
Abstract
Background:
Early detection and treatment of a colorectal anastomotic leak reduces leak-associated morbidity. The primary objective of this study was to assess the role of C-reactive protein (CRP) as a tool to facilitate the early diagnosis of large bowel anastomotic leak.
Patients and Methods:
We conducted a prospective observational study at a specialized colorectal unit of a tertiary referral teaching center where we recorded CRP levels pre-operatively and on day three for 113 patients undergoing a large bowel anastomosis. The primary outcome measure was the occurrence of anastomotic leak and its association with post-operative day three CRP levels (day one considered as 24 hours after surgery). The area under the curve of the receiver operating characteristic (ROC) curve analysis for the day three CRP value with the anastomotic leak was calculated and optimal cutoffs derived. Definitions and diagnostic criteria for a leak were established before commencing the study. Demographic, operative, diagnostic, and interventional procedure data were also recorded.
Results:
Twenty-two patients had an anastomotic leak (19.4%), and 14 (12.3%) required re-exploration or drain placement. The cutoff value of day three CRP with the greatest area under the ROC curve in the ROC curve analysis was 166 mg/L (area under the curve [AUC], 0.853) for open and laparoscopic procedures (sensitivity and specificity of 81.81% and 82.42%, respectively) with a negative predictive value of 93.8%. There was no difference in mean day three CRP levels between open and laparoscopic surgery (116.57 mg/L vs. 108.94 mg/L)
Conclusions:
A CRP value of more than 166 mg/L on day three should raise suspicion of an anastomotic leak.
Anastomotic complications after colorectal operations lead to substantial morbidity and mortality. They prolong recovery, cause delays in further treatment, and add to health care costs.1,2 When anastomotic complications occur, early detection and treatment may reduce morbidity and mortality. 3 Early detection may help avoid a laparotomy, stoma, or other complications. 4 Anastomotic leaks are typically suspected based on clinical features such as fever, tachycardia, and abdominal signs of peritonitis. Laboratory tests such as increased white blood cell count or computed tomography (CT) imaging are used to confirm the clinical suspicion. However, these clinical features often manifest only by the eighth post-operative day.
Post-operative C-reactive protein (CRP) levels have shown promise in the early detection of anastomotic leaks. After major surgery, CRP levels increase and peak on the second post-operative day and subsequently decline in the absence of an infective complication. In patients with anastomotic complications, CRP values remain elevated.5–7 This difference in CRP values between these two groups becomes detectable as early as the third post-operative day after surgery. An elevated day three CRP level can thus be used as an early marker for detecting an anastomotic complication.
A meta-analysis of seven studies including 2,483 patients concluded that a single CRP value on post-operative days three, four, or five could be used to differentiate patients with or without anastomotic complications. They reported a single day three value of 172 mg/L having a negative predictive value above 95%. 8 This meta-analysis included retrospective studies, and CRP values were not performed on all patients but only selectively. The studies also varied on the day of the CRP sampling. However, published data quote a wide range of day three CRP values ranging from 101 to 143 mg/L, and many retrospective studies did not measure CRP consistently on day three, with the possibility of selection bias. Multiple studies have measured CRP at varying time points.7–10
In this prospective cohort study, we aimed to assess the usefulness of a single post-operative day three CRP value in ruling out anastomotic complications among patients undergoing colorectal anastomosis. Our secondary objective was to calculate the optimum day three cutoff value to rule out anastomotic complications.
Patients and Methods
Study design and setting
This prospective observational study was conducted in the colorectal surgery unit of a tertiary care teaching institute. The study was approved by the Institutional Review Board (IRB No. 9759) and funded through an internal research grant.
Participants
All consenting adult patients undergoing an elective colonic or rectal anastomosis between January 2016 and June 2017 were considered for inclusion. Patients with any active infection or active systemic inflammatory disease (including inflammatory bowel disease and connective tissue disorders) were excluded. Patients who required re-exploration before day three were also excluded.
Study protocol
We measured CRP levels for all eligible patients pre-operatively and post-operatively on day three; we defined the day of surgery as day zero. C-reactive protein samples were collected via a peripheral venipuncture in a BD Vacutainer® Plus tube, Red Hemogard cover® (BD Inc., Franklin Lakes, NJ) and were quantified by nephelometry (Siemens ProSpec System, Siemens AG, Munich, Germany). Post-operative management was as per unit protocol. Although the treating surgical team was not blinded to the CRP results, the CRP values were not used as a basis for further evaluation. Existing unit and hospital policy on detection and management of anastomotic leaks was followed. All patients were followed up for 30 days post-operatively.
