
Abstract
Background:
Surgical site infection (SSI) is one of the most important and costly complications of surgical operations. The present study hypothesized that vitamin D deficiency is associated with an increased risk of SSI, and this current study investigated this hypothesis.
Patients and Methods:
A prospective cohort study was performed with adult patients undergoing open right hemicolectomy operation with stapled anastomosis between February 2018 and March 2021 in the surgery ward of Imam Khomeini hospital. A logistic regression test examined and analyzed the connection between serum 25-OH vitamin D levels and post-operative wound infections.
Results:
This study comprised 315 participants who met the inclusion criteria. Pre-operative serum vitamin D levels were <30 ng/mL in 107 participants (34%) and ≥30 ng/mL in 208 participants (66%). The mean serum vitamin D level was 35.66 ± 13.26 ng/mL among the study population. Increased vitamin D deficiency was linked with elevated odds of surgical wound infection incidence among the patients after surgery (odds ratio [OR], 5.49; 95% confidence interval [CI], 2.06–14.6; p = 0.001).
Conclusions:
Pre-operative vitamin D level strongly affects post-operative SSI in patients with colon cancer. This study highlighted the importance of conducting further research to determine the possible advantages of vitamin D in preventing incision infection after surgery.
Colon cancer is one of the frequent cancers among humans, with a high mortality rate. 1 The right hemicolon is home to approximately 40% of all colon malignancies. 2 Surgical resection or open right hemicolectomy is the predominant surgical approach for right-sided colon cancer. 3 Despite advancements in post-operative care, after-surgery problems in patients having elective colorectal operations have increased from 19% to 30%. 4
Nutritional status and inflammatory markers such as C-reactive protein (CRP), albumin, procalcitonin, and interleukin 6, are studied in predicting post-operative complications. 5 The occurrence and severity of post-operative complications such as surgical site infection (SSI), embolism, and deep vein thrombosis are essential factors in determining a successful surgery. 6 Pre-operative malnutrition has been proposed to be linked to an increased risk of post-operative complications such as SSI. 7 Pathophysiologically, SSI is a complicated process that includes an initial and pre-activated host immune-inflammatory reaction to pathogens, predisposition by genetic variables, and tailoring the invading microorganisms' site, load, and pathogenicity in surgical patients. 8 An SSI activates the body's immunologic system, resulting in swelling and pain, tissue damage, and slowed recovery. 9
Surgical site infection is difficult to define, and no clear rules distinguish it from contamination and colonization. 10 The incidence of SSI is an essential indicator of surgical results. The risk of wound infection development is higher in emergency operations and operations lasting longer than one hour. 11 Accordingly, the average time for open colorectal surgeries is between 95 and 135 minutes. 12 Pre-operative malnutrition and post-operative SSI are strictly interrelated. 13 Although there is a paucity in the literature concerning this fact, a few studies have paid special attention to the antimicrobial effects of vitamin D.14,15 Vitamin D sufficiency has been reported to help with healing, immunologic modulation, cellular proliferation, intestinal mucus integrity, and diabetic ulcers in laboratory settings and animal models. 16
Many studies displayed the connection of vitamin D deficiency with various cancers, being alive after surgery, and other issues.17,18 Also, vitamin C and zinc effects on wound healing have been confirmed,19,20 but there is still a gap in determining the impact of vitamin D on post-operative wound infection. Therefore, we hypothesized that vitamin D deficiency is associated with an increased risk of SSI, and this current study investigated this hypothesis.
Patients and Methods
This prospective cohort study was approved by the Ethics Committee of Urmia University of Medical Sciences with code IR-UMSU.REC.1398.297. This study was conducted in the surgery ward of Imam Khomeini hospital between February 2018 and March 2021. Written informed consent was obtained from all participants.
The principal investigator anonymized patient data after agreeing to join the study. Non-anonymized data were not available to collaborators or statisticians. Of 565 participants who underwent linear stapled open right hemicolectomy, 315 patients were selected who met the inclusion criteria. Because of the higher frequency of right hemicolectomy surgery among surgeries, we chose this anatomic localization for studying. The inclusion criteria included: histopathologic document of colon cancer; participants aged over 18 years; and patients who received therapeutic operation. The exclusion criteria were as follows: patients with diabetes mellitus; participants who underwent an emergent operation; having a smoking history; body mass index >30 and <18; malnutrition; operation time more than three hours, (7) high-grade American Society of Anesthesiologists (ASA) score (≥ grade 2); high intra-operative breeding volume >120 mL; pre-operative blood transfusion; patients with metastatic diseases; currently undergoing treatment with immunosuppressive agents; having had chemotherapy or radiotherapy in the past; patients with anastomotic leakage; patients being cared for in a nursing home; and admitted patients with confirmed asteatosis.
