
Abstract
Background:
The principles of antimicrobial stewardship promote the appropriate prescribing of agents with respect to efficacy, safety, duration, and cost. Antibiotic resistance often results from inappropriate use (e.g., indication, selection, duration). We evaluated practice variability in duration of antimicrobials in surgical infection treatment (Rx) or prophylaxis (Px).
Hypothesis:
There is lack of consensus regarding the duration of antibiotic Px and Rx for many common indications.
Methods:
A survey was distributed to the Surgical Infection Society (SIS) regarding the use of antimicrobial agents for a variety of scenarios. Standard descriptive statistics were used to compare survey responses. Heterogeneity among question responses were compared using the Shannon Index, expressed as natural units (nats).
Results:
Sixty-three SIS members responded, most of whom (67%) have held a leadership position within the SIS or contributed as an annual meeting moderator or discussant; 76% have been in practice for more than five years. Regarding peri-operative Px, more than 80% agreed that a single dose is adequate for most indications, with the exceptions of gangrenous cholecystitis (40% single dose, 38% pre-operative +24 hours) and inguinal hernia repair requiring a bowel resection (70% single dose). There was more variability regarding the use of antibiotic Px for various bedside procedures with respondents split between none needed (range, 27%–66%) versus a single dose (range, 31%–67%). Opinions regarding the duration of antimicrobial Rx for hospitalized patients who have undergone a source control operation or procedure varied widely based on indication. Only two of 20 indications achieved more than 60% consensus despite available class 1 evidence: seven days for ventilator-associated pneumonia (77%), and four plus one days for perforated appendicitis (62%).
Conclusions:
Except for peri-operative antibiotic Px, there is little consensus regarding antibiotic duration among surgical infection experts, despite class 1 evidence and several available guidelines. This highlights the need for further high-level research and better dissemination of guidelines.
Starting in 2019, the Scientific Studies Committee (SSC) of the Surgical Infection Society (SIS) began work on reviewing and re-prioritizing the research agenda of the organization. This initiative began by examining the current perception of progress made on the SIS research agenda published in 2006 by Nathens et al. [1,2], led to a narrative review of the current literature developed in support of that research agenda [3], and finally, culminated in the publication in 2021 of a new research agenda for the SIS that was developed using a modified Delphi approach [4]. Whereas the development of a new research agenda was the primary goal of that project, a common theme transcended this 15-year period: Limiting exposure to antimicrobial agents.
Six of the top 15 research questions published in 2021 deal with shortening the duration of antibiotic therapy (Rx) or tactics for avoiding antibiotic agents altogether [4]. Although none of the original questions of Nathens et al. [1,2] carried over into the new research agenda, each of the questions with a similar theme (i.e., limiting exposure to antimicrobial agents) were believed by a majority of current participants to be important for further research [2]. However, this seems to contradict available data regarding the appropriate duration of antibiotic Rx for surgical conditions encountered commonly, perhaps mirroring the current landscape among United States physicians.
When physicians in the United States are surveyed regarding the overuse of antibiotic agents and the importance of antibiotic resistance, the vast majority perceive it as an important national problem [5,6]. However, fewer perceived it as a problem at their institution (55%) or favored restricting the use of broad-spectrum antibiotics (60%) [5]. Many also admitted to prescribing antibiotic agents when the clinical evidence was unclear because of anxiety about missing an infection [6]. Using this discordance between physician perceptions of antibiotic resistance and their own prescribing patterns as a framework, we examined the self-reported antibiotic prescribing patterns of the SIS membership for common clinical scenarios encountered in surgical practice, with the goal of identifying potential high-priority questions for further research. We hypothesized that many of the clinical scenarios presented would have no clear consensus on the appropriate duration of antibiotic Rx, and that inter-respondent variability would be high.
Methods
This survey, designed by the SIS-SSC, was Internet-based and hosted by Google Forms (Alphabet, Inc., Mountain View, CA) between November 1, 2020 and March 31, 2021. A link to the survey was distributed to all members of the SIS via e-mail with periodic reminders to encourage participation. The goal of the survey was to determine areas of consensus and equipoise regarding antimicrobial durations for common clinical scenarios.
