
Abstract
Objective:
Reduction of surgical site infection.
Methods:
Retrospective evaluation of a surgical infection prevention program consisting of the gradual introduction of specific infection prevention methods and a surveillance system identifying and reporting on potentially preventable surgical site infections as defined by the omission of a preventive method.
Setting:
A university tertiary referral medical center.
Results:
The sequential introduction of infection prevention elements in the bundle resulted in a fluctuating rate of potentially preventable surgical site infections simultaneously with a slow, gradual reduction of the clean wound SSI rate.
Conclusions:
Change in a complex, multidisciplinary environment such as an inpatient surgical unit happens gradually and requires focused attention and input from all involved professionals.
Surgical site infections (SSIs) are the most common hospital-acquired infections (HAI) accounting for 22%–36% of all HAIs [1,2] and generate the most costs as well. Recently, two comprehensive guidelines for the prevention of SSIs from the U.S. Centers for Disease Control and Prevention (CDC) [3] and the World Health Organization (WHO) [4,5] have been published with Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) level recommendations (Table 1). Each recommended preventive item has compelling evidence for efficacy in reducing SSI risk, but no single item is sufficient to achieve optimal reduction of SSI risk. This requires the combined adherence to multiple preventive efforts to achieve optimal reduction [6,7].
Proven SSI Risk Reduction Measures a
SSI = surgical site infection.
Measures with less strong evidence are indicated by “Consider” whereas measures with stronger evidence simply states the recommended measure.
The necessity to achieve compliance with multiple risk reduction components has motivated a number of investigators to propose the introduction of “bundles” in campaigns to reduce SSIs. Many of these bundles combine a number of elements that have perhaps not been performed as reliably as intended in an effort to improve outcome [8]. In addition, many contain elements that appear logical and are traditional in efforts to reduce SSIs, but that do not have sufficient evidence to be included in the GRADE level recommendations [9] (Table 2). There are published reports of bundles that resulted in a reduction in SSIs [7,10–16], bundles that failed to achieve statistically significant results [17–22], and some bundles that actually resulted in increased SSI rates when the bundle removed proven SSI reduction elements [23]. Introducing bundles and achieving substantial change in procedures can be difficult [8,17], and articles that report compliance with bundles often indicate less than full compliance [20] but often report increasing success in SSI reduction with increased compliance [21,24,25]. Audit and feedback have been found to be useful in improving compliance with preventative measures [21,26–28].
Logical but Unproven Risk Reduction Measures
Methods
Within this context our institution participated in a national project (National Surgical Infection Prevention Collaborative) sponsored by the Centers for Medicaid & Medicare Services (CMS) in 2005 and involving hospitals from 50 states to develop programs to reduce SSIs [29]. Subsequently, in 2005 we initiated the Surgical Infection Prevention Subcommittee (SIPS) of the hospital Infection Prevention Committee in our medical center. This new committee was composed of representatives from each surgical specialty in the hospital and anesthesiology, pre-operative, intra-operative, and recovery room nurses, hospital epidemiologists and infectious diseases faculty, pharmacy, and Central Sterile Supply. The committee met monthly to review SSI data presented by our hospital epidemiologist and to promote the multiple well- established SSI prevention measures. In addition, the committee decided that it would also be of benefit to focus more intensively on a few critical preventative measures.
The following approach was undertaken. Attention was focused on individual preventative measures for monitoring and improving. Each measure was introduced in a stepwise, additive manner. The next measure was only added when the previous one had been implemented successfully. The evaluation of adherence with the preventative measures focused on operations complicated by SSIs. This was a resource conserving approach based on the belief that impediments to adherence could be revealed through thorough analysis of individual SSIs. Each SSI was categorized according to the concept of “potentially preventable” or “apparently unavoidable” based on fulfillment of the preventative measure(s) [30,31]. Surgical site infections categorized as potentially preventable were studied in depth to identify and remediate impediments to adherence. This report is Institutional Review Board exempt because no patient identifiers were available or used in the analysis.