The routine pre-operative evaluations including blood specimens, liver and kidney function tests, and pre-operative serum levels of 25-OH vitamin D were conducted. Malnutrition refers to deficiencies, excesses, or imbalances in a person's energy and nutrient intake.
21
All patients' pre-operative nutritional status (BMI, vitamin C, zinc, and albumin) was assessed using Nutrition Risk Screening 2002 (NRS-2022),
22
and those in normal status were included in the study. The enzyme-linked immunosorbent assay (ELISA) method was used to measure vitamin D levels. Blood samples were taken a week before the scheduled surgery from all patients. They were instructed to take oral antibiotics (neomycin 1 g orally and Flagyl 500 mg orally at 1:00
The patients diagnosed with SSI based on criteria developed by the U.S. Centers for Disease Control and Prevention (CDC) were followed up for 30 days. The SSI of the patients was assessed and recorded by the operating surgeons. The SSI was graded using the Clavien-Dindo classification. 23 Following the CDC definitions of SSI, it occurs 30 days after surgery involving a cut (incision) in the skin. There are three types of SSI: superficial (infection occurs just in the skin), deep (infection occurs beneath the incision area in muscle and the tissues), and organ/space infection (can be in any area of the body other than skin, muscle, and surrounding tissue that was involved in the surgery). 24 Accordingly, superficial and deep infections were assessed in this study because most of the emerged wounds were superficial and deep wounds.
Vitamin D concentration below 30 ng/mL showed deficiency. 16 Increasing agreement among researchers indicated that vitamin D lower than 30 ng/mL should be considered low vitamin D status.25,26 Measuring 25-OH vitamin D levels reflect a person's vitamin D supply. A blood 25-hydroxy vitamin D level of 30–100 ng/mL was regarded as sufficient, with concentration between 20 and 30 as insufficient, levels between 7 and 20 ng/mL as a deficiency, and levels lower than 7 ng/mL as severe deficiency.27,28 In this study, values lower than 30 ng/mL are considered low in vitamin D.
Statistical analysis
The Mean ± standard deviation (SD) was used to demonstrate the distribution of continuous variables, and frequencies were measured for qualitative variables. Either χ 2 or Fisher exact test was used to examine categorical variables. The Student t-test or Mann-Whitney U test was used for analyzing binary categorical subgroups (vitamin D deficiency status). The logistic regression test was used to determine the relation between gender (male), age, BMI (kg/m2), vitamin D deficiency, and incidence of infection. The data were analyzed with SPSS version 20 (IBM Corp, Armonk, NY). A p value <0.05 was considered significant. Multiple regressions were not used because there was no statistically significant association between gender, age, BMI, and infection incidence.
Results
The study population included 315 patients with linear open right hemicolectomy surgery; 81 patients were male (25.7%); the mean age was 63.37 ± 12.88 years. The patients had a mean serum vitamin D level of 35.66 ± 13.26 ng/mL. Serum vitamin D levels were found to be <30 ng/mL in 107 patients (34%) and ≥30 ng/mL in 208 patients (66%). The mean body mass index was 25.33 ± 4.33 kg/m2. Overall, SSI was observed in 21 patients (6.7%). Patients' demographic and clinical characteristics are presented in Table 1.
Patient Demographics and Clinical Characteristics Stratified According to Serum 25-OH Vitamin D Levels
BMI = body mass index; SSI = surgical site infection; SD = standard devation.
Mann-Whitney test.
Mean ± SD.
Vitamin D deficiency was shown to be more common in men than in women. The mean age of patients with normal vitamin D levels was slightly higher than patients with vitamin D deficiency (p > 0.05). The mean BMI of patients with normal vitamin D levels and vitamin D deficiency was nearly similar (p > 0.05). The mean serum vitamin D level was 36.39 ± 13.09 and 23.71 ± 9.87 ng/mL among patients without and with infection, respectively (p < 0.001). The incidence of SSI in patients with vitamin D deficiency was higher than in patients with normal levels of vitamin D (p < 0.001; Table 1).
