inclusion in this study. The IMD and deprivation domain scores are calculated differently for each country in the United Kingdom, meaning results from each country are not directly comparable. Therefore, analyses were planned for each country separately. The postal codes of United Kingdom patients included in the GIVE cohort were collected, however, on review of the data, only the sample of patients from England had sufficient data for analysis. The English Indices of Deprivation 2019 was used [24].
The IMD is a score based on seven domains of deprivation: income, employment, education, health, crime, barriers to housing and services, and living environment. Each domain is given a score ranging from zero to one, representing the proportion of people in an area who experience deprivation. Indices of deprivation, such as the IMD in the United Kingdom, often incorporate health. In the case of the English Indices of Deprivation 2019, health outcomes such as premature death and overall poor health heavily influence the health domain, thus influencing the overall index. Therefore, bias is potentially introduced in any study examining associations between the overall IMD and health outcomes. To overcome this, we focused on one component of the index in isolation: the income deprivation domain.
For the purposes of the IMD, England is divided into 32,844 small areas with an average population of 1,500 people. Each of these small areas is then ranked from the highest score to the lowest (rank 1 being the most deprived small area, rank 32,844 being the least deprived small area). For ease of analysis, small areas may be categorized based on their rank, and this is a standard approach in studies categorizing patients based on IMD [17,19,24]. Because of the sample size in this study, it was determined that the sample would be most appropriately categorized into three groups (tertiles): tertile 1 being patients from small areas among the most deprived one-third of England, tertile 3 being patients from small areas among the least deprived one-third of England.
For demographic, comorbidity, and operative description analysis, the sample was split into tertiles as described above. The income deprivation score (rather than rank) for each small area was included to demonstrate the spread in our sample and used for regression analyses, because the income ranks do not follow a linear scale. Patients with missing postal code data were excluded from analysis. Further subgroup analyses were considered following scrutiny of the data.
Outcomes
The primary outcome for this study was the rate of groin wound SSI, defined according to the CDC criteria [23]. Secondary outcomes were:
Rates of superficial and deep organ/space groin wound SSI. Rate of 30-day mortality. Rates of key demographic, comorbidity, and operative variables in each income deprivation tertile. Rate of groin wound SSI clinical consequences for each income domain tertile: ○ Additional dressings ○ Negative pressure dressings ○ Antimicrobial dressings ○ Oral and intravenous antibiotic agents ○ Radiologic or surgical re-intervention (to manage SSI) ○ Explantation of foreign material ○ Unplanned admission to hospital ○ Sepsis ○ Unplanned admission to (or admission lengthened unexpectedly in) critical care ○ SSI-related loss of limb ○ SSI-related death
Statistical methods
Continuous variables were examined for normality using the Kolmogorov-Smirnov test, and the one-way analysis of variance (ANOVA) or Kruskal-Wallis tests used as appropriate. The χ2 test was used for categorical variables. Percentages were calculated using the number of patients as a denominator for patient-specific variables and outcomes. The number of groin incisions was used as a denominator for operative and post-operative variables and outcomes.
Missing data were handled by multiple imputation (Markov chain Monte Carlo method, 25 iterations, 25 imputation sets). Univariable and multivariable analysis were conducted to predict SSI and mortality (binary logistic regression). Univariable analysis was conducted for variables of interest and carried forward to backward stepwise multivariable analysis if they met the threshold of p < 0.1. Statistical significance for multivariable analysis was defined as p < 0.05. Income score was treated as a continuous variable for regression analyses, and if found to be non-significant on univariable analysis, was planned to be forced into the final model as a sensitivity analysis, as determined a priori.
Sensitivity regression analyses using complete-case analyses were conducted to assess the integrity of our multiple imputation method. Data were analyzed in SPSS Statistics, version 26 (IBM Corp, Armonk, NY).
Results
Sample demographics
There were 1,176 groin incisions in 938 patients from 30 centers in the United Kingdom. The numbers of patients with postal code data from Scotland and Wales were unacceptably low (no patients from Northern Ireland were included in the GIVE study), therefore, analyses were limited to patients in England only.
