
Abstract
Background:
To establish the role of surgical antibiotic prophylaxis (SAP) in the prevention of surgical site infection (SSI) in children undergoing surgery.
Design:
A systematic review and meta-analysis of six databases: MEDLINE (PubMed), EMBASE, CINAHL Plus, Cochrane Library, Web of Science, and Scopus.
Study Selection:
Included studies (irrespective of design) compared outcomes in children undergoing surgery, aged 0 to 21 years who received SAP with those who did not, with SSI as an outcome, using the U.S. Centers for Disease Control and Prevention (CDC) definitions for SSI.
Data Extraction:
Two independent reviewers applied eligibility criteria, assessed the risk of bias, and extracted data.
Results:
A total of six randomized control trials and 26 observational studies including 202,593 surgical procedures among 202,405 participants were included in the review. The pooled odds ratio of SSI was 1.20; (95% confidence interval [CI], 0.91–1.58) comparing those receiving SAP with those not receiving SAP, with moderate heterogeneity in effect size between studies (τ2 = 0.246; χ2 = 69.75; p < 0.001; I2 = 57.0%). There was insufficient data on many factors known to be associated with SSI, such as cost, length of stay, re-admission, and re-operation; it was therefore not possible to perform subanalyses on these.
Conclusions:
This review and metanalysis did not find a preventive action of SAP against SSI, and our results suggest that SAP should not be used in surgical wound class (SWC) I procedures in children. However, considering the poor quality of included studies, the principal message of this study is in highlighting the absence of quality data to drive evidence-based decision-making in SSI prevention in children, and in advocating for more research in this field.
International infection prevention and control (IPC) guidelines provide standardized recommendations for health-care–associated infection (HAI) prevention in adults, but often lack specific information about children. Guidelines in healthcare are important because they inform local implementation of evidence-based measures. 1
Surgical site infection (SSI) is the second most common cause of HAI in high-income countries (HICs), 2 and the most common cause of HAI in low- and middle-income countries (LMICs). 3 Surgical site infection is also the most common complication of surgery in children, representing one-third of all post-operative complications. 4 Zingg et al. 5 found that among children, SSIs were more frequent with increasing age, and suggested that age-adapted strategies for IPC in pediatric settings were needed to combat HAIs, of which SSIs form an important and largely preventable portion. Surgical site infections range in severity, complexity, and effect. Superficial SSIs involve only the skin or subcutaneous tissue; deep SSIs involve primarily fascia and muscle, whereas organ/space SSIs involve specific organs or body cavities. 6
Adults who develop an SSI are twice as likely to die, 60% more likely to stay in an intensive care unit, and five times more likely to be re-admitted to the hospital. 7 These statistics are not available for children; nevertheless, SSIs are a major cause of morbidity and mortality in the pediatric patient, resulting in a substantial burden on the health and well-being of affected children and their families. 8 Surgical site infections lead to increased need for re-operation, and increase hospital stays by an average 10.6 days, hence to loss of work productivity for parents and guardians.9–12
Surgical site infection is the costliest type of HAI with an estimated annual cost of $3.3 billion and is associated with nearly one million additional inpatient-days annually in the United States. 13 In the United States, the Affordable Care Act has led to a focused interest in quality and value initiatives aimed at preventing SSIs because of their attendant financial burden.14,15
Strategies to reduce SSIs have focused on pre-operative patient optimization, operative factors such as surgical antibiotic prophylaxis (SAP), post-operative care, and infection surveillance programs. 16 Standardized SSI prevention protocols utilizing care bundles have been shown to reduce SSI rates in adults irrespective of resource setting,17,18 a strategy that may be as effective in children; SAP is included in every such care bundle.19–22 Surgical antibiotic prophylaxis administered within two hours prior to the surgical incision is an established practice for SSI prevention in adults.3,23,24 The goal of SAP is to prevent SSIs by using safe, cost-effective antibiotic agents that have the appropriate spectrum of activity.25,26
Although the effect of SAP has been well investigated and documented in adults, data on children are limited and SAP use poorly characterized. 27 Araujo da Silva et al. 1 reviewed international IPC guidelines and recommendations for prevention of HAIs, and found that pediatric-specific recommendations for SSI prevention were either totally omitted, or based on a limited number of intervention studies in specific conditions, such as spinal surgery and ventriculo-spinal shunts, and could not therefore be generalized to other conditions.