Demographic data (including names and e-mail addresses) were collected for each participant to ensure that duplicate respondents could be recognized. In the event of duplicate respondents, the survey response with the most recent timestamp was used. Survey responses were de-identified prior to final data analysis. Additional demographic data collected included previous positions or roles within the SIS, years of post-residency experience, nature of clinical practice, world region, and primary practice location. Primary practice location was used to determine the U.S. geographical region where applicable.
Respondents were first surveyed regarding their use of prophylactic (Px) antibiotic or antifungal agents in common clinical scenarios in which clinicians might utilize antibiotic Px or Rx. They were asked to consider the tactics they would most likely use, and not necessarily the most common scenario they have witnessed at their institution. This included the use of first-/second-generation cephalosporins for skin Px of common operations and common bedside procedures. Respondents were also asked to consider the use of broad-spectrum antibiotic agents in the peri-operative period for a variety of disease entities, and the use of antifungal Rx for common disease entities.
Next, the respondents were given 20 different clinical scenarios and they were asked to provide the duration of antibiotic therapy that they would use “most commonly.” Antibiotic duration choices were presented in categorical format allowing only one answer per scenario. Each question specified whether or not the infection involved a multi-drug–resistant organism (MDRO) and if the patient was immunocompetent. Finally, respondents were asked to provide an estimate for the quality of evidence and the importance of further study for each clinical scenario. Each of these questions was presented in a five-point Likert scale format.
Variables were reported as either means with standard deviation (SD) or counts with percentages for continuous and categorical data, respectively. Answer choices were compared by both U.S. geographic region and years of post-residency experience. p values were calculated using the χ2 test of independence. The Shannon Index was used to calculate data heterogeneity for each categorical antibiotic duration and reported as nats or natural units. This measurement was described in 1948 by Claude Shannon to quantify the degree of entropy within a set of data [7]. In its original application, the Shannon Index provided a measurement of uncertainty when predicting the next letter in a string of text by taking into account both the number of different letters in the dataset and the proportional abundance of each of those letters. As the number of letters in the dataset increases and as the proportion of each of those becomes more equal, it will be more difficult to predict accurately what the next letter will be. The Shannon Index will have a range from 0 (a theoretic dataset with only one possible letter and no uncertainty of what the next letter will be) to the natural log of the number of possible letters (a theoretic dataset with multiple letters appearing in equal proportions and maximum uncertainty regarding what the next letter will be).
Since its original description, the Shannon Index has been used widely in ecology as a method for quantifying population diversity [8]. For the purposes of this article, it is a measurement of heterogeneity; a lower value signals more agreement among respondents. Linear relations between variables were assessed by the Pearson correlation. All statistical analyses were performed in R 4.0.3 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Eighty-three survey responses were used in the final analysis; 19 survey responses were excluded secondary to respondent duplication, with only the most recent response being included. The majority of respondents were from the United States (n = 76; 92%), identified as academic clinical faculty (n = 66; 80%), and had served in some capacity within the SIS (n = 52; 63%). Geographic region and years of post-residency experience were more evenly distributed though the most common practice duration was more than 15 years (49%) and the most common U.S. geographical region was the Midwest (35%). The remaining demographic data can be found in Table 1.
Participant Demographics
SIS = Surgical Infection Society; NA = not available.
Skin prophylaxis
Whereas respondents reported using at least a single dose of first-/second-generation cephalosporin for procedures performed in the operating room (range, 88%–100%), bedside procedures were frequently performed without any antibiotic Px (range, 30%–65%; Fig. 1). With the exception of gangrenous cholecystitis (42%), more than two-thirds of respondents reported needing only a single dose of antibiotic with the remaining operating room procedures. As the perceived severity of illness increased, the reported use of more than a single dose of antibiotic increased (e.g., elective cholecystectomy [3.6%], acute cholecystitis [23.6%], and gangrenous cholecystitis [57.0%]). There was less consensus regarding the use of duration of antimicrobial skin Px for bedside procedures than operating room procedures as shown by a higher average Shannon Index (0.59 nats vs. 0.87 nats). Intracranial pressure monitors (“bolt” 69% and extraventricular drain 70%) were the only responses in which a majority of respondents reported using any duration of antimicrobial Px for bedside procedures. Responses for skin Px are shown in Figure 2.
