
Abstract
Background:
Necrotizing soft tissue infections (NSTIs) require prompt surgical debridement and antimicrobial therapy. Indicated antimicrobial therapy involves broad-spectrum coverage against common pathogens and toxin inhibition. Linezolid provides both methicillin-resistant Staphylococcus aureus (MRSA) coverage and toxin inhibition, however, there is limited evidence evaluating its role in empiric treatment. The purpose of this study was to evaluate the impact of empiric linezolid use for NSTIs on the total duration of MRSA-active therapy.
Patients and Methods:
This retrospective, single-center study included adult surgical intensive care unit (ICU) patients treated with empiric vancomycin and clindamycin or linezolid along with gram-negative and anaerobe coverage for NSTIs. The primary end point of this study was the duration of MRSA-active therapy. Secondary end points included ICU and hospital length of stay (LOS; days), new-onset acute kidney injury (AKI), and Clostridioides difficile infection (CDI).
Results:
There were 21 patients in the vancomycin/clindamycin cohort and 28 patients in the linezolid cohort. The average duration of vancomycin was 3.9 days versus 2.9 days of linezolid (p = 0.04). The average hospital LOS for the vancomycin/clindamycin cohort was somewhat longer than the linezolid cohort, although the difference was not statistically significant (p = 0.07), and the incidence of new-onset AKI during hospitalization was higher in the vancomycin/clindamycin cohort (38.1% vs. 0%; p < 0.001). No differences were observed for ICU LOS or CDI.
Conclusions:
Empiric linezolid use for NSTI was associated with one less day of MRSA-active therapy and lower incidence of new-onset AKI during hospitalization. Linezolid was a safe and effective alternative to vancomycin/clindamycin for empiric treatment of NSTIs.
Necrotizing soft tissue infections (NSTIs) represent rapidly progressive conditions with high morbidity and mortality. In the United States, mortality rates have been reported up to 25% and approximately 50% of NSTI cases are associated with complications [1]. Selection of empiric antimicrobial regimens with appropriate spectrum of activity and ability to impede toxin production along with prompt surgical intervention are essential to NSTI management. Necrotizing soft tissue infections are classified as type 1, type 2, or type 3 based on the causative pathogens, and the toxins produced by these pathogens vary with each classification (Table 1) [1–4]. Antimicrobial regimens include agents with broad gram-positive, gram-negative, and anaerobic coverage along with an agent to inhibit production of toxins. When NSTI is suspected, a typical empiric antibiotic regimen includes piperacillin-tazobactam, vancomycin, and clindamycin [5].
Types of Necrotizing Soft Tissue Infections
Linezolid may be used empirically for NSTI to replace both vancomycin and clindamycin for methicillin-resistant Staphylococcus aureus (MRSA) and toxin coverage, however, there is a lack of data evaluating the efficacy of linezolid compared with vancomycin and clindamycin. Linezolid has demonstrated inhibition of bacterial exotoxin production comparable to clindamycin and has shown improved clinical cure rates and reduced adverse effects in comparison to vancomycin in several trials for the treatment of skin and soft tissue infections [6–8]. Clindamycin, however, is not recommended for empiric use for both MRSA and exotoxin coverage and use requires a two-drug regimen in combination with vancomycin. Clinical guidelines recognize linezolid as an alternative, one-drug therapy for coverage of MRSA and discuss its potential role against toxins, however, guideline recommendations do cite limited evidence for use of linezolid as a first-line empiric agent [9,10].
This study aims to compare outcomes associated with empiric linezolid versus vancomycin and clindamycin-containing regimens for treatment of NSTI. The authors hypothesized that linezolid use would be associated with a shorter duration of MRSA-active therapy and similar patient outcomes.