There were 907 groin incisions in 725 patients from 22 centers in England. No postal code data were available for 101 patients, meaning 772 groin incisions in 624 patients were included in final analysis. Full demographic details of the sample are shown in Table 1. The number of male patients was 465 of 624 (74.5%), median age at surgery was 71 years (interquartile range [IQR], 64–78), median (IQR) body mass index (BMI) was 26.3 (23.0–30.5). Most were Caucasian (582/605; 96.2%); 191 of 623 (30.7%) had type 1 or type 2 diabetes mellitus; 194 of 611 (31.8%) had ischemic heart disease (IHD); 25 of 556 (4.5%) had a pre-operative estimated glomerular filtration rate (eGFR) <30 mL/min/1.73 m2; and 136 of 620 (21.9%) had chronic obstructive pulmonary disease (COPD). Patients with severe (or worse) pre-operative morbidity, i.e., American Society of Anesthesiologists (ASA) 3–5 accounted for 507 of 583 (87%); 266 of 620 (42.9%) patients underwent an emergency or urgent procedure. The income scores assigned to each patient did not follow a normal distribution, the median income score (IQR) for the sample was 0.110 (0.061–0.197), compared with a median income score (IQR) of 0.099 (0.056–0.178) for all LSOAs in England in the English Indices of Deprivation 2019 [24]. This means our sample of patients lived in areas of higher income deprivation compared with the whole of England.
Demographics of Patients Undergoing Arterial Intervention through a Groin Incision in England
eGFR = estimated glomerular filtration rate; ASA = American Society of Anesthesiologists; IQR = interquartile range.
The number of patients in income domain tertile 1 (most income-deprived areas), tertile 2, and tertile 3 (least income-deprived areas), were 238 (38.1%), 205 (32.9%), and 181 (29.0%), respectively (Fig. 1).
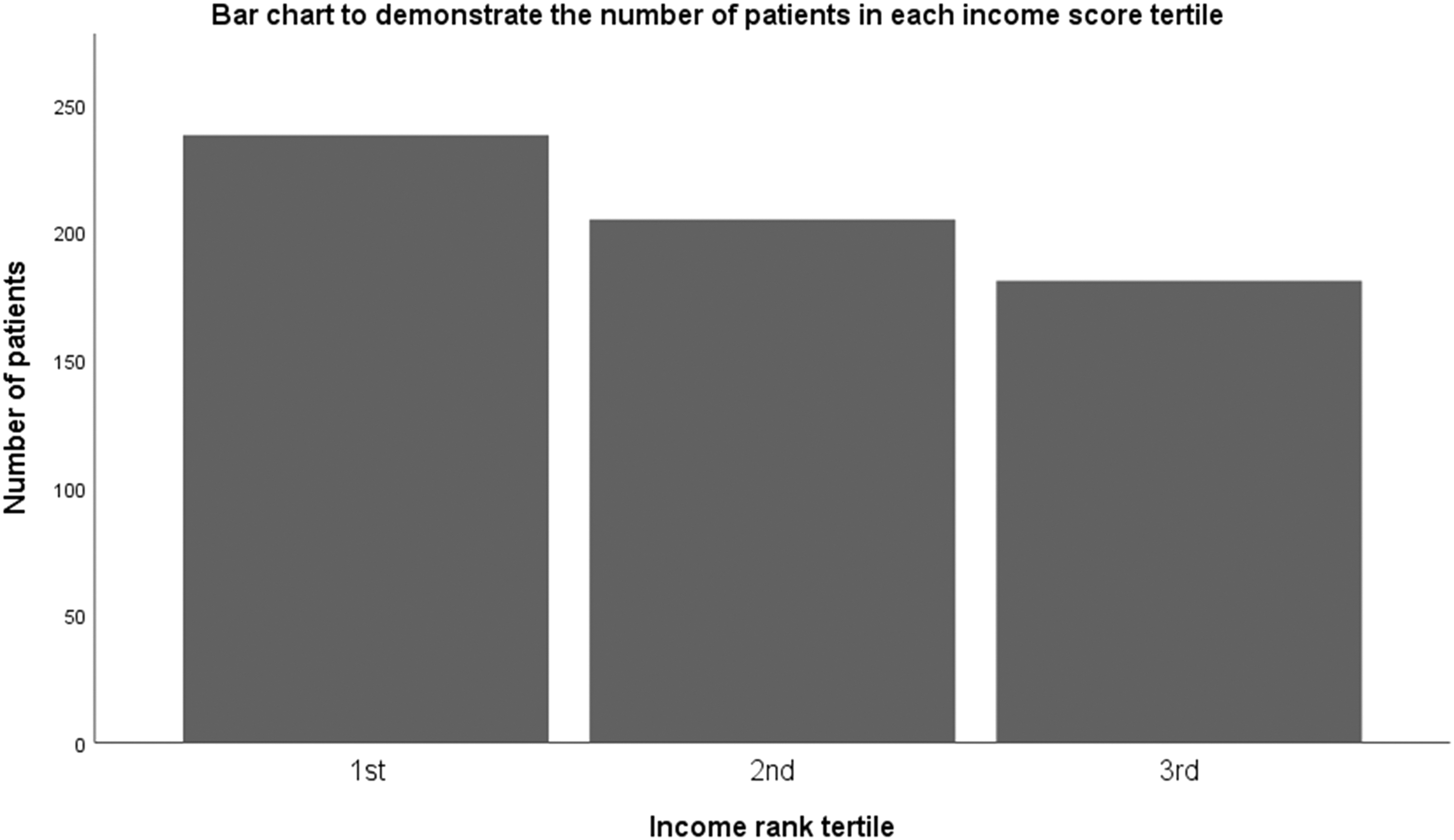
Number of patients living in each income deprivation tertile. Tertile 1: most income-deprived areas. Tertile 3: least income-deprived areas.
Characteristics across income domain tertile groups