Outcomes
The primary outcome measure of interest was anastomotic complications. For this study, we used a broad criterion for anastomotic complications, and any one of the following was considered to be indicative of an anastomotic complication: luminal or feculent contents in the drain or from the surgical site; radiologic evidence of anastomotic leak, the presence of air or fluid collection along with air in the anastomotic region or intra-abdominal/pelvic collection with air pockets or contrast extravasation from the anastomotic site; or evidence of anastomotic dehiscence on re-exploration.11–13
Data collection and statistical analysis
Data including CRP values, demographics, operative details (anastomosis technique, stapled or hand-sewn, level of anastomosis), diagnostic tests, and interventions were recorded onto an EpiData Manager form via the EpiData entry client (The EpiData Association, Odense M, Denmark) and analyzed with SPSS software (SPSS, IBM Corp, Armonk, NY). Clinical continuous variables were represented as mean and standard deviation, and categorical variables as frequencies and percentages. Associations between independent continuous covariates and leak occurrence were assessed using the Mann-Whitney U test. Categorical variables were studied using the χ2 or Fisher exact test. Univariable and multivariable analyses were performed to identify risk factors for an anastomotic leak. Receiver operating characteristic curve analysis was used to determine the optimum cutoff value corresponding to the maximum AUC for day three CRP.
Results
The total number of patients recruited was 120; 13 patients were eligible after applying the exclusion criteria. Seven were excluded (Fig. 1).

Algorithm of study flow.
The mean age of participants was 51.2 years and 70 (61.9%) of 113 patients were male. The most common indication for surgery was malignancy in 92 patients (81.4.%).
The most common operations were anterior resection in 33 patients (29.2%) and right hemicolectomy in 30 patients (26.5%). Thirty-three patients (29.2%) underwent a laparoscopic procedure. Details of patient demographics are provided in Table 1.
Baseline Patient Characteristics
Anastomotic complications
Twenty-two patients (19.4%) had an anastomotic complication. Four were diagnosed clinically, 14 were detected with a CT scan, and four during re-laparotomy. Eight patients were managed non-operatively, two patients required radiologic procedures, and 12 required re-laparotomy. Table 2 contains the post-operative details of patients with an anastomotic leak. Leaks were detected on average on day eight (Fig. 2).
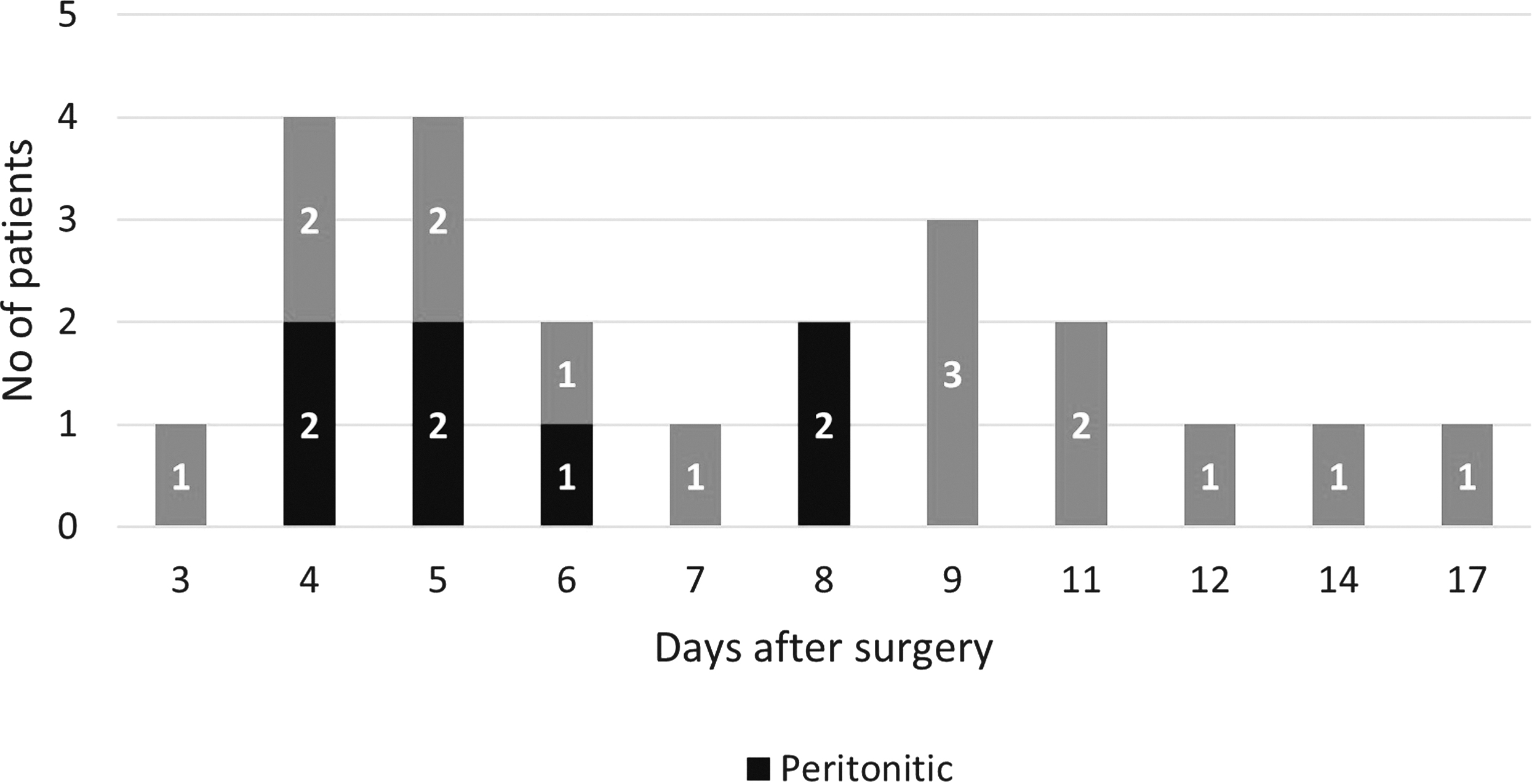
Leak detection, days after surgery.
Post-Operative Outcomes
C-reactive protein and anastomotic complications