Materials and Methods
Study design
This was a retrospective, single-center, quasi-experimental study performed at a tertiary academic medical center. The study population included adult subjects with NSTI who were treated empirically with either intravenous vancomycin and clindamycin or linezolid along with gram-negative and anaerobe antimicrobial coverage in the surgical or trauma intensive care units (ICUs). Diagnostic International Classification of Diseases-10 (ICD-10) codes and procedural Current Procedural Terminology codes were used to confirm NSTI diagnosis. The vancomycin/clindamycin cohort consisted of subjects who received vancomycin and clindamycin as part of empiric NSTI antibiotic regimens from July 1, 2016 through June 30, 2017. The linezolid cohort included subjects who received linezolid as part of empiric NSTI antibiotic regimens from July 1, 2018 through December 31, 2020. A one-year washout period was utilized to account for the implementation of linezolid use empirically into practice.
Subjects were divided into cohorts as receiving vancomycin/clindamycin or linezolid. Patients receiving vancomycin for more than 48 hours and switched to linezolid were excluded. Patients who received MRSA-active therapy for more than 14 days were also excluded. The investigators excluded patients requiring prolonged durations of MRSA-active therapy to avoid including patients receiving definitive therapy for deep seated MRSA infections. Baseline characteristics collected for each of the cohorts included age, gender, Sequential Organ Failure Assessment (SOFA) scores on ICU admission and discharge, vasopressor use and duration, ventilator use and duration, and baseline renal dysfunction. In addition, deep wound cultures performed in the operating room (OR) were collected.
At the institution, broad empiric antibiotic agents were started on all patients with suspected NSTI. After surgical debridement, the surgical team evaluated the nature of the infection and the need for toxin coverage. Culture results from the OR debridement subsequently determined the appropriate definitive therapy for patients with NSTI. However, discontinuation was encouraged after the completion of all surgical debridements with appropriate source control. In 2018, to adjust to shortages, restrictions on linezolid use in the ICU were adjusted from requiring pre-approval to allowing 72 hours of empiric use. The trauma and acute care surgery and ICU teams adjusted their antibiotic protocol to include linezolid as a first-line agent. This study was approved by the UF Health Sebastian Ferrero Office of Clinical Quality & Patient Safety in Gainesville, Florida (project ID: 1375).
Outcomes
The primary end point of the study was the duration of MRSA-active therapy in the vancomycin/clindamycin cohort versus the linezolid cohort. Secondary end points measured included number of surgical debridements, total duration of antibiotic therapy (days), ICU length of stay (days), hospital length of stay (days), incidence of new-onset acute kidney injury (AKI) as defined by Kidney Disease Improving Global Outcomes (KDIGO) guideline criteria after the initiation of antibiotics, and incidence of Clostridioides difficile infection (CDI) after antibiotic administration as defined by ICD-10 codes and positive toxin polymerase chain reaction (PCR) test during the hospital stay [11–14]. Operative wound cultures were also obtained.
Statistical analysis
End points were classified as either continuous or categorical variables. The continuous variables were analyzed using Student t-test or Wilcoxon rank sum/Kruskal-Wallis tests for median and interquartile range (IQR) values. The categorical variables were analyzed using either χ2 or Fisher exact test. Normally distributed continuous variables were described with mean and standard deviation. Categorical variables were described using n (number of subjects) and percentage. Median and IQR were used to represent number of surgical debridements for each cohort. Statistical significance for analysis was determined using a p value (α) < 0.05. All statistical analyses were performed using JMP Pro 15.0 Software (SAS Institute Inc., Cary, NC).
Results
There were 181 subjects evaluated for inclusion in this study; 49 subjects met inclusion criteria, with 21 subjects in the vancomycin/clindamycin cohort and 28 subjects in the linezolid cohort. Reasons for exclusion were vancomycin administration for longer than 48 hours prior to linezolid (n = 120), and a MRSA-active agent administered for more than 14 days (n = 12) (Fig. 1). Baseline characteristics were comparable between the two groups (Table 2). The average age in the vancomycin/clindamycin cohort was 52 ± 14 years versus 53 ± 16 years in the linezolid cohort. Both cohorts had more male subjects than female subjects. Twelve subjects had baseline renal dysfunction with chronic kidney disease. Additionally, SOFA scores on both ICU admission and ICU discharge were similar between cohorts. Ventilator and vasopressor use and duration were not found to be significantly different between both groups. Further comparisons are displayed in Table 2.
