
Abstract
Background:
Splenic abscess (SA) is a rare, life-threatening illness that is generally treated with splenectomy. However, this is associated with high mortality and morbidity. Recently, percutaneous drainage (PD) has emerged as an alternative therapy in select patients. In this study, we compare mortality and complications in patients with SA treated with splenectomy versus PD.
Patients and Methods:
A systematic literature search of 13 databases and online search engines was conducted from 2019 to 2020. A bivariate generalized linear mixed model (BGLMM) was used to conduct a separate meta-analysis for both mortality and complications. We used the risk of bias in non-randomized studies of interventions (ROBINS-I) tool to evaluate risk of bias in non-randomized studies, and the Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) approach for assessing quality of evidence and strength of recommendations. Results were presented according to Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.
Results:
The review included 46 retrospective studies from 21 countries. For mortality rate, 27 studies compared splenectomy and PD whereas 10 used PD only and nine used splenectomy only. Data for major complications were available in 18 two-arm studies, seven single-arm studies with PD, and seven single-arm studies with splenectomy. Of a total of 589 patients, 288 were treated with splenectomy and 301 underwent PD. Mortality rate was 12% (95% confidence interval [CI], 8%–17%) in patients undergoing splenectomy compared with 8% (95% CI, 4%–13%) with PD. Complication rates were 26% (95% CI, 16%–37%) in the splenectomy group compared with 10% (95% CI, 4%–17%) in the PD group.
Conclusions:
Percutaneous drainage s associated with a trend toward lower complications and mortality rates compared with splenectomy in the treatment of SA, however, these findings were not statistically significant. Because of the heterogeneity of the data, further prospective studies are needed to draw definitive conclusions.
Splenic abscess (SA) is a rare and often fatal condition that commonly presents with fever, left upper quadrant abdominal pain, and leukocytosis [1,2]. Evidence from autopsy series in western countries suggests SA has an incidence rate between 0.14% and 0.7% [3–5]. Although SA is rare in high-income countries, case reports suggest a higher incidence of SA in low-income countries [6–8]. The incidence of SA has increased in recent years, which has been attributed to numerous factors including increased detection from improved imaging technology, increasing intravenous drug use, and higher rates of immunocompromise [4,5].
Treatment for SA has traditionally included splenectomy with antibiotic agents [4–7]. Splenectomy is associated with morbidity and mortality due in part to increased susceptibility to overwhelming infection from encapsulated organisms [1,5,7,9,10]. Spleen-preserving treatments using imaging-guided percutaneous drainage (PD) have been recognized as effective treatment options for SA [5]. Percutaneous drainage is particularly effective for patients who are poor candidates for surgery [5]. In addition to preserving the spleen, some studies have demonstrated reduced risks of intra-abdominal spillage, low peri-operative complications, and shorter recovery time in patients who undergo PD instead of splenectomy [1,5,8,11,12].
Mortality associated with splenic abscess is high and varies by immune status, underlying etiology, type of abscess, and speed of diagnosis [5]. Splenic abscessed that are untreated or inadequately treated are often fatal [11,13]. Currently, there is no consensus or guideline for SA management. Our study aims to determine whether image-guided percutaneous drainage of SA compared with splenectomy is associated with decreased mortality and morbidity.
Patients and Methods
Literature search strategies
This study was registered with PROSPERO, the international prospective register of systematic reviews (registration: CRD42020164221). A comprehensive search strategy was created using controlled vocabulary and free-text terms, in accordance with the Methodological Expectations of Cochrane Intervention Reviews (MECIR) standards. The searches were created and executed between December 11, 2019 and February 6, 2020 by a trained medical librarian (D.H.) in 13 databases and online search engines: Medline via Ovid (1946 to December 13, 2019) and PubMed (1946 to present); Embase via Ovid (1947 to December 20, 2019); Cochrane Library via Wiley (1996 to present), Web of Science Core Collection (1900 to present); ClinicalTrials.gov, the World Health Organization's (WHO) International Clinical Trials Registry Platform and Global Index Medicus; the ISRCTN Registry; African Journals OnLine; the NIH RePORTER; National Information Center on Health Services Research (NICHSR) ONESearch; and Google Scholar. Studies were limited to human studies published after 1990 because of changes in available surgical technology. The complete search strategy is included in Supplementary Table S1. Articles were compiled and de-duplicated in Mendeley and all screening was performed in Covidence [14].