Demographic, comorbidity, and operative data were similar between the tertiles (Table 2). Median age at time of procedure increased significantly with decreasing area income deprivation: tertile 1 median (IQR) age, 68 (59–75); tertile 2 median age, 72 (66–78); and tertile 3 median age, 74 (65–81), p < 0.001. Tertile 1 had a significantly higher prevalence of COPD compared with tertiles 2 and 3: tertile 1 = 64 of 237 (27%); tertile 2 = 36 of 204 (17.6%); tertile 3 = 36 of 179 (20.1%), p = 0.047. Tertile 1 had a significantly higher prevalence of hyperlipidemia compared with tertile 2: tertile 1 = 110 of 210 (52.4%); tertile 2 = 74 of 192 (38.5%); tertile 3 = 84 of 171 (49.1%), p = 0.016. Similarly, there were statistically significant differences without appreciable trend (in relation to income deprivation) between the tertiles in rates of groin incisions that were shaved pre-operatively with clippers, had aqueous chlorhexidine used as skin preparation, had a separate leg incision (in addition to a groin incision), and had skin glue applied as the only dressing. There was no significant difference in the median length of hospital stay in days between the tertiles: tertile 1 (IQR) = 5 (2.0–10.0); tertile 2 = 3 (3.0–11.0); tertile 3 = 4 (2.0–8.0), p = 0.064.
Demographic, Comorbidity, and Operative Data per Income Deprivation Tertile
eGFR = estimated glomerular filtration rate; SSI = surgical site infection; ASA = American Society of Anesthesiologists; IQR = interquartile range.
Statistical significance.
Surgical site infection rates
There were 75 of 772 (9.7%) groin wound SSIs in 64 of 624 (10.3%) patients. Of these groin wound SSIs, 29 of 75 (38.7%) were deep organ/space SSIs, and 46 of 75 (61.3%) were superficial SSIs. There were no significant differences between the income domain tertiles in terms of overall SSI, superficial SSI, and deep organ/space SSI rates (Table 3). Increasing income score was not significant in univariable regression analysis in predicting either SSI or 30-day mortality.