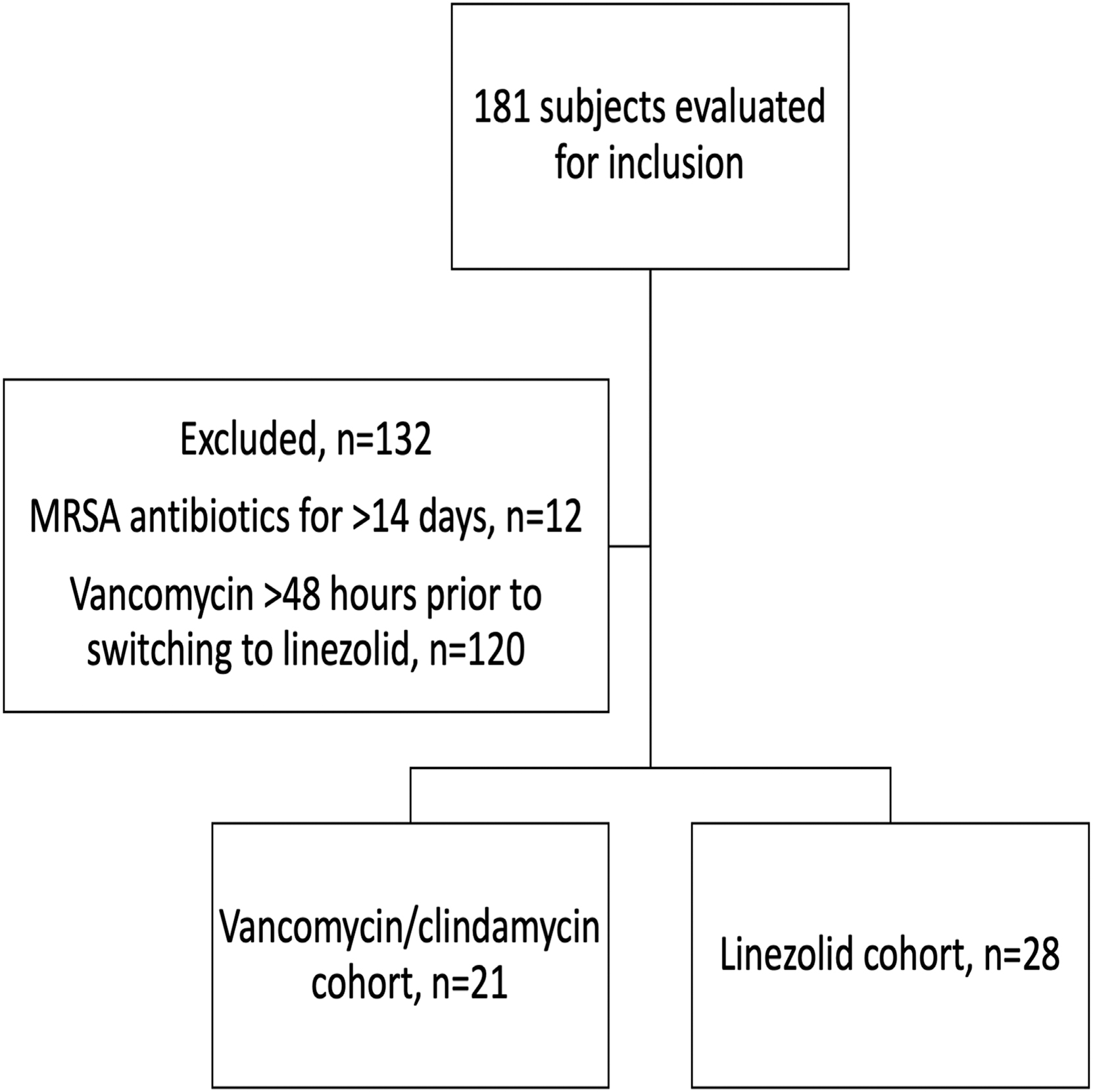
Flow chart of patient inclusion in the study. LZD = linezolid; VAN = vancomycin; CLI = clindamycin.