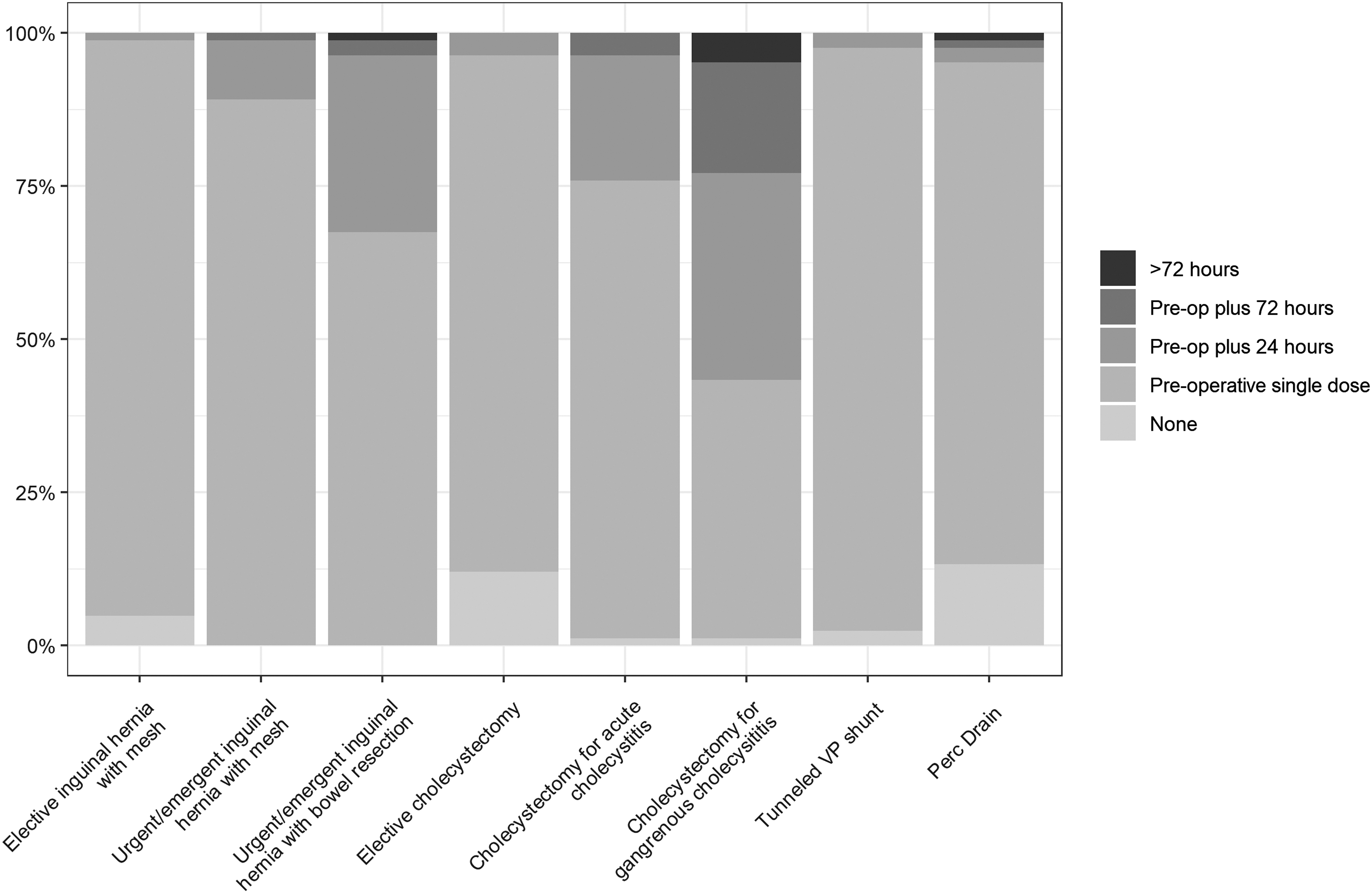
Commonly used durations of first- or second-generation cephalosporins for skin prophylaxis in operative procedures. Shannon Index (nats) for each of the above listed procedures (from left to right): 0.26, 0.38, 0.77, 0.52, 0.72, 1.24, 0.23, 0.63. nats = natural units; VP = ventriculoperitoneal; Perc = percutaneous; Pre-op = pre-operative.