Rates of SSI, Superficial SSI, Deep Organ/Space SSI, and Thirty-Day Mortality per Income Deprivation Tertile
SSI = surgical site infection
Independent predictors of all SSIs in this sample were: increasing age (years) (OR, 1.031; 95% CI, 1.003–1.059; p = 0.030), female gender (OR, 1.845; 95% CI, 1.069–3.185; p = 0.028), BMI ≥30 kg/m2 compared with a normal BMI (OR, 3.267; 95% CI, 1.468–7.269; p = 0.004), COPD (OR, 1.952; 95% CI, 1.147– 3.323; p = 0.014), IHD (OR, 1.880; 95% CI, 1.140–3.100; p = 0.013), re-do groin incision (OR, 1.926; 95% CI, 1.047–3.543; p = 0.035), aqueous betadine skin preparation compared with alcoholic chlorhexidine (OR, 4.012; 95% CI, 2.014–7.992; p < 0.001), xenograft bypass/patch material compared with no bypass/patch used (OR, 5.493; 95% CI, 2.353–12.824; p < 0.001), prosthetic bypass/patch material compared with no bypass/patch used (OR, 2.788; 95% CI, 1.136–6.839; p = 0.025), and increasing operative time (hours) (OR, 1.646; 95% CI, 1.018–1.334; p = 0.027; Table 4). When forced into the final model, increasing income score was not predictive of SSI (p = 0.689).
Independent Predictors of All SSIs, Including Income Score When Forced into the Model
SSI = surgical site infection; BMI = body mass index.
Statistical significance.
Sensitivity analysis using complete-case analysis identified BMI ≥30Kg/m2, chronic obstructive pulmonary disease, ischaemic heart disease, American Society of Anesthesiologists grade 3-5 (compared to ASA grade 1-2), re-do groin incision, aqueous betadine skin preparation, xenograft bypass/patch material compared to no bypass/patch, and intraoperative transfusion as independent predictors of all SSIs (Supplementary Table S1). In contrast to our analysis using multiple imputed data, female gender, prosthetic bypass/patch material, and increasing operative time were not independent predictors of all SSIs on complete-case analysis.
Mortality
The 30-day mortality frequency was 11 of 238 (4.6%), 10 of 205 (4.9%), and 9 of 181 (5.0%) for tertiles 1, 2, and 3, respectively (p = 0.985). Independent predictors of 30-day mortality were: increasing age (years) (OR, 1.059; 95% CI, 1.025–1.094; p = 0.001), female gender (OR, 1.985; 95% CI, 1.028–3.836; p = 0.041), pre-operative eGFR <30 mL/min/1.73 m2 (OR, 3.443; 95% CI, 1.266–9.368; p = 0.015), and increasing operative time (hours) (OR, 1.170; 95% CI, 1.008–1.358; p = 0.038) (Supplementary Table S2). When forced into the final model, increasing income score was not predictive of 30-day mortality (p = 0.286). Independent predictors of 30-day mortality in complete-case analysis were increasing age, female gender, and increasing operative time (Supplementary Table S3).
Clinical consequences of SSI
Among the patients who developed a groin wound SSI, there were no statistically significant differences between the income domain tertiles in terms SSI management and clinical consequences: additional dressings, negative pressure therapy dressings, antimicrobial dressings, oral and intravenous antibiotic agents, radiologic or surgical re-intervention, explantation of foreign material, unplanned admission to hospital, sepsis, unplanned admission to (or admission lengthened unexpectedly in) critical care, SSI-related loss of limb and SSI-related death (Supplementary Table S4).