Baseline Characteristics
VAN = vancomycin; CLI = clindamycin; LZD = linezolid; SOFA = Sequential Organ Failure Assessment; ICU = intensive care unit.
n (%)
Mean
Median (interquartile range).
For the primary end point of duration of MRSA-active therapy, the vancomycin/clindamycin cohort was found to have a longer duration of therapy compared with the linezolid cohort (3.9 ± 2.9 days vs. 2.9 ± 0.9 days; p = 0.04). Regarding the secondary end points, there were no significant differences found between the cohorts for hospital or ICU length of stay, duration of antimicrobial therapy, or antimicrobial duration after last surgical debridement (Table 3).
Secondary End Points
VAN = vancomycin; CLI = clindamycin; LZD = linezolid; ICU = intensive care unit; AKI = acute kidney injury; CKD = chronic kidney disease.
n (%)
Median interquartile range.
The median number of surgical debridements was one for the vancomycin/clindamycin cohort and two for the linezolid cohort. The incidence of new-onset AKI inpatient was found to be higher in the vancomycin/clindamycin cohort compared with the linezolid cohort (8 [38.1%] vs. 0 [0%]; p = 0.0005). There were two confirmed cases of CDI in the vancomycin/clindamycin cohort and none in the linezolid cohort. The most common deep wound pathogens included Candida glabrata, Escherichia coli, and Serratia marcescens in the vancomycin/clindamycin cohort and Proteus mirabilis and Klebsiella pneumoniae in the linezolid cohort (Fig. 2). There were four subjects with Fournier's gangrene. Of note, there were no positive MRSA cultures recorded for any subjects in this study.
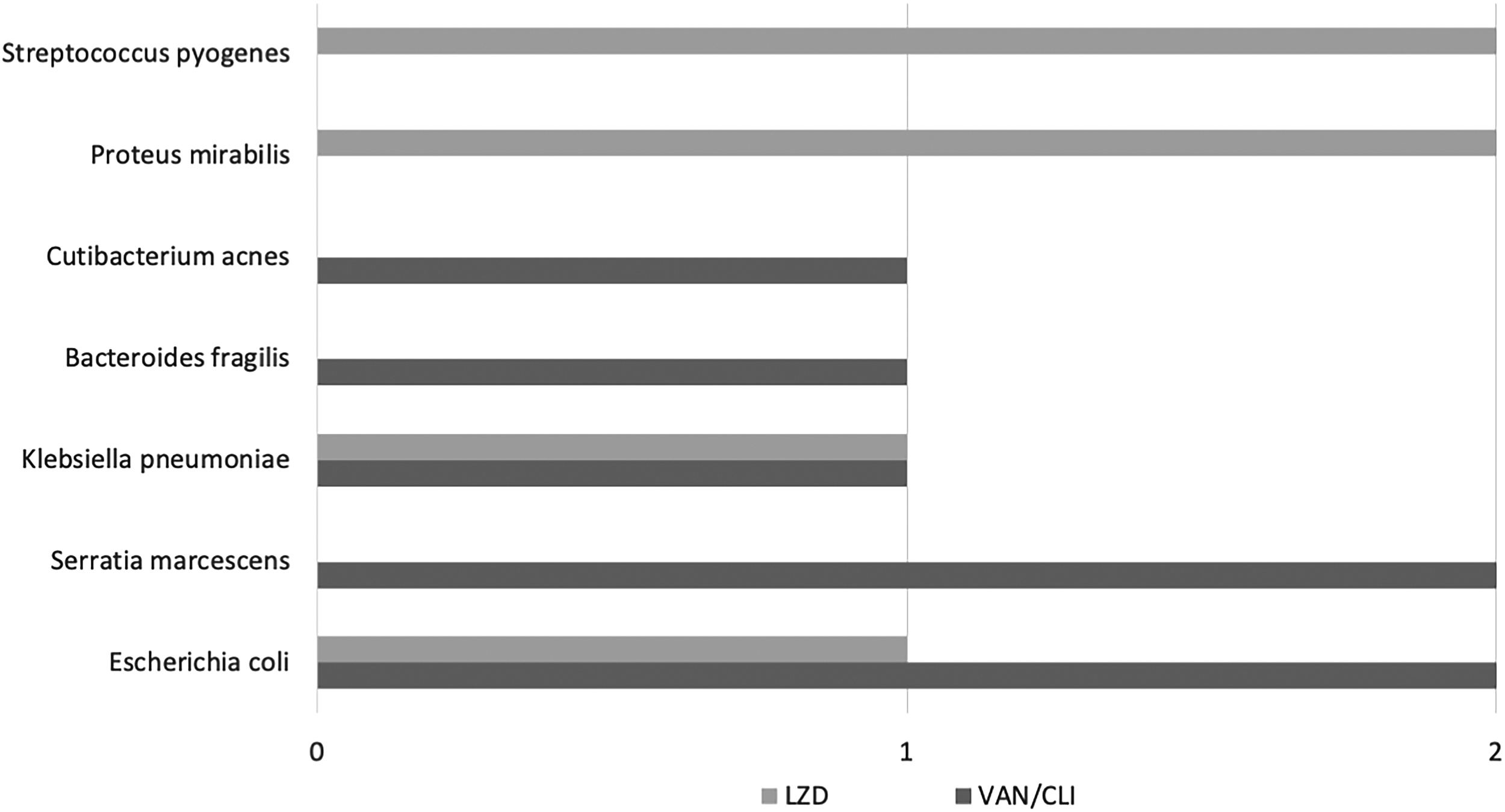
Bacterial organisms isolated in deep wound cultures.
Discussion
Empiric linezolid use for NSTI in this cohort resulted in one less day of MRSA-active therapy on average and less adverse drug events (i.e., no patients developed AKI or CDI). This shorter duration with linezolid may have been associated with the order's automatic stop time (at 72 hours of therapy), however, institutional standard practices include daily evaluation of antimicrobial need and allow for a request for extension of therapy if required. The impact of extending antibiotic use by one