Single logistic regression analysis was performed to demonstrate vitamin D deficiency and independent risk factors of infection (Table 2). The frequency of male patients in the group with SSI incidence was higher than patients without SSI. Male patients had higher odds of SSI incidence than female patients (odds ratio [OR], 2.31; 95% confidence interval [CI[, 0.94–5.71; p < 0.05). The mean age of patients in the group with SSI incidence was less than patients without SSI. (OR, 0.0.97; 95% CI, 0.94–1.01; p > 0.05). The BMI in patients of the group with SSI incidence was almost similar at 30 (OR, 1.07; 95% CI, 0.96–1.2; p > 0.05).
Vitamin D Deficiency and Independent Risk Factors of Surgical Site Infection Using Single Logistic Regression
OR = odds ratio; CI = confidence interval; BMI = body mass index; N = normal; ABN = abnormal.
Statistically significant.
Increased vitamin D deficiency was associated with elevated odds of SSI incidence among the patients after surgery (OR, 5.49; 95% CI, 2.06–14.6; p = 0.001). Vitamin D deficiency was statistically more prevalent in patients with surgical wound infection (Fig. 1).
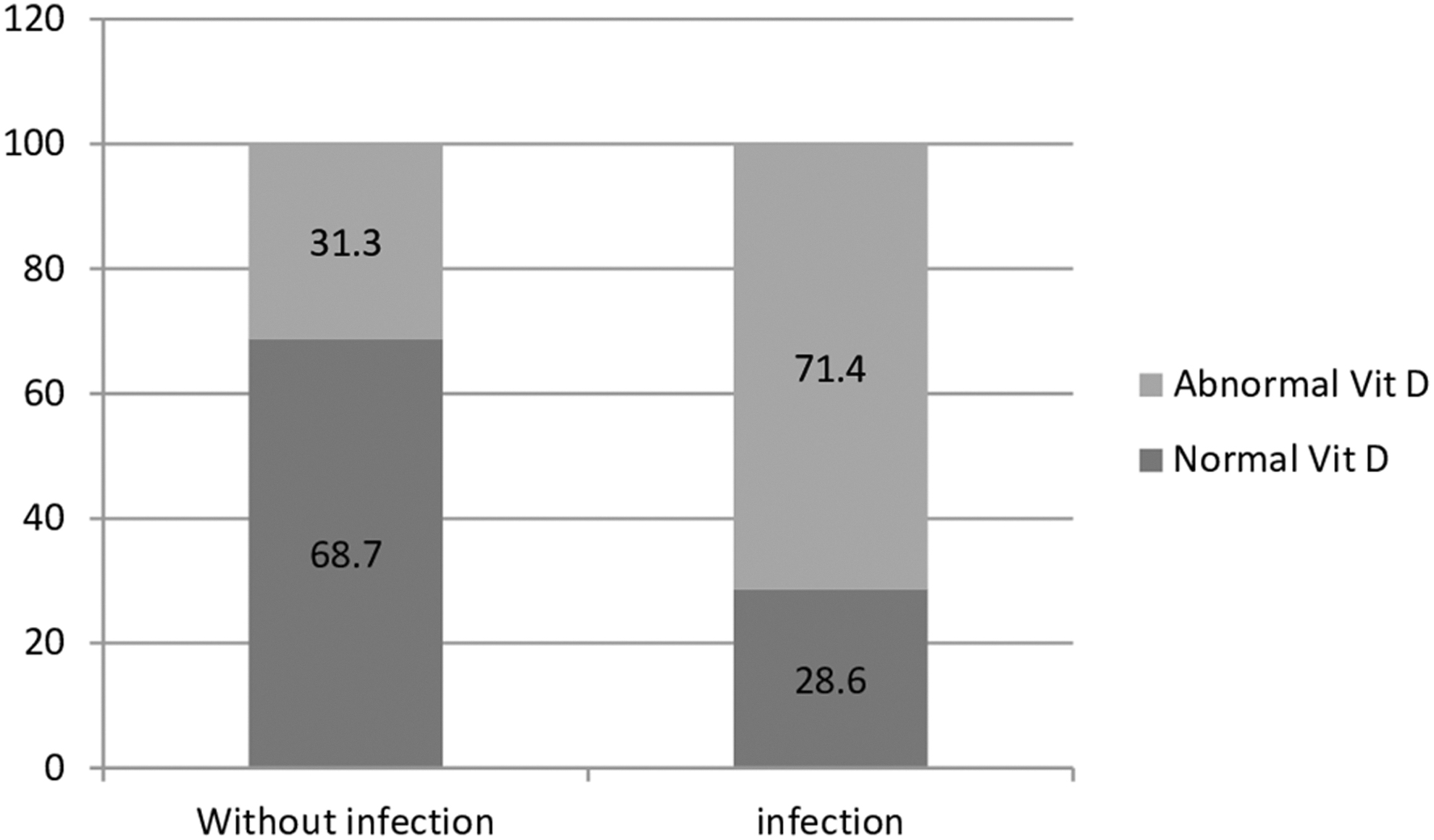
Vitamin D deficiency among patients with or without surgical site infection.
