
Abstract
Objective:
We describe a patient with history of heart transplant on maintenance immunosuppression who presented with sigmoid colon perforation from cytomegalovirus (CMV) colitis and performed a systematic review of outcomes after perforated CMV colitis.
Background:
Cytomegalovirus enterocolitis is uncommon among solid organ transplant patients and can result in small or large bowel perforation.
Methods:
We systematically reviewed articles describing patients with CMV enterocolitis with small or large bowel perforations from PubMed, Embase, and Web of Science from database inception to February 2021.
Results:
Seventy-seven articles were identified containing 84 patients with perforated CMV enterocolitis. The most prevalent comorbid diagnosis was human immunodeficiency virus (HIV; 27 patients, 32%), and 37 patients (44%) were taking corticosteroids at time of presentation. The ileum was the most common location for a perforation (26 patients, 31%). Odds of survival were lower for patients with small bowel perforation (odds ratio [OR], 0.38; 95% confidence interval [CI], 0.14–0.98) and HIV/acquired immunodeficiency syndrome (AIDS; OR, 0.32; 95% CI, 0.11–0.88). Odds of survival were higher for patients with large bowel perforation (OR, 2.64; 95% CI, 1.03–7.09), radiographically diagnosed perforation (OR, 3.45; 95% CI, 1.12–11.60) and those who received a CMV antiviral (OR, 9.19; 95% CI, 3.26–28.48).
Conclusions:
Perforated CMV enterocolitis is uncommon even in immunocompromised hosts. Clinicians should maintain a high level of suspicion for CMV-induced bowel perforation in this population because antiviral treatment is associated with increased odds of survival.
Cytomegalovirus (CMV) is a common pathogen that can threaten immunocompromised patients. Most (50%–80%) adults harbor antibodies to CMV [1], but the virus commonly reactivates in immunosuppressed patients, such as those who have undergone solid organ transplant. More than 90% of heart transplant patients may experience active CMV infection in the year after transplant [2]. Although only 3% of solid-organ transplant recipients develop active CMV infection later than one year after transplant, late CMV infection has a worse prognosis than early CMV infection [3]. It is estimated that of the 22%–52% of solid-organ transplant patients who are admitted with diarrhea [4], at least 6% of cases are because of CMV colitis [5]. Case reports document occasional bowel perforation in CMV enterocolitis [6–8], but estimates of incidence have not been reported.
We present a case of a sigmoid colon perforation caused by CMV colitis in a heart transplant patient and performed a systematic review of perforated CMV enterocolitis. Clinicians should have a high index of suspicion for CMV enterocolitis in transplant patients on immunosuppression, including those with a distant history of transplant.
Case Presentation
A 76-year-old female with history of heart transplant 17 years prior presented to an outside emergency department after a ground level fall with hypotension, altered mental status, and abdominal pain. She was transferred to our institution after receiving fluid resuscitation and intravenous antibiotic agents (ceftriaxone, 2 g; azithromycin, 500 mg; metronidazole, 500 mg; and piperacillin-tazobactam, 3.375 g). On arrival vital signs were remarkable for hypotension (105/67 mm Hg) and an oxygen requirement (95% saturation on two liters of oxygen, respiratory rate 20 breaths per minute), but was afebrile (35.9°C) and non-tachycardic (88 bpm). Laboratory tests were notable for creatinine 4.91 mg/dL, white blood cell count of 12.0 K/mcL (80.4% neutrophils, 8.4% lymphocytes), and lactate 0.44 mmol/L. The patient's immunosuppression included tacrolimus 2 mg every morning and 2.5 mg each night at bedtime by mouth and mycophenolate mofetil 500 mg twice daily orally. Surgical history included ventral hernia repair with mesh.
Computed tomography (CT) of the abdomen and pelvis revealed pneumoperitoneum and the patient was taken to the operating room for a presumed upper gastrointestinal perforation. Initial diagnostic laparoscopy revealed what was suspected to be a partially healed duodenal ulcer over which a Graham patch was placed. However, in the ensuing days the patient continued to display sepsis suggesting another source of intra-abdominal infection. Two repeat CTs with oral contrast did not reveal the extraluminal leak, although minimal contrast was seen in the distal portions of her gastrointestinal tract (Fig, 1).