day is clinically significant as this extension has been shown to increase the risk of adverse drug events and pathogen resistance [12]. There is a lack of robust literature on use of linezolid in empiric NSTI regimens [5,15]. This paucity of data may be related to variability in selection of empiric antibiotic agents and antibiotic duration, with a recent multi-center review supporting the fact that there is no standardized practice for NSTI patients [15]. In the Surgical Infection Society's 2020 Guidelines on the Management of Complicated Skin and Soft Tissue Infections, the lack of large-scale trials to inform empiric antimicrobial selection for NSTI is discussed and the authors recommend coverage for suspected pathogens based on patient presentation, host, and exposure [5].
Acute kidney injury as a secondary outcome appeared different between the cohorts. This outcome was of particular interest as concomitant vancomycin and piperacillin-tazobactam are frequently utilized in this patient population. When vancomycin is used in combination with piperacillin-tazobactam, an additive nephrotoxic effect may occur and therefore might influence the incidence of drug-induced AKI [11,12]. One study evaluated the impact of renal stress after administration of the combination of vancomycin with piperacillin-tazobactam. In this study, subjects were found to have a greater release of AKI biomarkers, and this may be associated with long-term adverse outcomes [12]. Of the eight subjects in the vancomycin/clindamycin cohort with a diagnosis of AKI, two subjects were found to have potential drug-induced AKI based on KDIGO guideline criteria, defined as occurring 72 hours after initiation of therapy [13]. These patients also had documentation from nephrology consult regarding potential drug-induced AKI. In current NSTI literature and guidelines, empiric antibiotic therapy includes piperacillin-tazobactam, vancomycin, and clindamycin. Therefore, it is especially crucial to monitor patients with baseline renal dysfunction or those at high risk for development of AKI when being initiated on this empiric regimen, however, alternative antibiotic regimens may avoid this complication altogether [5,9,10].