Inclusion and exclusion criteria
No filters were used to exclude particular study types or languages from our database searches. We included studies with patients with SA treated with either splenectomy or PD. For splenectomy, we considered patients undergoing splenectomy using either open or laparoscopic approaches. For PD, we included patients undergoing image-guided PD using either computed tomography (CT) or ultrasound (US)-guidance based. Patients were included if the PD was performed using either aspiration or drain placement for treatment purposes. Patients were not included if they underwent a procedure for diagnostic, but not therapeutic, drainage. We included only those studies reporting data on the primary outcome, mortality.
Our exclusion criteria included: duplicate publication, full-text unavailable, inability to extract key data including data on the primary outcome (mortality), studies with fewer than five participants, studies limited to animals, and studies published prior to 1990. The search strategy was limited to publications after 1990 because PD is a newer technology. In addition, there have been advances in management of patients with sepsis and critically ill patients over time that could also influence outcomes. Patients undergoing percutaneous techniques for diagnosis, rather than treatment, were excluded.
Screening and data collection
Two reviewers (B.G., J.W.) independently screened articles for eligibility and a third reviewer (J.R.) resolved any differences. Studies were screened for eligibility using title and abstract. Then, studies underwent a full text review. The results of the screening and selection steps are illustrated using the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram (Fig. 1).

Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram detailing the study screening and selection process.
Data were extracted independently by two reviewers (B.G., J.W.). A third reviewer (J.R.) resolved any discrepancies. Data were stored and compared in Redcap [15]. We performed a pre-test before the formal extraction to ensure accurate data collection. Our data collection forms were based on templates created by the Cochrane Developmental, Psychosocial, and Learning Problems group [16]. Google translator was used to translate studies that were not written in English.
We collected data on age, gender, comorbidities and contributing factors, abscess characteristics, treatment received, and outcomes such as comorbidities and mortality. We defined comorbidities as any reported co-existing disease process such as hypertension or coronary artery disease. Contributing factors were defined as any potential inciting or exacerbating event or disease process such as endocarditis, surgery, or trauma. Some conditions, such as diabetes mellitus or human immunodeficiency virus, could be considered as both a comorbidity and contributing factor. Because there were differences in reporting of these factors, we reported both comorbidities and contributing factors together. Abscess characteristics were inconsistently recorded, therefore we limited our data collection to single versus multiple because this was the most commonly reported abscess characteristic.
Our primary study outcome was mortality. We included in-hospital and 30-day mortality. The secondary outcome was any post-operative complication. Because there was no standard definition for complications found in the studies, we included all reported post-operative complications. We also examined the number of patients receiving PD who later required repeat drainage or salvage splenectomy. We conducted two separate analyses when evaluating complications. Our first analysis of complications included only those reported post-operative complications. Our second analysis of complications included reported post-operative complications as well as repeat drainage and salvage splenectomy as complications.
Risk of bias and quality of evidence assessment
We used the risk of bias in non-randomized studies of interventions (ROBINS-I) tool to evaluate risk of bias in non-randomized studies, and the Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) approach for assessing quality of evidence and strength of recommendations (Supplementary Table S2A and S2B) [17,18].
Statistical analysis
For the two-arm studies that had both intervention groups, we used a standard random-effects meta-analysis to compare outcomes between the two groups. We focused on the mortality and complication rates. The risk difference (RD) was used as the effect measure. We used the command rma from R package “metafor” to implement this standard random-effects meta-analysis using the recommended restricted maximum likelihood (REML) method [19]. This approach uses an artificial continuity correction of adding 0.5 to each cell of studies where either intervention has no event in the two-arm studies, which were 20 of 27 studies. This standard approach excludes single-arm studies with either splenectomy only or PD only.