The most recent World Health Organization (WHO) SSI prevention guidelines highlighted the lack of data in children and thus recommendations were limited to adults only.3,23,28 A combination of low-quality studies in children, a dearth of pediatric SSI data, and an abundance of high-quality adult studies means that the current practice of SAP administration in children is informed entirely by adult data, similar to many other practices in the IPC world.1,29,30 There are many diagnostic and therapeutic differences between children and adults, therefore, the standard IPC practices designed for adults may not be effective or need modifications when applied to a pediatric population.31,32 Neonates for example, are at high risk of infection because of factors such as immunologic immaturity and microbiota implantation; also, antibiotic pharmacokinetics are different compared with older children and adults.33,34 Additionally, although appropriate antibiotic use may be protective for this patient population, inappropriate use exposes them to deleterious adverse effects. 35 Therefore, risk factors for SSI in children derived from studies in adult populations are potentially misleading because of differences in pathophysiology and management.30,36
There exists, nevertheless, a body of evidence across different pediatric surgical specialties investigating the effect of SAP on SSI. However, no systematic review has yet summarized data evaluating the effectiveness of SAP in children. This systematic review and meta-analysis sought to establish the role of SAP in the prevention of SSI in children undergoing surgery.
Patients and Methods
Search strategy and selection criteria
The systematic review protocol was registered with PROSPERO (CRD42019111791), 37 and followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement.38,39 We searched the following databases: MEDLINE (PubMed), EMBASE, CINAHL Plus, Cochrane Library, Web of Science, and Scopus, for studies published in English between January 1993 and August 2020, to ensure included studies were consistent with the U.S. Centers for Disease Control and Prevention (CDC) SSI definitions, first published in 1992. 6
We used a compound search strategy using a comprehensive list of search terms that included exploded Medical Subject Headings (MESH terms) with the following search concepts: surgical antibiotic prophylaxis; children; and surgical site infection, and with synonyms for each search concept. The full search strategy is available in Supplementary Table S1–S3. Included studies, irrespective of design, compared outcomes in children undergoing surgery, aged 0 to 21 years who received SAP (SAP group) with those who did not (no SAP group), with SSI as an outcome, using the CDC definitions for SSI.6,14
The search was conducted independently by two reviewers (P.M.N. and Y.H.). All references identified by the search were imported into Endnote 20 (Clarivate Analytics, Philadelphia, PA); duplicates were removed, and titles and abstracts screened. Full-text articles were reviewed for eligibility; the reviewers compared and agreed on a list of eligible studies. Any disagreements were resolved by discussion between the two authors or, when necessary, via consultation with the senior author (K.K.).
Data extraction
Two authors (P.M.N. and Y.H.) independently reviewed each eligible article and extracted relevant data using a pre-specified data extraction form. Data collection included publication date, country in which study was conducted, country-income status, number of participants, age, gender, degree of contamination according to CDC wound classification, SAP administration, post-operative antibiotic use, and outcomes (SSI, allergy, and other morbidities, or mortality). The Newcastle-Ottawa Quality Assessment Scale 40 was used to assess the quality of included observational studies, while RCTs were assessed using RevMan 5.4. Odds ratios for all included studies comparing SSIs between participants who received SAP, and those who did not, were extracted or computed from reported data, and used to derive the effect size in the meta-analyses.
Risk of bias assessment
Two authors (P.M.N. and Y.H.) independently assessed the risk of bias of included studies using the Cochrane Collaboration's tool for assessing risk of bias in RCTs,41,42 and the Newcastle-Ottawa Scale for Observational Studies. 42 The Newcastle-Ottawa scales were converted to the U.S. Agency for Healthcare Research and Quality (AHRQ) standard thresholds (good, fair, and poor) for interpretation. 43 Results were displayed as tables for both RCTs and observational studies. The possibility of publication bias was assessed visually with a funnel plot.
Data analysis
Meta-analyses of available comparisons from the included studies were performed using STATA, version 17 (StataCorp LLC, College Station, TX). A random effects model assuming a different underlying effect for each study was used to calculate pooled odds ratios, along with 95% confidence intervals. The I2 and a L'Abbe plot were used to assess heterogeneity and dispersion of effects sizes. Meta-analyses were performed for all included studies, with subgroup analysis of RCTs and observational studies. Pooled proportions of SSIs in those who received SAP (SAP group), and those who did not receive SAP (no SAP group) were calculated. Subgroup analyses were performed on type of study, resource setting, surgical specialty, and surgical wound class (SWC).
Results
Database and hand searches yielded 6,901 titles and abstracts; 2,950 duplicates were removed. A further 3,791 were excluded after screening; 160 full-text articles were assessed for eligibility, of which 123 were excluded. Five studies were excluded during data abstraction; 32 studies were included in the meta-analysis (Fig. 1).