Urgent/emergency procedures
The number of patients undergoing an urgent or emergency procedure was 266 of 620 (42.9%), therefore further analysis comparing these procedures to elective procedures was undertaken. The full demographic and procedural variables that were compared between urgent/emergency and elective procedures are shown in Supplementary Table S5. In the urgent/emergency group, significantly more patients had: eGFR <30, partially dependent functional status, post-operative anticoagulant use, and an ASA grading of 3–5. Fewer patients in the urgent/emergency group had a Rutherford grading of 4–6, capacity to consent, hypertension, post-operative single antiplatelet use, and bilateral incisions. Urgent/emergency cases differed from elective procedures with regards to some operative variables: more limbs with open wounds, more re-do incisions, less use of non-iodinated adhesive skin preparation, more groin incisions extended to the leg, more open only procedures, fewer aneurysmal endovascular ± open procedures, less use of xenograft as bypass/patch material, more muscle flaps created, more wound drains used, and more use of local antibiotic agents. Median income score did not differ significantly between urgent/emergency and elective patients (p = 0.755).
The number of SSIs did not significantly differ between urgent/emergency procedures and elective ones (p = 0.145); there was a non-significant trend of increased mortality with urgent/emergency procedures: 15 of 266 (6.8%) versus 12 of 354 (3.4%); p = 0.052. Patients undergoing an urgent/emergency procedure had a shorter median operative time (3 [IQR, 2–4] hours vs. 3.2 [IQR, 2.5–4] hours; p = 0.007) and a longer hospital length of stay (7 [IQR, 3–15] days vs. 4 [IQR, 2–7] days; p < 0.001).
Supplementary Table S6 shows the results of multivariable logistic regression analyses to identify predictors of SSI in both subgroups (elective and urgent/emergency procedures). Income deprivation was not significant on univariate analysis for either subgroup. When forced into both models, income deprivation was not identified as an independent predictor of SSI: OR, 1.395; 95% CI, 0.022–89.096; p = 0.875 (urgent/emergency); OR, 0.074; 95% CI, 0.002–2.755; p = 0.158 (elective).
Discussion
The overall number of groin wound SSIs was 75 of 772 (9.7%) per groin incision, and 64 of 624 (10.3%) per patient. There were no significant differences between the income deprivation tertiles in terms of groin wound SSI rates, clinical consequences of SSI, and 30-day mortality rate. Income deprivation score was not associated with SSI and 30-day mortality, this was consistent in subgroup analysis. Median age at time of procedure differed significantly between the tertiles: increasing with decreasing area income deprivation.
The overall SSI rate in our study is comparable to that reported in existing literature on vascular groin wound SSIs [5–7]. In contrast to previously published research on SSIs and socioeconomic deprivation in other specialties [17–19], we found no association in our sample. This may be because of differences in the patient samples: previous studies include either orthopedic or cardiac patients who are likely to have different patient-related and procedure-related SSI risk profiles in comparison to our sample. Our findings support that those patients requiring vascular intervention have a relatively high prevalence of SSI risk factors regardless of socioeconomic status, since many are also cardiovascular disease risk factors [5,16,25], and groin wounds themselves increase the risk of SSI [5]. These results further the understanding of the epidemiology of groin wound SSI after vascular intervention. Ideally, surgeons could predict which patients are likely to develop SSI and selectively utilize often expensive SSI-preventing adjuncts. There is difficulty for clinicians in synthesizing complex information to produce accurate predictions of post-operative outcomes [26], and few validated groin wound SSI-specific prediction models are available [27].
There are several questions regarding vascular groin wound SSI risk factors and prevention that remain. The efficacy and cost-effectiveness of wound adjuncts aimed at preventing SSIs need to be further evaluated [8]. It is unknown why female gender is associated with increased groin wound SSI in the vascular population [1,4,5], although it is plausible that this is the result of the fat distribution pattern (favoring the gluteo-femoral area as opposed to visceral) [28]. Other potentially relevant variables that are yet to be researched in the context of vascular groin wound SSIs are intra-operative wound tension and lymphatic vessel preservation/control. This study provides up-to-date evidence suggesting that SSI-reducing strategies should target modifiable patient- and procedure-related risk factors and additional interventions/adjuncts aimed at preventing SSIs [1,8], regardless of income deprivation.