Alternatively, a bivariate generalized linear mixed model (BGLMM) was used to estimate the overall RD, which uses the exact binomial likelihood and accounts for single-arm studies and zero events in two-arm studies [20]. Through this BGLMM model, random effects were used to represent between-study heterogeneity of the outcome rates among studies. The BGLMM also estimated the overall outcome rates for each treatment, and obtained the overall RD. Via this approach, studies with only one treatment available or zero events, can still contribute to the estimation without continuity correction. We also calculated the corresponding 95% confidence intervals for those overall estimates. We used PROC NLMIXED in SAS (version 9.4; SAS Institute Inc, Cary, NC) to implement the BGLMM.
The meta-analysis results and the comparison between the standard random-effects model and BGLMM were represented in forest plots. Between-study heterogeneity was assessed by the Cochran Q test and the I2 statistics [21,22]. The I2 statistic was used to describe the percentage of the variation across studies that is caused by between-study differences rather than chance. Common cutoff points for low (I2 = 25%), moderate (I2 = 50%), and high degrees of heterogeneity (I2 = 75% or higher) were used. We visualized the differences between splenectomy and PD among all studies using caterpillar plots. Because most studies have one arm with zero event, we did not conduct any publication bias test [23]. The statistical significance level was set at 0.05. Data were reported according to guidelines provided by PRISMA for systemic reviews and meta-analyses [24].
Results
Study characteristics
A total of 6,845 studies were identified through the initial literature research. After screening for eligible studies, 46 studies were included in the meta-analysis (Fig. 1). Table 1 details basic characteristics of the included studies. Twenty-seven of the 46 studies included both interventions: splenectomy and image-guided PD (two-arm studies) [3,4,11,25–47]. Nine studies included splenectomy only [48–56] and 10 studies included PD only [5,57–65].
Characteristics of Studies Examining Complications and Mortality in Patients Receiving Splenectomy versus PD for SA
WBI = World Bank Income Level (H = high, UM = upper middle, LM = lower middle, L = low); BiH = Bosnia and Herzegovina; , USA = United States of America; ROB = risk of benefit assessment (H = high); NR = not reported; PD = percutaneous drainage; SA = splenic abscess; N/A = not applicable; NR = not reported.
Google Translate utilized.
All studies had data on mortality, whereas only 30 studies had data on complications. Only 14 of the 27 two-arm studies had the number of patients with complications available in both intervention arms. Two two-arm studies had complications data for one study arm. For the single-arm studies, complications were recorded in seven of nine splenectomy-only and seven of 10 PD-only studies.
Using World Bank Income Level, of the 46 studies, six were from upper-middle income countries, 10 were from lower-middle income countries, and 30 were from high-income countries. All studies were retrospective chart reviews or case series and had a high risk of bias.
Patient characteristics
Table 2 summarizes patient and abscess characteristics from the included studies. In these 46 studies, there were 979 patients of whom 531 were male, 314 were female, and the gender was not reported for the remaining 134 subjects. The mean study age ranged from eight to 74.1 years old. Data on comorbidities and contributing factors were available in 45 studies. The most reported comorbidities were diabetes mellitus, cancer, endocarditis, and immunosuppression.
Characteristics of Patients in the Studies Included in the Meta-Analysis Comparing Splenectomy versus PD for SA
PD = percutaneous drainage; DM = diabetes mellitus; CA = cancer; LD = liver disease; PNA = pneumonia; SCD = sickle cell disease; EC = endocarditis; PA = pancreatitis; MDS = myelodysplastic syndrome; SLE = systemic lupus erythematosus; CHF = congestive heart failure; PUD = peptic ulcer disease; AIDS = acquired immune deficiency syndrome; ALL = acute lymphoblastic leukemia; ESRD = end-stage renal disease; COPD = chronic obstructive pulmonary disease; CAD = coronary artery disease; ETOH = alcohol use; HTN = hypertension; NHL = non-Hogkin lymphoma; AML = acute myeloid leukemia; MPD = myeloproliferative disorder; IVDA = intravenous drug addiction; MI = myocardial infarction; UTI = urinary tract infection; TB = tuberculosis; Tx = transplant.