(
Because the patient continued to deteriorate with evidence of peritonitis, emergent exploratory laparotomy was performed on hospital day five, with fecal diversion to control a presumed distal perforation not identified on the initial operation. After additional resuscitation, the patient was again taken to the operating room for washout and possible closure during which a 1 cm perforation was found in her sigmoid colon. Sigmoidectomy was performed with creation of end colostomy.
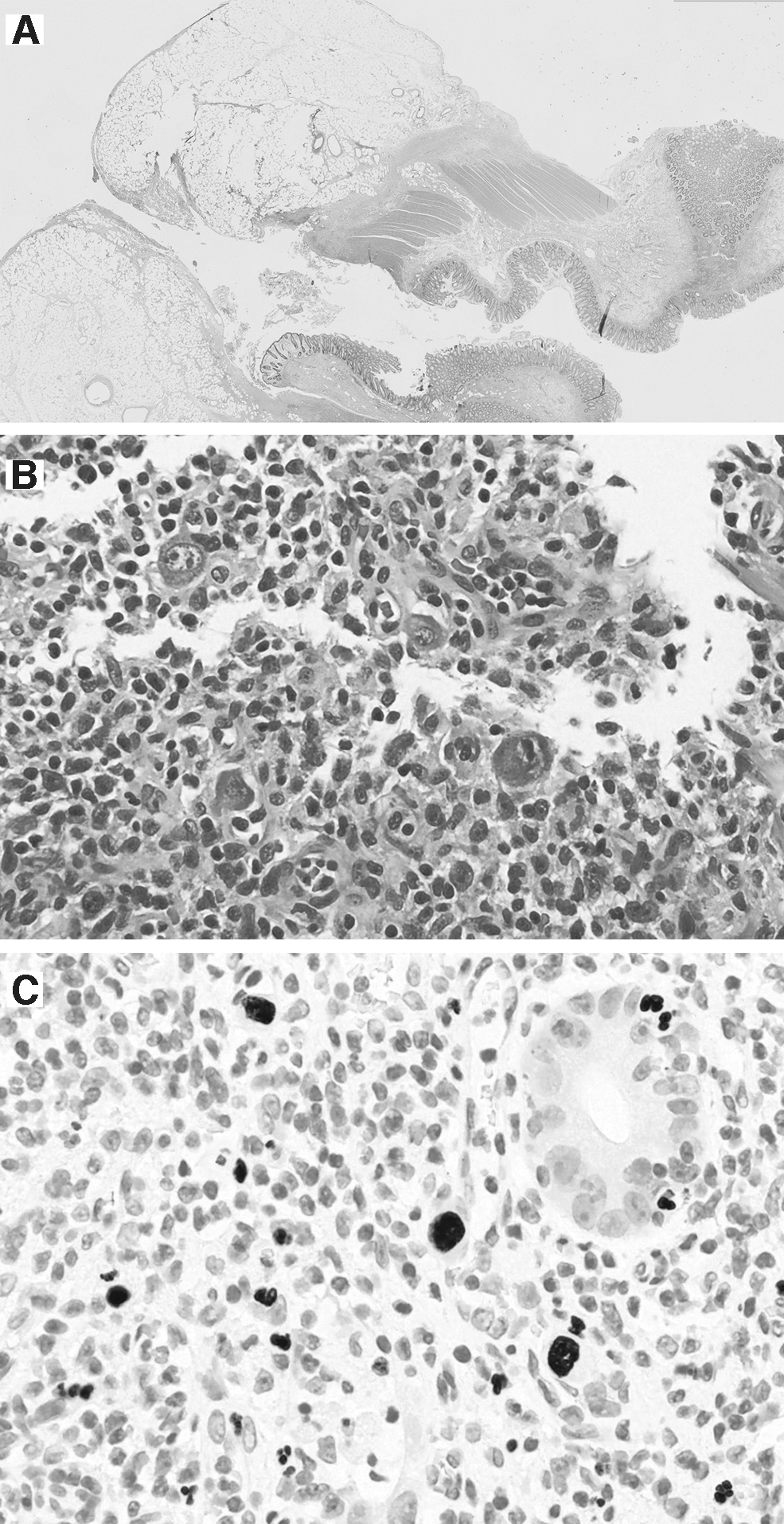
Post-operatively, CMV was suspected. Serum polymerase chain reaction (PCR) returned positive on day 10 after which the patient was started on ganciclovir. Cytomegalovirus titers eventually returned elevated with immunoglobulin G (IgG) 57 AU/mL. Pathologic examination of her colon demonstrated CMV colitis, with CMV inclusion bodies in the mucosa surrounding the colonic perforation (Fig. 2). Of note, the CMV status of the patient's graft was unknown. Although the patient was weaned from sedation on day 13, she remained minimally responsive. Given her pre-operative poor functional status and prolonged hospital course with poor neurologic function, she was transitioned to comfort care. The decision was made to terminally extubate her on day 19.