Socioeconomic deprivation is associated with poorer outcomes in other areas of vascular surgery; mortality outcomes after abdominal aneurysm repair [29], aortic dissection [30], and lower limb re-vascularization [20,31] have been reported to be higher in patients living in more deprived areas. We did not identify an association between living in a more income-deprived area and poorer outcomes in this study. Potential reasons include differences in the populations studied, the potential bias introduced in previous studies that use a composite measure of socioeconomic deprivation that is influenced by health outcomes [24], publication bias in the literature, and confounding from unknown variables that have not been accounted for in our analyses.
Our data suggest that patients living in more income-deprived areas were presenting with similar comorbidities and with similar pathology at a younger age than their counterparts living in less income-deprived areas. The inverse association between increasing small-area socioeconomic deprivation and age at initial presentation with cardiovascular disease has been demonstrated previously [10,32]. There are significant early and late morbidity and mortality risks associated with arterial surgery [33,34]. Requiring surgical intervention at a median of six years earlier in life (the difference between the most and least income-deprived tertiles in this sample) can potentially result in a significant number of life-years lost, and disability life-years suffered, considering the volume of procedures undertaken [35]. This result highlights that there are persistent cardiovascular health inequalities in England that are proving challenging to address. It is long established that unhealthy lifestyles and cardiovascular deaths are more prominent in deprived communities [10]. Primary prevention strategies, if implemented successfully, may address this issue [36]. More recently, however, there is evidence demonstrating poorer engagement with abdominal aortic aneurysm (AAA) screening services in more deprived areas [37,38]. Improving health service engagement in deprived communities is one way that healthcare providers may be able to address cardiovascular health inequalities [39]. Further research is required to determine whether this is true of other key aspects of vascular services (e.g., supervised exercise programs for intermittent claudication, and compliance with best medical therapy for cardiovascular disease prevention).
A strength of this prospective study is that we included consecutive patients from 22 centers from a variety of geographical areas in England. The 2019 English IMD closely aligned with our study period (January 21, 2019 through May 1, 2019). This means our results are highly specific and applicable to vascular practitioners in England, which would not be achievable with a more geographically heterogenous sample. The relation between socioeconomic status and health risk-factors varies between countries [41]. Similarly, different socioeconomic factors may be more relevant to risk factor exposure (e.g., rurality in very low-income countries will be more relevant than in a high-income country) [40]. These are complex sources of bias and confounding that were avoided in this relatively homogenous sample. The composite IMD score includes health outcome data (heavily influenced by premature death, and poor overall health) which introduces potential bias when examining health outcomes [24]; we avoided this by investigating the income deprivation domain of the IMD in isolation. Our sensitivity analysis (complete-case analysis) identified independent predictors of SSI and mortality that were largely similar to our analysis using multiple imputed data.
There are several limitations to this study. The entire GIVE study cohort was not analyzed, reducing the sample size and, therefore, reducing the power of this study to detect associations with deprivation. Despite having data on patients from 22 centers, applicability outside of England is limited. Similarly, the vast majority of patients were Caucasian, and results reported here may not be applicable to areas where the majority of patients are of different ethnicity. We did not have patient-specific income deprivation data, therefore, we cannot extrapolate our findings to make assumptions about how individual income deprivation influences SSI risk. There are unknown variables that may have introduced confounding such as intra-operative wound tension and lymphatic vessel control. Last, follow-up data capture in the GIVE study was limited to clinical notes, outpatient clinic records, and documentation from re-presentation to hospital. This means that milder superficial SSIs that were treated in the community unknown to the treating vascular team could have been missed, which is reflected in the relatively high proportion of SSIs that were deep organ/space in this sample.
Conclusions
There was no association between living in more income-deprived area and SSIs, mortality, and clinical consequences of SSI in this sample. Patients living in more income-deprived areas had equivalent comorbidities and vascular procedures compared with patients living in less income-deprived areas, but they presented for operative intervention at a younger age.