Commonly used durations of first- or second-generation cephalosporins for skin prophylaxis in bedside procedures. Shannon Index (nats) for each of the above listed procedures (from left to right): 0.90, 0.89, 0.79, 0.84, 0.88, 0.84, 0.97. nats = natural units; ED = emergency department; ICP = intracranial pressure; IR = interventional radiology.
Antifungal and broad-spectrum antibacterial agents in the peri-operative period
Compared with the use of cephalosporins for skin Px, the use of broad-spectrum antibiotic agents in the peri-operative period showed less consensus regarding duration of Rx. Whereas three of the surveyed conditions had greater than 50% agreement on antibiotic duration, namely, single pre-operative dose for facial fractures and four plus one days [9] of antibiotic agent(s) for operative duodenal and gastric perforation, the remainder did not. For none of the conditions surveyed did more than two-thirds of respondents use a specific antibiotic duration (Fig. 3). For Hinchey 1 and Hinchey 2 diverticulitis, most respondents believed that antibiotic agents should be used at least until source control was achieved (82% and 87%, respectively). However, there was a nearly even split between duration of antibiotic therapy after source control between none, four days, seven days, and more than days for both conditions. This was reflected by both Hinchey 1 and Hinchey 2 diverticulitis having the highest degree of heterogeneity among the surveyed conditions.

Commonly used durations of broad-spectrum antibiotic(s) for surgical prophylaxis. Shannon Index (nats) for each of the above listed procedures (from left to right): 1.34, 1.50, 1.25, 1.26, 1.75, 1.68. nats = natural units; Fx = open reduction of fracture; Perf = perforation; Pre-op = pre-operative. *Diverticulitis is considered non-operative and not requiring a drain placement.
Respondents were also surveyed regarding the use of antifungal Rx. A majority of respondents believed that the routine use of antifungal agents was unnecessary in gastric perforation (51%), duodenal perforation (58%), Hinchey 1–2 diverticulitis (92%), Hinchey 3–4 diverticulitis (89%), and neutropenic enterocolitis (52%). There was less consensus among patients presenting from a nursing home where the use of antifungal agents was used more commonly (Fig. 4); respondents used antifungal agents commonly for both gastric perforations (61%) and duodenal perforations (57%) in this patient population.

Commonly used durations of antifungal prophylaxis in surgical conditions. Shannon Index (nats) for each of the above listed procedures (from left to right): 1.35, 1.24, 1.49, 1.43, 0.36, 0.49, 1.35. nats = natural units; *Nursing home = admitted from the facility.
Antibiotic duration scenarios
For this section of the survey, respondents were given a series of clinical scenarios and asked to give the antibiotic duration that they used “most commonly” as well as to consider the importance of clinical research on the topic and the quality of existing data. Of the 20 clinical scenarios given, there were only five in which more than 50% of respondents chose a single antibiotic duration (Tables 2 and 3): Tokyo-3 acute cholecystitis [10] after percutaneous cholecystostomy (4 + 1 days; 53%), index presentation of ventilator-associated pneumonia (VAP; 7 days; 72%), recurrent VAP (7 days; 51%), perforated appendicitis after successful appendectomy (4 + 1 days; 57%), and osteomyelitis without debridement (6 weeks; 52%). The lowest amount of heterogeneity was seen for index presentation VAP (0.86 nats), and the highest amount of heterogeneity was seen in necrotizing soft tissue infections (NSTIs) after definitive debridement (1.9 nats). Perforated appendicitis after successful appendectomy in the immunocompromised patient and bacterial liver abscesses after successful percutaneous drainage also showed a high degree of heterogeneity (1.74 and 1.79 nats, respectively).