(
Patients and Methods
A systematic search of PubMed, Embase, and Web of Science was performed for all English-language case reports and clinical studies from database inception to February 2021 describing CMV enterocolitis with bowel perforation (Supplementary Appendix SA1). Patients 18 years of age or older with confirmed CMV enterocolitis and confirmed perforation of the small or large bowel were included. Patients with upper gastrointestinal perforation or bowel perforation attributed primarily to a non-CMV cause (iatrogenic, malignant) were excluded.
For each patient, demographics, comorbid conditions, immunosuppressive and immunomodulatory medications at presentation, perforation location(s), perforation diagnosis method, surgical intervention, CMV treatment and timing (before or after surgery), and mortality were collected. CMV serum markers and cause of death were collected when applicable.
We investigated the associations between comorbidities and survival, diagnostic method and perforation location, and aspects of diagnosis/treatment and survival by odds ratio using logistic regression with p > 0.05 in GraphPad Prism, version 9.1.1 (GraphPad Software, San Diego, CA) for each relevant pair of variables. When perfect separation of values precluded logistic regression, Fisher exact test was used to calculate odds ratio. Effects of age on survival were investigated using Spearman R. Permission to conduct our study was obtained through our university's Institutional Review Board (IRB), which exempted our case report from IRB approval.
Results
Literature search findings
Of the 781 articles found, 77 case reports and case series contained sufficient detail for inclusion (Supplementary Appendix SA2). We excluded observational studies (7 retrieved) because of lack of patient-level information. We also excluded unrelated randomized controlled trials in which CMV enterocolitis perforations were recorded as adverse events (Fig. 3). No prospective studies or randomized controlled trials studying CMV enterocolitis with perforations were found. The median year of publication for included case reports was 2010 (interquartile range [IQR], 21.25 years).