Funding Information
No funding was received.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
GIVE Study Group
Abdulmunem Althini, Alkhadra Hospital. Libya; Adnan Bajwa, Frimley Park Hospital. United Kingdom; Ahmed Elbasty, Frimley Park Hospital. United Kingdom; Ahmed Elhadi, Tripoli Medical Center. Libya; Ahmed Hassanin, Tallaght University Hospital. Ireland; Ahmed Msherghi, Tripoli Medical Center. Libya; Ahmed Shalan, Queen Elizabeth Hospital Birmingham. United Kingdom; Ala Khaled, Tripoli Medical Center. Libya; Aled Jones, Royal Cornwall Hospital. United Kingdom; Alexander Crichton, Russells Hall Hospital. United Kingdom; Aminder Singh, Addenbrooke's Hospital. United Kingdom; Amy Stimpson, Morriston Hospital. United Kingdom; Andrew Batchelder, Glenfield Hospital. United Kingdom; Andrew Cowan, Royal Devon and Exeter Hospital. United Kingdom; Andrew Duncan, Glenfield Hospital. United Kingdom; Ankur Thapar, St George's Hospital. United Kingdom; Annie Clothier, Royal Gwent Hospital. United Kingdom; Arsalan Wafi, St George's Hospital. United Kingdom; Asif Mahmood, University Hospital Coventry. United Kingdom; Athanasios Saratzis, Guy's and St Thomas' Hospitals. United Kingdom; Benjamin Patterson, St Mary's and Charing Cross Hospitals. United Kingdom; Bethany Wardle, Southmead Hospital. United Kingdom; Brenig L. Gwilym, Royal Gwent Hospital. United Kingdom; Bridget Egan, Tallaght University Hospital. Ireland; Calvin Eng, Royal Infirmary Edinburgh. United Kingdom; Ciaran Brennan, Royal Cornwall Hospital. United Kingdom; Claire Perrott, St Mary's and Charing Cross Hospitals. United Kingdom; Craig Forrest, Queen Elizabeth University Hospital. United Kingdom; Dafydd Locker, Royal Gwent Hospital. United Kingdom; Daniel U. Rodriguez, John Radcliffe Hospital. United Kingdom; Danielle Lowry, Royal Gwent Hospital. United Kingdom; David Bosanquet, Royal Gwent Hospital. United Kingdom; David Cooper, Cheltenham General Hospital. United Kingdom; David Milgrom, Wythenshawe Hospital. United Kingdom; Devender Mittapalli, Derriford Hospital. United Kingdom; Elaine Townsend, Royal Glamorgan Hospital. United Kingdom; Ella Schofield, John Radcliffe Hospital. United Kingdom; Emily Boyle, Tallaght University Hospital. United Kingdom; Emily Kirkham, Cheltenham General Hospital. United Kingdom; Enrico Mancuso, Addenbrooke's Hospital. United Kingdom; Faris Saleh, Wythenshawe Hospital. United Kingdom; Fernando Picazo, Royal Perth Hospital. Australia; Francesca Guest, Southmead Hospital. United Kingdom; Gareth Harrison, Countess of Chester Hospital. United Kingdom; George Dovell, Southmead Hospital. United Kingdom; George Smith, Hull Royal Infirmary. United Kingdom; Ghazaleh Mohammadi-Zaniani, Newcastle Freeman Hospital. United Kingdom; Graeme K. Ambler, Southmead Hospital. United Kingdom; Hannah Burton, Royal Devon and Exeter Hospital. United Kingdom; Hannah Danbury, John Radcliffe Hospital. United Kingdom; Hayley Moore, Frimley Park Hospital. United Kingdom; Hazem Ahmed, Alkhadra Hospital. Libya; Helen Suttenwood, Russells Hall Hospital. United Kingdom; Huw Davies, Birmingham Heartlands Hospital. United Kingdom; Iain Roy, Countess of Chester Hospital. United Kingdom; Ian Barry, Fiona Stanley Hospital. Australia; James Ackah, Derriford Hospital. United Kingdom; James Forsyth, Leeds General Infirmary. United Kingdom; James Olivier, Cheltenham General Hospital. United Kingdom; Jonathan Nicholls, Cheltenham General Hospital. United