Antibiotic Duration, Perceived Quality of Available Data, Perceived Importance of Continued Research, and Respondent Heterogeneity for Commonly Encountered Surgical Conditions
nats = natural units; NSTI = necrotizing soft tissue infection; cIAI = complex intra-abdominal infection; perc = percutaneous; chole tube = cholecystostomy; VAP = ventilator-associated pneumonia;, MDR = multi-drug–resistant.
Antibiotic Duration, Perceived Quality of Available Data, Perceived Importance of Continued Research, and Respondent Heterogeneity for Bacteremia and Osteomyelitis
cx = culture; nats = natural units; GNR = gram-negative rod; GPC = gram-positive cocci; MRSA = methicillin-resistant Staphylococcus aureus; NA = not available.
Participants were also asked to rank the importance of continued research in each of the clinical scenarios as well as the quality of the current evidence. The five questions with the highest mean importance scores were related to complex intra-abdominal infections (cIAI) in which source control is not possible (4.19 ± 1.05), NSTI after definitive debridement (4.18 ± 1.01), persistent cIAI with failure of index source control with one drain in place (4.08 ± 1.00), recurrent cIAI with failure of index source control and two drains in place (3.86 ± 1.00), and septic shock from gram-negative rod (GNR) bacteremia (3.76 ± 0.94). Except for GNR bacteremia, all of these clinical scenarios also had a mean data quality score of less than 2.5. There was a positive correlation between the heterogeneity of answer choices and the perceived importance of research on the topic (R2 = 0.235; p = 0.03). Similarly, as the heterogeneity of survey answers increased, the perceived quality of current data related to the clinical scenario decreased (R2 = 0.46; p = 0.001).
Differences in geographic region and years of post-residency experience
Survey participants were then divided by categorical years of post-residency experience and U.S. geographic region to look for patterns of practice regarding each of the surveyed topics. In general, there were few statistically significant differences among the distributions of answer choices.
When subdivided by years of post-residency experience, the use of antifungal Rx in duodenal perforations (p = 0.012) and antibiotic duration in recurrent VAP (p = 0.002) showed variable answer distributions. For the former, those respondents with 15 years or more of post-residency experience were less likely to use antifungal agents (76% reported never) compared with younger surgeons (still in training: 0; <1 to 4 years: 18%; 5–9 years: 45%; 10–14 years: 29%). For the latter, those respondents with 15 years or more of post-residency experience were less likely to use a set duration of more than seven days of antibiotic agent(s) for recurrent VAP (22%) compared with surgeons with less experience (still in training: 50%; <1 to 4 years: 64%; 5–9 years: 41%; 10–14 years: 29%).
When regional differences were examined, cIAI with no source control (p = 0.03), multi-drug–resistant Pseudomonas VAP (p = 0.027), and perforated appendicitis after successful appendectomy (p = 0.034) were found to have significant differences in answer ranking. For cIAI, respondents from the Northeast and Southeast regions were more likely to use antibiotic agents for a set duration of seven days (67% and 57%, respectively), whereas respondents from other geographic regions were more likely to continue antibiotic agents “until clinical resolution” (Midwest: 48%; Southwest: 50%; West: 55%). Regarding multi-drug–resistant Pseudomonas VAP, respondents from the Midwest, Northeast, and Southwest regions were most likely to treat for 14 days (41%, 58%, and 70%, respectively) compared with the West where respondents reported treating “until clinical resolution” (55%). The Southeast, on the other hand, was evenly split among seven days (36%), 10 days (21%), and 14 days (29%). Finally, for perforated appendicitis, a majority of respondents from the Midwest, Northeast, and Southwest treated commonly with four plus one days of antibiotic agents (62%, 58%, and 90%, respectively); the Southeast was split between 24 hours (50%) and four plus one days (43%); and the West was split between four plus one days (45%) and 72 hours (36%).