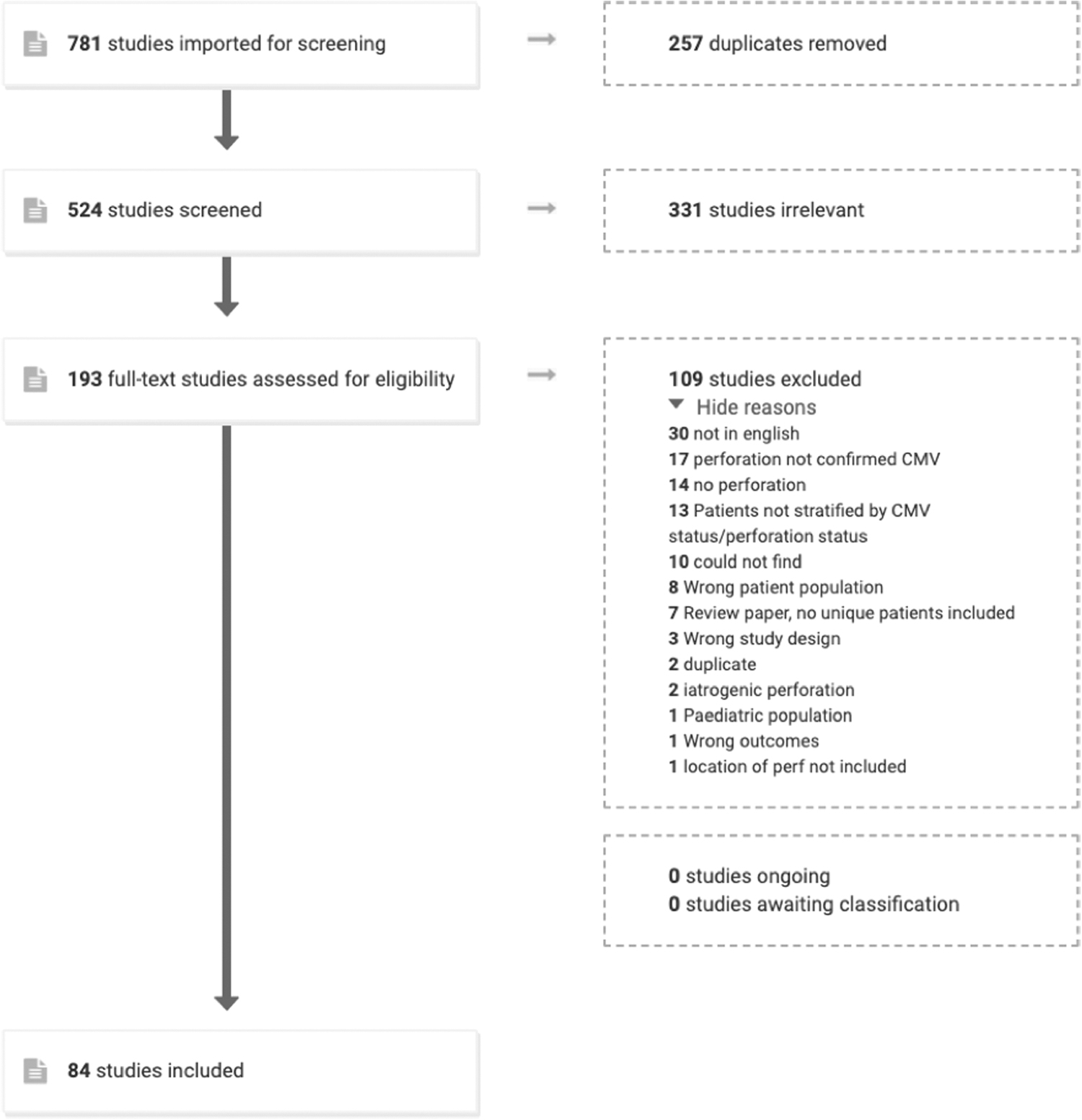
Preferred Reporting of Systematic Reviews and Meta-Analyses (PRISMA) pathway for study inclusion in systematic review.
Demographics and predisposing factors
Eighty-four patients were included. Twenty-seven (32%) were female, and the median age was 52 (range, 19–88) years. Human immunodeficiency virus (HIV) with or without acquired immunodeficiency syndrome (AIDS) was the most prevalent comorbidity (27 patients, 32%) followed by history of kidney transplant (10 patients, 12%). Eleven patients (13%) had no comorbidities. Patients were commonly taking corticosteroids at presentation (37 patients, 44%). Transplant or rheumatologic immunosuppressants constituted the next most common category of medications, followed by chemotherapeutics (Table 1).
Patient Characteristics at Presentation
Medications at time of presentation grouped into common classes.
HIV = human immunodeficiency virus; AIDS = acquired immune deficiency syndrome; SLE = systemic lupus erythematosus; IVIG = Intravenous immunoglobulin; CT = computed tomography; KUB = kidney, ureter, bladder; NOS = not otherwise specified; CMV = cytomegalovirus.