Of the 979 reported patients, 813 had splenic abscess. One hundred sixty-six patients had other conditions and were not included in the analysis. Of the 813 patients with SA, 246 had multiple abscesses, 402 had single abscess, and 165 patients did not have abscess characteristics reported. Supplementary Table 3 shows the microbiologic etiology of the abscesses. In total, 288 patients underwent splenectomy, 301 underwent percutaneous drainage, 218 received antibiotic agents only, and the remaining six underwent a different treatment method (i.e., open drainage). Thus, 589 patients were included in the study to compare percutaneous drainage versus splenectomy. Most patients with splenectomy or PD had concomitant antibiotic therapy, but data for the exact number of patients and course of antibiotic agents were incomplete.
Mortality and Complications of Patients with Splenic Abscess Treated with PD or Splenectomy
PD = percutaneous drainage; N/A = not available; SCD = sickle cell disease; LD = liver disease; EC = endocarditis; CA = cancer; DM = diabetes mellitus; SCT = sickle cell trait; Chemo = chemotherapy; CML = chronic myelomonocytic leukemia; TB = tuberculosis; CAD = cardiovascular disease; MI = myocardial infarction; ETOH = alcohol use; IVDU = intravenous drug use; ESRD = end-stage renal disease; HTN = hypertension; DVT = deep vein thrombosis; ARDS = acute respiratory distress syndrome; PA = pancreatitis.
Table 3 summarizes the mortality and complications reported in the included studies. Of the 589 patients with SA who were treated with PD or splenectomy, there were 64 deaths (11%), 35 of which were patients undergoing splenectomy whereas the remaining 29 received PD. The overall mortality rate for patients receiving splenectomy was 12% compared with 10% for PD. Eighty-five (14%) patients had complications, 67 of whom underwent splenectomy whereas the remaining 18 underwent PD. Commonly reported complications included pneumonia, sepsis, and wound infection. The overall complication rate for splenectomy was 23% compared with 6% in PD. Of the patients receiving PD, 27 (9%) required salvage splenectomy and 16 (5%) required repeat drainage. When these were included in complications, the overall complication rate for PD was 20%.
Meta-analysis
Overall outcomes for each treatment per study
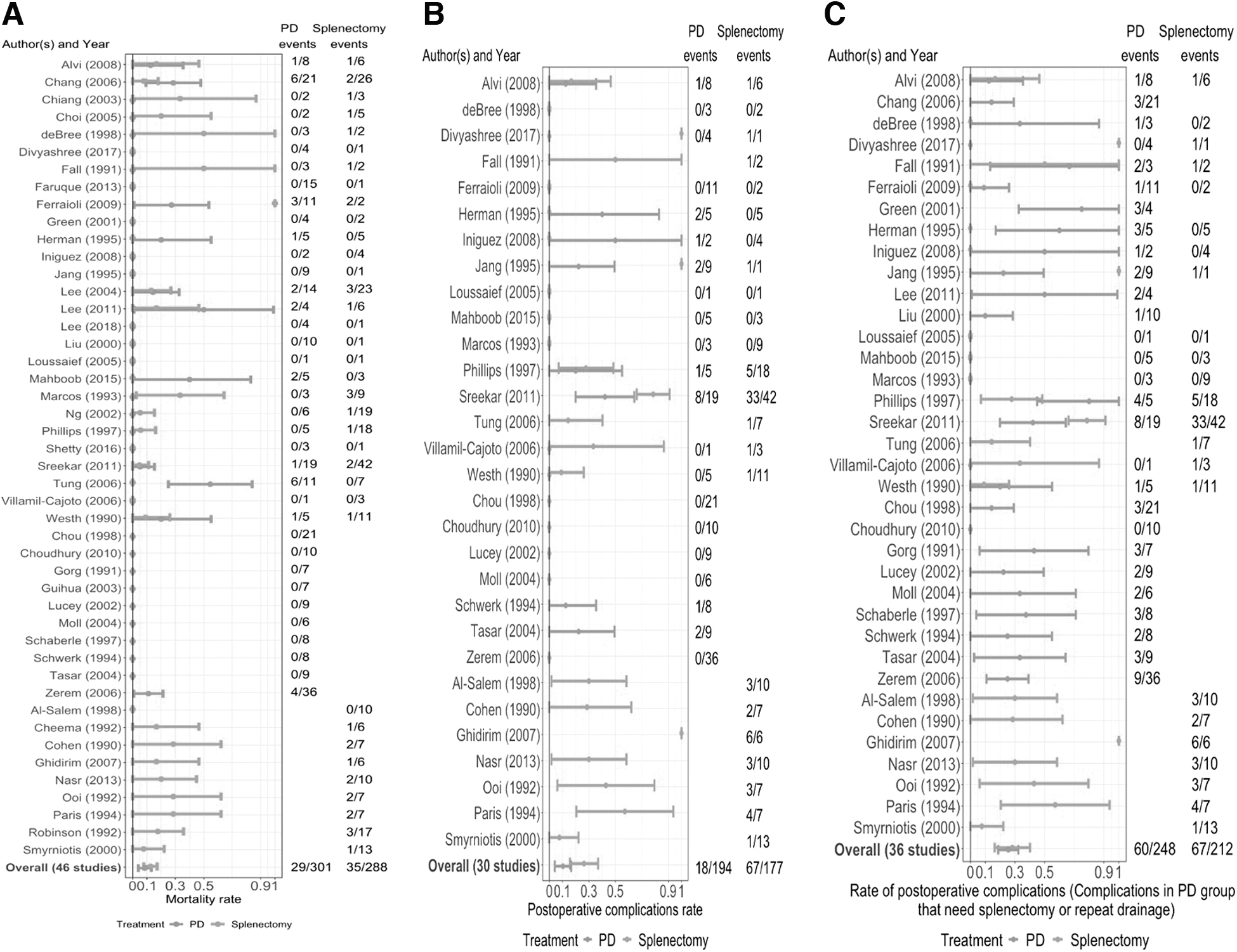