Discussion
This study offers an interesting perspective on antibiotic prescribing patterns among members of the surgical community in the United States. Overall, it highlights significant practice variability even among members of the SIS, a society dedicated to the study and dissemination of research and best practices related to infectious diseases among surgical patients. Whereas many of the scenarios were selected purposely because of anticipated controversy, there was little consensus among any of the provided responses. Furthermore, this variability in practice was mirrored by a perception that data on the subject are lacking. Many of the topics covered during the survey would be prime targets for either the development of guidelines for appropriate antibiotic duration or clinical trials examining the optimal, minimum antibiotic duration for certain infections.
Pre-operative antibiotic Px was perhaps the area of the study with the largest degree of consensus among participants. More than two-thirds of participants opined that a single dose of pre-operative antibiotic agent(s) was sufficient for a majority of operating room procedures surveyed (elective inguinal hernia repair, urgent inguinal hernia repair, elective cholecystectomy, cholecystectomy for acute cholecystitis and gangrenous acute cholecystitis, and intra-peritoneal drain placement). This is relatively unsurprising considering that the World Health Organization [11], American College of Surgeons/SIS [12], U.S. Centers for Disease Control and Prevention [13], and the American Society of Health-System Pharmacists/Infectious Diseases Society of America/SIS/The Society for Healthcare Epidemiology of America [14] have all published guidelines recommending the cessation of antibiotic agents after a single dose or no more than 24 hours post-procedure. However, consensus decreased as the perceived complexity/risk of the case increased. For gangrenous cholecystitis, only 42% of participants opined that a single dose of pre-operative antibiotic Px was appropriate, 34% believed the need to continue antibiotic agent(s) for 24 hours post-operatively, and nearly one-quarter (23%) believed that a duration more than 24 hours was necessary. Whereas one could argue that longer duration of antibiotic agent(s) may be indicated for gangrenous acute cholecystitis based on the Tokyo Guidelines [10], the distribution of answers did not seem consistent in this paradigm, as only 4.8% of participants reported the routine use of longer than 72 hours of antibiotic agent(s) in this scenario. It is perhaps likely that this ostensible behavior represents the fear of missing an infection more than the fear of potential risks of extended antibiotic duration, consistent with previously surveyed physician prescribing patterns [6].
Both Px and Rx with antifungal agents was rejected almost ubiquitously for cases of diverticulitis, but participants were varied in their approach to foregut perforations. Interestingly, the only randomized controlled trial to specifically look at antifungal Px in intra-abdominal perforations showed no difference in mortality [15], and there are no randomized trials supporting the use of empiric antifungal agents specifically in perforated peptic ulcer disease [16]. In fact, there is strong inferential data from multiple studies suggesting antibacterial agents alone (without empiric antifungal Rx) can be used to treat cIAI adequately [17–20]. Despite no significant evidence to support the use of antifungal Rx in foregut perforations, between 42% and 61% of participants reported the routine use of some duration of antifungal Rx for duodenal or gastric perforations, depending on the clinical scenario. Again, this emphasizes that the fear of missing an infection may outweigh any fear of overuse of antimicrobial agents when specific guidance is lacking.
The lack of consensus among the 20 clinical scenarios examined in the survey may offer a framework for further research. All five clinical scenarios with more than 50% consensus regarding antibiotic duration had corresponding guidelines from reputable medical societies to support a specific duration: complicated cholecystitis [10,21], VAP/recurrent VAP [22,23], appendicitis [21,24,25], and osteomyelitis [26]. On the surface, this may suggest that increased research or the development of societal guidelines may lead to better consistency in practice patterns. However, with the exception of neutropenic enterocolitis and pyogenic liver abscesses, each of the theoretic scenarios already have clinical practice guidelines that offer a suggested duration of antibiotic Rx (Table 4) and could be used to inform clinical decisions about the duration of antibiotic Rx [10,11,12–14,22–25,27–32]. Clearly there is a disconnect between clinical practice guidelines and the common antibiotic prescribing practices of treating providers.
Summary of Current Guidelines Regarding Antibiotic Durations in Commonly Encountered Surgical Procedures
IAI = intra-abdominal infection; VAP = ventilator-associated pneumonia; ICU = intensive care unit; NVO = native vertebral osteomyelitis; MRSA = methicillin-resistant Staphylococcus aureus.