Diagnosis and treatment
Initial diagnosis of the bowel perforation was made radiographically (CT, abdominal or chest plain film) for 57 patients (68%). Bowel perforation was discovered intra-operatively for 15 patients (18%). Most patients underwent laparotomy (73, 87%). When grouped by large bowel, small bowel, and rectum, large bowel perforations predominated (49 patients, 58%). When small bowel was divided into duodenum, jejunum, and ileum, the ileum was the most common site of perforation (26 patients, 31%).
Forty-nine patients (58%) received an antiviral for CMV, the vast majority of whom received ganciclovir (43 patients). Three patients (4%) were documented to have not received an antiviral, and antiviral administration was not reported for the remaining 32 patients (38%). For the majority of those treated, the antiviral was initiated after surgery (30 patients, 65%) rather than before (16 patients, 35%). Serum markers were sometimes reported, with 22 patients (26%) positive for at least one antibody (IgG or IgM) and 42 patients (50%) positive for any serum marker (PCR, antibody, pp56 antigen; Table 2). For 13 patients with CMV serum viral load by PCR reported, 3,900 copies per milliliter was the median viral load (range, 220–272,000 copies per milliliter).
Diagnosis and Treatment of Perforation and CMV
Diagnosis of perforation refers to earliest method of perforation detection.
CMV = cytomegalovirus; PCR = polymerase chain reaction IgM = immunoglobulin M; IgG = immunoglobulin G; NOS = not otherwise specified
Survival
Forty-three patients (51%) were reported to have survived at follow-up after discharge, 31 patients (37%) died, and for 10 patients (12%) survival was not reported. For 34 surviving patients with reported duration of follow-up, mean follow up was 8.06 ± 9.22 months, with range 0.5–36 months. Of 25 patients with cause of death reported sepsis was the most common cause (13 patients, 52%) followed by respiratory failure (8 patients, 32%; Table 3).
Survival
Cause of death percentages calculated as proportion of 25 patients with reported cause of death.
Predictors of survival and diagnostic method
We investigated associations between age, gender, common comorbid conditions (HIV and/or AIDS, kidney transplant, ulcerative colitis or Crohn disease, leukemia or lymphoma, systemic lupus erythematosus), and common immunosuppressants (corticosteroids, cyclosporine, azathioprine, tacrolimus, mycophenolate mofetil) and survival. Human immunodeficiency virus and AIDS were consolidated into a single group for analysis because only four patients had HIV without AIDS. Absence of comorbid conditions was also included as an independent variable. We found that only HIV or AIDS status had a statistically significant correlation with survival with patients with HIV or AIDS less likely to survive (OR, 0.32; 95% CI, 0.11–0.88).
No associations were found between perforation location and whether the perforation was diagnosed radiographically prior to surgery. However, perforation location did correlate with survival. Patients with small bowel perforations were less likely to survive (OR, 0.38; 95% CI, 0.14–0.98), and patients with colonic perforations were more likely to survive (OR, 2.64; 95% CI, 1.03–7.09). Rectal and perforations in multiple locations did not have an association with survival. Other aspects of diagnosis and treatment were investigated for effects on survival: radiographic diagnosis was correlated with survival (OR, 3.45; 95% CI, 1.12–11.60), and antiviral treatment for CMV was associated with survival (OR, 9.19; 95% CI, 3.26–28.48; Table 4).
Correlations with Survival and Diagnostic Methods
For survival: higher OR indicates higher odds of survival. For diagnostic methods: higher OR indicates higher odds of radiographic diagnosis. Non-radiographic diagnostic methods include intra-operative detection and autopsy, and radiographic methods include CT, chest radiograph, or abdominal radiograph. One peritoneal lavage diagnosis was excluded. For association between diagnostic method and survival, patients diagnosed via autopsy were excluded. For anti-CMV timing, patients who received antiviral before surgery were compared with those who started it after surgery. Association of rectal perforation with radiographic diagnosis calculated using Fisher exact test because of perfect separation of variables.
Statistically significant results.