Discussion
Vitamin D deficiency is a universal general health concern 29 and is a risk factor for post-operative complications, particularly wound infection after surgery. In this investigation, the risk of post-operative SSI was negatively connected with serum 25 (OH) vitamin D concentrations. This relation appeared stronger for men than women, although gender was not statistically significant. Furthermore, there was no significant relation between patients' vitamin D, age, and BMI. The incidence of SSI in patients with vitamin D deficiency was higher than in patients with normal vitamin D levels.
In line with these findings, Abdehgah et al. 30 reported a relation between pre-operative vitamin D3 deficiency and post-operative SSI and found that patients with higher pre-operative vitamin D levels were associated with a lower danger of infection. Also, vitamin D concentrations before the operation were reversely linked with wound infections in heart operations and total knee arthroplasty patients.31,32 Quraishi et al. 34 showed that hospital-related infections are connected to insufficient pre-operative 25-OH vitamin D concentrations in individuals who have had bariatric surgery.
In contrast to these results, according to experimental studies on the relation between vitamin D and post-operative complications, no difference was observed in the prevalence of unexpected outcomes between patients with insufficient and greater vitamin D levels. 35 Furthermore, Grandi et al. 36 discovered that low vitamin D concentrations before the surgery did not affect subsequent postoperative cardiovascular problems.
In our population, no connection was reported between patients' vitamin D, age, and BMI, which was supported by Matinkia et al. 37 Likewise, a subsequent investigation by Soleiman et al. 38 showed no connection between vitamin D concentrations and gender, age, and BMI of the studied patients, which is in line with the findings found in our study.
Consistant with the study by Martens et al. 39 our research could infer that vitamin D deficiency had been connected to poor results of post-operative infectious complications because of decreased immunomodulatory effects in hospitalized patients. By considering SSI as a post-operative complication, this study discussed the impact of vitamin D levels on the functions of immune cells in the wound healing process. Vitamin D impacts the immune system by increasing chemotaxis, autophagy, and phagolysosomal function in innate immune cells and increasing the presence of vitamin D receptors on B and T lymphocytes and macrophages. 40 In line with this result, the study by Moromizato et al. 41 has confirmed that vitamin D affects immune, endothelium, and mucosal functioning, glucose, and calcium metabolism. Accordingly, another study indicated that vitamin D affects immunologic cells directly. Its deficiency is associated with infectious illness morbidity and the initiation or advancement of autoimmune illnesses like rheumatoid arthritis, systemic lupus erythematosus, and multiple sclerosis.42
Although our results support emerging insights into post-operative SSI, it is important to highlight its limitations. A study with a larger sample size is warranted for more definitive results, especially to confirm the trends observed. It means controlling all the risk factors that contribute to SSIs and adjusting for the confounders to evaluate one variable is challenging and needs a large population. In addition, although we used a standard criterion such as a surgeon's diagnosis of SSI, our observations had a low risk of measurement bias. Last, we conducted a retrospective study of patients from a single institution, which may also limit the generalizability of our findings. Future studies should aim to pool data from multiple institutions to yield study populations with adequate statistical power to study the relationship between 25-OH vitamin D levels and the risk for post-operative infections after various surgical procedures. Furthermore, limited access to sun exposure because of religious beliefs can be a factor that contributes to vitamin D deficiency, which was not considered in this study.
Conclusions
In conclusion, pre-operative vitamin D insufficiency might be a possible predictor of SSI in patients with open right hemicolectomy. However, further double-blinded randomized clinical trials are needed to draw a firm conclusion for such a strong association and measure vitamin D levels before surgery as a typical method to decrease complications such as SSI after surgery.
Footnotes
Acknowledgments
The authors would like to express their gratitude to the clinical research development unit of Imam Khomeini Hospital, Urmia University of Medical Sciences, for English editing.
This study conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Ethics Committee of Urmia University of Medical Sciences.
Authors' Contributions
Amestejani and Masoudi conceived and designed the experiments and contributed to the analysis and interpretation of the results. Homapour and Rezaei collected the data. Kafili developed the theory and performed the computations. Moosavi wrote the article. All authors discussed the results and contributed to the final manuscript.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
The authors declare that they have no conflict of interest.