The mean CRP of the whole population was 114 mg/L. The mean CRP among patients with an anastomotic leak was 186.4 mg/L, and among those without a leak was 96.9 mg/L. There was no significant difference in CRP values between laparoscopic and open procedures.
Underlying disease, pre-operative CRP value, age, gender, surgical approach, surgical procedure, level of anastomosis, stapled versus hand-sewn, curative versus palliative intent were not associated with the occurrence of a leak. Day three CRP was shown to be a predictor of anastomotic complications.
Day three CRP and leak
A CRP cutoff of 166 mg/L yielded 81.8% sensitivity and 82.4% specificity (AUC, 0.853) for anastomotic compilations. The negative predictive value at this cutoff was 93.8%. Using this cutoff, 2.5% of patients in the low CRP group had anastomotic complications, and 55.5% of patients in the high CRP group had anastomotic complications.
The mean day of leak detection was day eight, however, most leaks were detected on day four or five, and another peak noted around day eight to nine (Fig. 2).
Leaks detected between days three and eight: Clinical course
Of 22 patients with a leak, 14 patients were detected between days three and eight. The most common symptom was abdominal pain, vomiting, and distension after oral feeding.
Patients who developed peritonitis or enteric contents noted in the surgical site or drain were directly posted for an exploratory laparotomy (7/14 patients; see Fig. 2, marked in red). The remaining seven patients with clinical suspicion of a leak were kept nothing by mouth, nasogastric tube placed for decompression, and started on antibiotic agents if there were any signs of systemic inflammatory response syndrome (SIRS). They all underwent an abdominal contrast CT scan on or before day five which confirmed a leak. Four were successfully managed conservatively, whereas three patients failed conservative measures and required surgery within 48 hours of leak detection. (one patient on days five, six, and seven).
Between days three and eight, there were three patients who were discharged before a leak was detected. They later presented to the emergency department with peritonitis or feculent content in the midline incision (one patient on day five and two patients on day eight).
Leaks detected after day eight: Clinical course
There were eight patients with leaks detected between day nine and day 17. In this group, five of these eight patients did not tolerate an oral diet well, however, their symptoms were milder and were therefore managed conservatively.
Detection of a leak was delayed in this subset; the CT abdomen that eventually detected the leak was ordered only when the patient developed midline wound discharge (four of eight), failed to respond to conservative measures (two of eight), or in the case of two patients only when they presented for outpatient review after discharge with diarrhea and low-grade fever (day 11 and day 17).