OR = odds ratio; CI = confidence interval; HIV = human immunodeficiency virus; AIDS = acquired immune deficiency syndrome; SLE = systemic lupus erythematosus;CMV = cytomegalovirus; CT = computed tomography.
Discussion
Perforated CMV enterocolitis is uncommon but when reported occurs primarily among immunocompromised or immunosuppressed patients, particularly those with impaired T-cell response. The mortality rate among patients included in our systematic review was 37%, whereas the comparable 30-day post-surgical mortality rate for intestinal perforations of all causes is 10%–15% [9]. The disparity may be attributable to immunocompromised patients' increased susceptibility to infection, given that mortality most often occurred from sepsis. Alternatively, they may be less likely to withstand the stress of peritonitis. Unsurprisingly, HIV/AIDS diagnosis was associated with increased risk of death. A case series from 1990 estimates mortality of perforated CMV enterocolitis in HIV-positive patients to be as high as 87% [10]. However, most included cases were published before 2000, so this high mortality may also reflect higher rates of AIDS and overall poor HIV prognosis in this time period.
The strong association between antiviral treatment for CMV and survival may be skewed by historical factors. Ganciclovir, the first treatment for CMV, was initially used under compassionate use for CMV retinitis through the 1980s, but ethical questions regarding clinical equipoise delayed clinical trials [11]. A randomized controlled trial for ganciclovir in CMV enterocolitis was finally completed in 1993 [12]. Cases reported after the mid-1990s were more likely to have received ganciclovir, and other medical advances may have also boosted survival rates in parallel. Despite historical confounders, ganciclovir may likely affect survival in patients with bowel perforations since untreated CMV risks further gastrointestinal and systemic complications.
Starting antiviral treatment before surgery was not associated with a survival benefit compared to post-operative initiation. However, our patient population was not designed to study whether ganciclovir reduces bowel perforations and subsequently mortality, because only patients with perforations were included. These findings suggest that a high index of suspicion for CMV and even empiric antiviral therapy while awaiting confirmatory testing may improve clinical outcomes in immunocompromised patients with colitis.
Ours is the second reported case of CMV colitis complicated by a missed sigmoid perforation. Toogood et al. [13] describe a 66-year-old male status post-kidney transplant with similar presentation and outcome. Unfortunately, our patient's CMV progressed for 10 days during her admission that could have contributed to her poor outcome. Our systematic review revealed that radiographic diagnosis of perforation was associated with improved survival, likely reflecting the benefit of detection prior to clinical deterioration necessitating exploratory laparotomy. Computed tomography with oral contrast alone is 78% sensitive for gastrointestinal perforations in all locations [14], but factors such as ileus [15] and supine patient positioning [16] can prevent positive oral contrast from reaching distal perforations in sufficient quantity. Intra-rectal contrast is sometimes recommended for detection of distal gastrointestinal tract perforations [17]. In our patient, CT scan with contrast enema in addition to oral contrast may have enabled adequate radiographic visualization of the distal gastrointestinal tract for perforations.
The main limitation of our approach is that case reports are highly subject to publishing bias, limiting the utility of associations discovered by aggregating these patients. Historical shifts in anti-CMV medication and management of HIV/AIDS may also confound results. To our knowledge, this is the only systematic review of perforated CMV colitis, and the most robust studies we found on the topic were small observational studies (5–20 patients). A larger scale observational study could be warranted to investigate whether early initiation of ganciclovir prevents bowel perforation or improves survival in patients with CMV colitis.
Conclusions
Clinicians should have a high index of suspicion for CMV enterocolitis in transplant patients. Despite high mortality from bowel perforations, antiviral treatment may improve survival. Given poor outcomes of perforated CMV enterocolitis, efforts should be made to establish the diagnosis as early as possible, particularly in immunosuppressed patients.
In the event that a suspected gastrointestinal perforation is not found on CT with oral contrast, consider the possibility of a distal gastrointestinal perforation that may be better detected with contrast enema or intra-operative flexible sigmoidoscopy.
Funding Information
No funding was received for this work.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.