Results
Surgical site infection surveillance was performed during this period on all clean wounds and on targeted clean-contaminated wounds (Table 3). In 2005, we began by focusing on appropriate choice of prophylactic antibiotic agents, appropriate timing for initial dose, and re-dose given at the correct time when indicated. These criteria were audited by our hospital epidemiologist for cases in which an SSI was found. If the above criteria for prophylaxis had been missed at any point, the SSI was categorized as potentially preventable. If all had been done according to correct protocol but an SSI had occurred anyway it was categorized as apparently unavoidable. Each potentially preventable SSI was presented and discussed at the monthly SIPS meeting. Our initial potentially preventable rate for detected SSIs was high at 45% although the overall SSI rate was in a reasonable range (0.83% for clean wounds). We worked on better prophylaxis delivery and brought the potentially preventable rate down.
Surveyed Surgical Wounds
In 2007, we expanded our definition to include normothermia. Failure to meet the antibiotic prophylaxis criteria would still be considered potentially preventable, however, an SSI occurring in a patient arriving in the post-anesthesia care unit (PACU) with a temperature below 36°C would also be categorized as potentially preventable. This brought the potentially preventable rate up, but our clean wound infection rate continued to decrease slowly. Subsequently, in 2010, we added peri-operative glucose control to our definition, defining an SSI as potentially preventable if glucose level exceeded 180 mg/dL within 48 hours post-incision. Over the time that we pursued this sequentially increasing SSI prevention bundle our potentially preventable rates went up and down with the stepwise increase in preventative measures, but our clean wound SSI rate steadily and gradually declined (Fig. 1, Table 4 ).
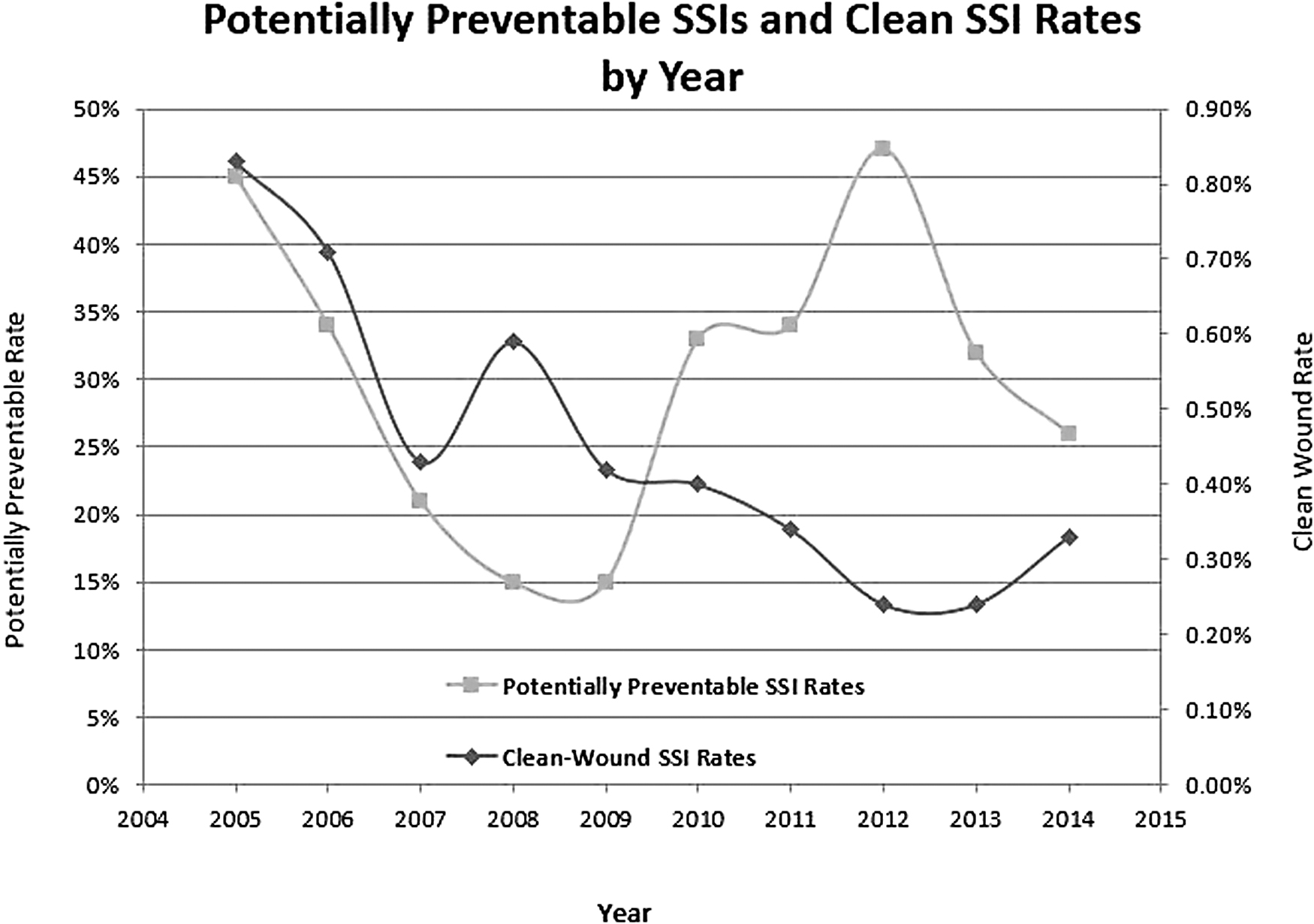
Potentially preventable surgical site infection (SSI) rates represented on left vertical axis and clean wound SSI rates represented on right vertical axis. 2005: Appropriate prophylactic antibiotic, on time, and re-dosed when necessary. 2007: Add first post-operative temperature >36°C. 2010: Add glucose <180 mg/dL for 48 hours post-incision.