Elevated day three CRP and non-anastomotic complications
Sixteen patients with a day three CRP greater than 166 mg/L did not have an anastomotic leak. The mean day three CRP in this group was 192.7 mg/L. Thirteen of these patients had significant non-anastomotic complications (Table 3).
Elevated Day Three CRP >166 mg/L and Non-Anastomotic Complications
SSI = surgical site infection.
Discussion
In this study, we have shown that a CRP on day three is different between patients with and without a leak, and a cutoff value of 166 mg/L can be used with an 81.8 % sensitivity and 82.4% specificity. This is in keeping with the literature in which CRP levels are continually elevated in patients with anastomotic complications.5–8 The mean day of leak detection in our study was on day eight. Ortega-Deballon et al., 5 Almeida et al., 6 and Garcia-Granero et al. 7 have shown similar trends, with clinical findings and elevated white cell counts detecting leaks at day seven.
In our study, those with overt signs of peritonitis or SIRS were correctly suspected to have a leak and were diagnosed appropriately, often within the first five days. However, patients who had milder symptoms had delayed detection, usually after the eighth day. In fact, five patients were discharged prematurely because they appeared clinically well, only to return later with overt symptoms of an anastomotic leak. These relatively asymptomatic patients were not identified early enough, despite being reviewed in multiple ward rounds by an experienced clinical team. The advantage of day three CRP testing is the early detection of those patients who initially manifest with only minimal clinical findings. An elevated day three CRP should prompt heightened vigilance and consideration of early CT imaging.
An elevated day three CRP value after colorectal anastomosis indicates an ongoing inflammatory process, most importantly, an anastomotic leak. An elevated value should prompt heightened vigilance and consideration of early cross-sectional imaging to confirm or rule out a leak. In patients with equivocal findings, or in patients in whom a decision is made to manage a small leak non-operatively, the subsequent trajectory of CRP values can help gauge response to treatment or plan for discharge. A single assay on day three, with selected patients undergoing serial CRP assays is also cost effective, especially when patients pay out-of-pocket for healthcare. McSorley et al. 14 advocate a “CRP first approach” as a valuable tool to reduce morbidity of late detection of anastomotic complications, and the ongoing PRECious trial also seeks to evaluate this strategy. 15
We found the ideal day three CRP cutoff value with maximum AUC 85.3% (95% confidence interval [CI], 76.8%–91.6%) (AUC) at 166 mg/L (sensitivity and specificity of 81.81% and 82.42%, respectively; Fig. 3). Choosing a high cutoff would have a high specificity at the cost of lower sensitivity, meaning higher false negatives. A false negative in this scenario is a missed leak, which defeats the purpose of earlier detection.