The main limitations of this study are related to the selection of survey respondents and survey question design. The clinical scenarios presented were not tested prior to deployment for reliability among varying participants. It is possible that the clinical scenarios were interpreted differently by individual respondents. However, most of the clinical scenarios presented were straightforward and unlikely to be interpreted ambiguously. The survey was also unable to ascertain why individuals opined that a particular antibiotic duration was appropriate for each scenario, limiting our ability to determine any causation for answer variability. Whereas there were some statistically significant differences among respondents based on years of post-residency experience or geographic region, there is no discernable pattern to those differences. Finally, an argument could be made that this survey population does not represent the practice patterns of the general surgical community. However, considering that all of the participants were active or former members of the SIS, our assumption is that the larger population likely has greater heterogeneity than the SIS member-respondents, whose interests are related specifically to surgical infections.
It is difficult to know the increase in life expectancy attributable to the development of antibiotics. In the last 100 years, average life expectancy has increased by almost 40 years and communicable diseases such as pneumonia and tuberculosis no longer are represented in the top five causes of death [33–35]. However, the rise of MDRO could be changing that landscape. Between 11% and 17% of admissions related to bacterial infections are now suspected to involve one or more MDRO, and the estimated annual cost of treating MDRO is now estimated at over $2 billion annually, a doubling since 2002 [36,37]. Prevention of further increases in antibiotic resistance is seated in appropriate antibiotic stewardship (i.e., appropriate indications, antibiotic selection, and duration).
Limiting the use of broad-spectrum antibiotic agents is a primary focus of many antibiotic stewardship programs, but it is a difficult factor to control without rapid diagnostic testing and in a landscape of increasing MDROs. Limiting duration of antibiotic therapy and thereby limiting overall antibiotic exposure are equally important aspects of antibiotic stewardship that are well supported by data. For nearly every indication that has been studied adequately—community-acquired pneumonia [38–45], cIAI [9,46], VAP [47–50], osteomyelitis [51], pyelonephritis/complicated urinary tract infections [52–57], sinusitis [58], cellulitis [59–62], and primary bacterial peritonitis [63]—a shorter duration of antibiotic Rx has been shown to be at least equivalent to longer duration Rx.
In conclusion, this study revealed a lack of consensus about the duration of antimicrobial Rx and, to a lesser degree Px, for commonly encountered clinical scenarios. Although these data represent self-reported, rather than actual, prescribing patterns, the heterogeneity of responses is concerning. If corroborated, it implies that many infectious diseases may be treated with an inappropriate (i.e., overly long) duration of Rx. There is a clear need to either generate more data or disseminate existing data better for the topics with the greatest heterogeneity, highest average importance score, and lowest perceived available data (e.g., NSTIs).
Scientific Studies Committee of the Surgical Infection Society
Philip S. Barie, Weill Cornell Medicine; L. Andrew O. Benedict, St. Luke s Hospital; Philip A. Efron, University of Florida College of Medicine; Christopher A. Guidry, University of Kansas Medical Center; Haytham M.A. Kaafarani, Massachusetts General Hospital; Dennis Kim, Harbor-UCLA Medical Center; Michele M. Loor, Baylor College of Medicine; David Machado-Aranda, Michigan Medicine and Veteran's Affairs Healthcare System; Tina S. Mele, Schulich School of Medicine and Dentistry; April E. Mendoza, Massachusetts General Hospital; Gareth Morris-Stiff, Case Western Reserve University; Rishi Rattan, University of Miami Miller School of Medicine; Sebastian D. Schubl, University of California, Irvine; Jeffrey S. Upperman, Monroe Carell Jr. Children's Hospital at Vanderbilt.
Footnotes
Acknowledgments
This article was a co-recipient of the award for Best Paper Presentation by a resident physician.
Funding Information
No funding was received.
Author Disclosure Statement
None of the authors of this paper have relevant financial disclosures related to this project. As a voluntary, survey-based study, this study is exempt from institutional board review.