Most studies had zero mortality rate for PD-only studies compared with splenectomy-only studies (Fig. 2A). The overall risk for mortality for PD only was 8% (95% confidence interval [CI], 4%–13%) and 12% (95% CI, 8%–17%) for splenectomy only. Similarly, the overall risk of postoperative complications for PD only was 10% (95% CI, 4%–17%) and 26% (95% CI, 16%–37%) for splenectomy (Fig. 2B). The overall risk of complications when including salvage splenectomy and repeat drainage was 26% (95% CI, 19%–32%) in the PD group and 28% (95% CI, 16%–40%) (Fig. 2C) in the splenectomy group.
(
Comparing mortality rate and post-operative complication rate between the two intervention groups
The RD estimates of mortality rate and their 95% confidence intervals is depicted in Figure 3A. Using the random-effects model, the overall RD of mortality rate for PD compared with splenectomy is 2% (95% CI, −5% to 9%) from the 27 two-arm studies. In contrast, the BGLMM estimated the overall RD of −4% (95% CI, −11% to 3%) from all 46 studies.

Forest plots among 27, 14, and 15 two-arm studies (black squares) and overall meta-analysis effect estimates (polygons) from the random-effect meta-analysis in metafor package (top) and the bivariate generalized linear mixed model (BGLMM) (bottom). (
For complication rate, we had 14 two-arm studies without missing data. The overall RD of complication of PD versus splenectomy was −9% (95% CI, −22% to 5%) in the random-effects meta-analysis model from 14 two-arm studies and −16% (95% CI, −26% to −6%) in BGLMM from all 30 two-arm and single-arm studies (Fig. 3B).
Figure 3C shows that the RD of complications when including salvage splenectomy or repeat drainage between PD versus splenectomy was 2% (95% CI, −15% to 20%) in the random-effects meta-analysis, and −3% (95% CI, −15% to 10%) in BGLMM.
Discussion
Splenic abscess is a serious condition typically treated with splenectomy or PD [5]. To date, no large systematic reviews have compared the outcomes of these treatments. Our systematic review and meta-analysis did not find a statistically significant difference between mortality and complications in patients with SA treated with splenectomy versus PD. Although most of the differences between groups were not statistically significant, there was a trend toward lower mortality and complication rates associated with PD than splenectomy. We further observe that BGLMM showed stronger evidence of PD to reduce mortality and complication rates after incorporating information from studies otherwise excluded by conventional random-effects models. There are numerous factors that may explain our results.