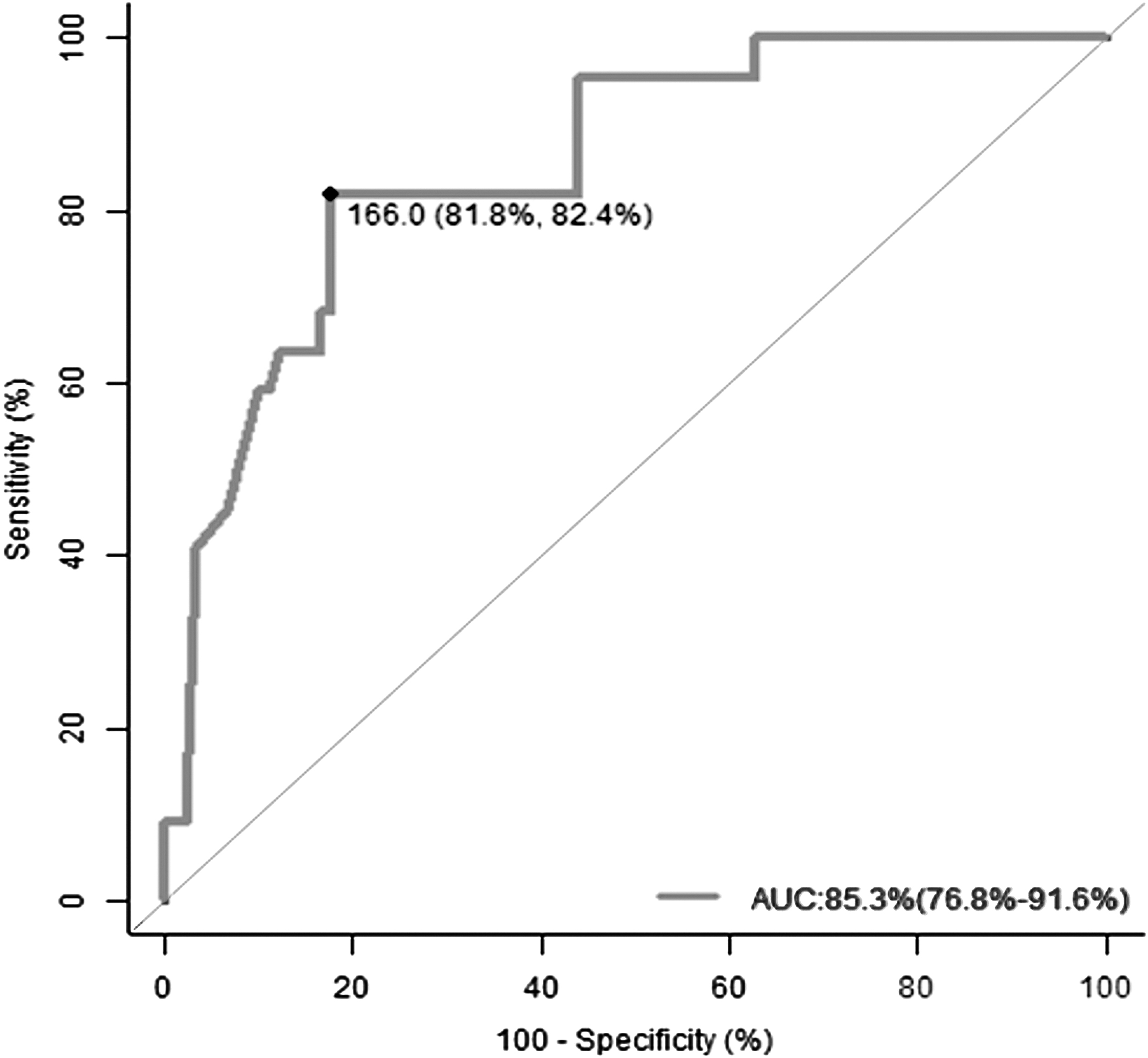
Receiver operator characteristic curve for day three C-reactive protein (CRP) values in detecting an anastomotic leak. AUC = area under the curve.
We derived a negative predictive value of 93.8% at this cutoff value of 166 mg/L. In a similar study, Garcia-Granero et al. 7 derived a cutoff value on day three of 147 mg/L with an negative predictive value of 99%. In a meta-analysis of 2,483 patients, Singh et al. 8 also derived a day three cutoff of 172 mg/L. Although we have shown a day three value to be significant, Singh et al. 8 found that CRP measured on days four and five was also valuable
Even in the absence of an anastomotic leak, an elevated day three CRP level may indicate the presence of substantial non-anastomotic complications. Enhanced recovery after surgery (ERAS) protocols dictate shorter hospital stays; a CRP level less than 166 mg/L on day three also serves as an excellent predictor of an uneventful post-operative outcome. Although many studies measured CRP daily in the post-operative period, a single CRP assessment on day three may be sufficient to facilitate early detection and serve as a marker for safe discharge.5–7,16–18
Our study has many limitations. The treating team was not blinded to the CRP levels, which could have introduced some bias in the management protocol. Although some studies have shown differential CRP levels in open and laparoscopic groups, we did not perform subgroup analysis for this. This is because of the differential distribution of complications in the laparoscopic and open arm and small numbers in the laparoscopic arm. Other markers such as procalcitonin and interleukin 6 are useful, either in isolation or combined with other markers for early detection.19 We have not explored this in this study. The day three CRP value with our derived AUC of 85.3% cannot be used in isolation to detect leaks, and certainly does not supplant clinical judgment, however, it is a useful adjunct in decision-making, especially in patients with subtle signs.
Our results need to be validated in a prospective cohort. It is hoped that early investigations and intervention in those with high CRP will lead to early detection and therefore reduced morbidity and mortality. The effect of CRP-directed imaging and leak detection needs further study.
Conclusions
The post-operative day three CRP is different between patients with and without an anastomotic leak. A CRP value of 166 mg/L has a sensitivity of 81.8% and a specificity of 82.4% with an negative predictive value of 93.8 and can be used as one of the markers for safe discharge.
Footnotes
Funding Information
This study was funded through a fluid research grant from the research wing of Christian Medical College, Vellore, India, which is dedicated to post-graduate research.
Author Disclosure Statement
There was no direct or indirect funding or support from any pharmacological company or instrumentation labarotory or provider of equipment. There was no conflict of interest declared by any of the authors.