The use of antibiotic agents in general may be associated with CDI, however, clindamycin has been associated with a higher risk [14]. This study demonstrated both avoidance of one additional day of MRSA-active therapy and avoidance of CDI in the linezolid cohort. Fifteen total subjects received testing with Clostridioides difficile toxin PCR for CDI, and two subjects were found to have positive tests from the vancomycin/clindamycin cohort. The significance of this outcome is also limited as the definition only included a single hospital encounter and did not take into account the subjects’ history of CDI, other outside hospital encounters or recent antibiotic use.
Limitations for this project include its small sample size at a single center. Furthermore, the retrospective nature of the analysis limited the ability to control for baseline characteristics. Although not statistically significant, longer durations of vasopressor and ventilator use in the vancomycin/clindamycin cohort might have impacted secondary endpoints such as AKI and hospital and ICU length of stay. The primary outcome, duration of MRSA-active therapy, might also be affected by a delay to surgical source control as the time to definitive procedure was not evaluated in this cohort. This analysis also limited conclusions regarding secondary outcomes including a lack of the etiology of AKI and symptom evaluation of CDI. Potential adverse effects of vancomycin (i.e., AKI) and clindamycin (i.e., CDI) were evaluated in this study but potential adverse effects of linezolid (i.e., thrombocytopenia) were not evaluated fully [11,12,14]. However, the average duration of linezolid therapy in this study was three days and onset of thrombocytopenia is more likely to occur with longer durations of treatment (i.e., 7 to 14 days) [16].
Last, no MRSA was isolated in this cohort, limiting the conclusions of this study to empiric coverage only. The subjects evaluated may not have been at risk for MRSA based on their exposure and local rates of community-acquired and hospital-acquired MRSA were not accounted for in this study. Methicillin-resistant Staphylococcus aureus coverage in general may be better determined by patient and environmental risk factors including pre-surgical swabs, however, because linezolid provides antitoxin effects, its use may not be affected by this approach.
As far as strengths are concerned, this observational cohort analysis is the only study to date evaluating empiric antibiotic regimens for the treatment of NSTI. Although our cohort is limited, small sample sizes generally lead to false-negatives versus false-positives, so the differences in antibiotic days and AKI are valid findings. These study results may be limited by the small sample size and retrospective design but represent real-world experience with an antibiotic regimen that may avoid potential for several adverse drug events. Further practical considerations include the avoidance of monitoring serum concentrations and using one agent versus two. Although exact costs were not calculated for each patient in this study, on average an estimation of the total drug and monitoring costs of the anti-MRSA agents in the vancomycin/clindamycin cohort and in the linezolid cohort were similar.
Conclusions
Linezolid was a safe and effective alternative for empiric NSTI treatment compared with the combination of vancomycin and clindamycin. The average duration of MRSA-active therapy was one day less with empiric linezolid. The impact of decreasing antibiotic use by one day can potentially reduce the incidence of adverse events and/or pathogen resistance. Additionally, the rate of new-onset AKI during hospitalization was lower in the linezolid cohort. Larger randomized, prospective studies evaluating empiric NSTI treatment regimens are needed to support the findings in this study.
Footnotes
Acknowledgments
The authors of this study would like to acknowledge Benjamin Staley, PharmD, BCPS Clinical Data Translation Specialist for assistance with accessing subject information; Kathryn DeSear, PharmD, BCIDP, FIDSA Infectious Diseases Clinical Pharmacy Specialist for the creation and modification of the data set; and Luke Manda, UF College of Pharmacy PharmD Candidate 2023 for assistance with data collection.
Funding Information
There is no funding to report for this study.
Author Disclosure Statement
No authors have any disclosures to report for this study.