Prior studies have highlighted the influence of a patient's pre-existing conditions and type of abscess on outcomes in SA [3,7]. Data on comorbidities and inciting factors were available in 46 of 47 studies, however, these data were often incomplete and inconsistently recorded, so we were unable to do subgroup analysis. Although some studies reported underlying factors (e.g., sickle cell disease) and inciting etiologies (e.g., trauma, endocarditis), other studies reported common comorbidities (e.g., diabetes mellitus, acquired immune deficiency syndrome [AIDS]). Each of these factors would likely impact outcomes. However, this was reported inconsistently across the studies challenging any efforts to make definitive conclusions on the effects of etiology and comorbidities on outcomes. It is possible that patients who were sicker and with more complex splenic abscess underwent splenectomy to insure control of the infection. However, it is also possible that some patients were too sick to safely undergo surgery and thus underwent PD. The heterogenous reporting of this variable makes it difficult to conclude the effect of this bias on outcomes.
Disease characteristics differed between populations as well. Abscess characteristics were not reported in 12 studies and data were not consistently available on size, whether abscesses were multilocular or unilocular, or how many abscesses were present in patients listed as having multiple. Generally, splenectomy may be performed for all abscess types including small, large, unilocular, and multilocular abscesses. In contrast, PD is best served in a select instances in which there are fewer, easily accessible, and drainable abscesses [2]. Therefore, abscess characteristics likely play a role in selection bias.
Resource availability likely also influenced outcomes, as this varied based on the time and location of the study. Splenectomy, especially using open techniques, is universally available and has been for decades. Some studies included only splenectomy patients, as that was the only treatment option available. In contrast, PD involves newer technology and may only be available in higher resource settings. The resources needed to support a PD intervention program are therefore higher than for splenectomy. Most studies (64%) included in this review were from high-income countries with no data reported from low-income countries. Of the nine splenectomy-only studies, seven began collecting data before 1990. In comparison, of the 12 PD-only studies, only two began collecting data before 1990. As medical care has advanced over time, there may be a selection bias with PD as this includes a more recent population that may have benefitted from other advances in medical care (i.e., newer antibiotic agents, advances in management of patients with sepsis, improved intensive care, etc.).
This study has several limitations. The strength of our recommendation is weakened because of the high risk of bias. All studies included in this review were case series or retrospective chart reviews, so there was limited capacity to control for confounding factors. There was a substantial amount of missing data and variations in dataset, and the small sample size limited subgroup analysis. Limited follow-up in studies may have also been a source of bias. Most studies followed patients through their hospital course, but not after hospital discharge. This may capture short-term complications but may miss other important complications such as complications associated with splenectomy or re-admissions for recurrent SA. Specifically, complications from splenectomy may take years to arise and thus are not captured by short-term data. One study examining the long-term risks of splenectomy in more than 8,000 American veterans found that risk of infection and death from infection continued to be increased more than a decade after the procedure [66]. Additionally, many of the studies with larger numbers of participants were from Asian countries, which may limit generalizability. Further investigation through multi-institutional prospective cohort studies with larger sample size and accounting for confounders (age, gender, comorbidities, etiology/inciting factor, causative pathogen, abscess characteristics, illness severity) is warranted.
Conclusions
This is the first extensive systematic review on this topic across the globe. The findings from this review will provide insight on safe ways of managing splenic abscess globally. Both splenectomy and PD are effective treatment options for SA. Although there is a trend toward reduced mortality and post-operative complications with percutaneous drainage of splenic abscess, ultimately no difference was found in outcomes of PD versus splenectomy for splenic abscess. Furthermore, the findings in this review were weakened by a high risk of bias. Providers need to account for patient, abscess, and resource characteristics in determining optimal treatment options. Further studies are needed to better delineate management when both treatment options are available.
Footnotes
Acknowledgments
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Funding Information
Research reported in this publication was partially supported by the National Center for Advancing Translational Sciences Award Number UL1-TR002494 and the National Library of Medicine Award Number R01LM012982 of the National Institutes of Health.
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.