Kingdom; Joseph Shalhoub, St Mary's and Charing Cross Hospitals. United Kingdom; Kamil Naidoo, St Mary's and Charing Cross Hospitals. United Kingdom; Kamran Mohiuddin, Morriston Hospital. United Kingdom; Katherine Hurst, John Radcliffe Hospital. United Kingdom; Keith Hussey, Queen Elizabeth University Hospital. United Kingdom; Kerry Burke, Wythenshawe Hospital. United Kingdom; Khalid Bashar, Queen Elizabeth Hospital Birmingham. United Kingdom; Kishore Sieunarine, Royal Perth Hospital. Australia; Konstantinos Tigkiropoulos, Papageorgiou Hospital. Greece; Lewis Meecham, University Hospital Coventry. United Kingdom; Louise Hitchman, Hull York Medical School. United Kingdom; Lucy Green, Hull Royal Infirmary. United Kingdom; Luke Hopkins, Morriston Hospital. United Kingdom; Maciej Juszczak, Birmingham Heartlands Hospital. United Kingdom; Madhu Rangaraju, Birmingham Heartlands Hospital. United Kingdom; Matthew Brown, Glenfield Hospital. United Kingdom; Michael Rocker, Royal Glamorgan Hospital. United Kingdom; Michelle Cronin, Royal Glamorgan Hospital. United Kingdom; Mohamed Altabal, Al Masarra Clinic. Libya; Mohedin Arifi, Al Masarra Clinic. Libya; Muhammed Elhadi, Tripoli Medical Center. Libya; Natasha Chinai, Southmead Hospital. United Kingdom; Nicholas Platt, Cheltenham General Hospital. United Kingdom; Nikesh Dattani, Russells Hall Hospital. United Kingdom; Nishath Altaf, Royal Perth Hospital. Australia; Olivia Grant, Royal Glamorgan Hospital. United Kingdom; Olivia McBride, Royal Infirmary Edinburgh. United Kingdom; Owain Fisher, University Hospital Coventry. United Kingdom; Panagiota Birmpili, The Royal Liverpool University Hospital. United Kingdom; Paul Moxey, St George's Hospital. United Kingdom; Philip Stather, Addenbrooke's Hospital. United Kingdom; Rachael Forsythe, Royal Infirmary Edinburgh. United Kingdom; Rachel Falconer, Raigmore Hospital. United Kingdom; Rachel Sam, Queen Elizabeth Hospital Birmingham. United Kingdom; Robert Hinchliffe, Southmead Hospital. United Kingdom; Russell Jamieson, Royal Infirmary Edinburgh. United Kingdom; Ruth A. Benson, Russells Hall Hospital. United Kingdom; Ryan Preece, St Mary's and Charing Cross Hospitals. United Kingdom; Salil Korambayil, Royal Cornwall Hospital. United Kingdom; Samuel Debono, Queen Elizabeth University Hospital. United Kingdom; Sandhir Kandola, The Royal Liverpool University Hospital. United Kingdom; Sandip Nandhra, Newcastle Freeman Hospital. United Kingdom; Sarah Onida, St Mary's and Charing Cross Hospitals. United Kingdom; Sean Tierney, Tallaght University Hospital. Ireland; Shaneel Patel, The Royal Liverpool University Hospital. United Kingdom; Simon Neequaye, The Royal Liverpool University Hospital. United Kingdom; Tariq Al-Samarneh, Wythenshawe Hospital. United Kingdom; Tasleem Akhtar, Russells Hall Hospital. United Kingdom; Thomas Aherne, Tallaght University Hospital. Ireland; Thomas Wilson, Royal Cornwall Hospital. United Kingdom; Timothy Beckitt, Southmead Hospital. United Kingdom; Toby Richards, Fiona Stanley Hospital. Australia; Tom Hardy, Royal Devon and Exeter Hospital. United Kingdom; Tom Wallace, Leeds General Infirmary. United Kingdom; Tristan Lane, St Mary's and Charing Cross Hospitals. United Kingdom; Trixie Yap, Guy's and St Thomas' Hospitals. United Kingdom; Tryfon Vanias, Glenfield Hospital. United Kingdom; Ummul Contractor, Royal Glamorgan Hospital. United Kingdom.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.