Potentially Preventable and Clean Wound Surgical Site Infection Rates
SSI = surgical site infection.
Discussion
This staged introduction of an SSI prevention bundle allowed us to work on one element at a time, recognizing that introducing new modules in a multidisciplinary setting can be difficult, and focusing on one element at a time is helpful. Also, having our hospital epidemiologist focus on auditing performance only on detected SSIs limited the effort required of this professional who had multiple other obligations in a resource limited environment. In addition, by delving into the systemic reasons for the lack of adherence to the preventative measures among the potentially preventable SSIs, we were able to direct our attention to implementing the needed quality improvements. Thus, we achieved better timing on antibiotic prophylaxis administration by moving administration from the pre-operative holding area to the operating room with administration by the anesthesiologist. We obtained more reliable intraoperative redosing with the assistance of an electronic alert system in the anesthesia electronic medical record [32–34]. Normothermia maintenance was assisted by universal warming of all patients in the pre-operative holding area and continued warming in the operating room [35–37]. Prevention of hyperglycemia was assisted by a protocol for obtaining a point-of-care glucose measurement in every patient (both diabetic and non-diabetic) in the pre-operative holding area with standing orders for initiation of insulin infusion for glucose >140 mg/dL and standing orders for control in the operating room [38,39].
Conclusions
Change in a complex, multidisciplinary environment such as an inpatient surgical unit happens gradually and requires focused attention and input from all involved professionals. Through consistent and systematic review of SSI prevention bundle elements, applied in a stepwise approach, our medical center was able to sustain adherence to the selected bundle elements that resulted in a significant reduction in SSI rates for clean wounds and targeted clean-contaminated wounds over a period of 10 years.
Footnotes
Funding Information
There was no financial support from any source for the production of this manuscript.
Author Disclosure Statement
None of the authors have conflicts of interest.