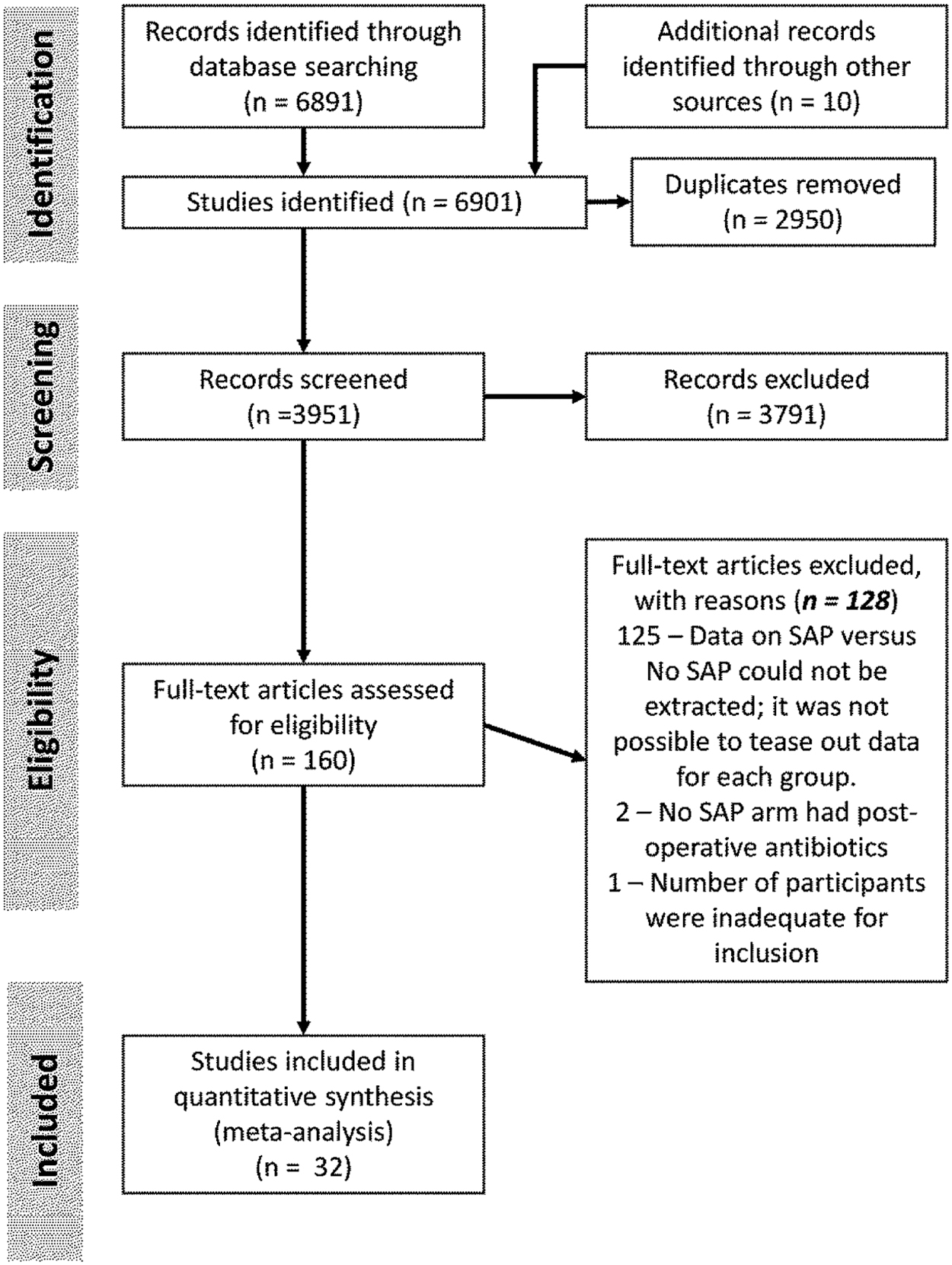
Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram. SAP = surgical antibiotic prophylaxis
General characteristics of included studies
Thirty-two studies met the study criteria for inclusion: six RCTs44–49 and 26 observational studies50–75 including a total of 202,953 children, aged between 0 and 21 years. Five studies used the number of incisions as denominator,44,51,54,73,74 whereas the rest reported individual participant outcomes (Table 1). Overall, more males than females were recruited, with the proportion of boys ranging between 43% and 100%; three studies involved only boys.53,63,69 The 32 studies originated from 17 countries: 12 from the United States,52–54,56–58,60,61,63,65,67,71 three from Canada,59,64,69 two each from Nigeria44,46 and The Netherlands,70,72 and one study each from Switzerland, 50 New Zealand, 51 Germany, 55 Mexico, 62 Estonia, 66 Kenya, 68 India, 45 Nepal, 47 Tunisia, 74 Bangladesh, 75 Sweden, 48 Italy, 49 and the United Kingdom. 73 Twenty-three studies from HICs comprised 98.3% (n = 199,245) of the study participants,48–61,63–65,67,69–73 with the United States contributing the majority (n = 187,106). The six RCTs included a total of 1,825 participants, whereas the 26 observational studies had 201,302 participants. Because of the small number of RCTs, and the limited number of abstractable data for subanalyses from the included studies, the authors present combined analysis of the observational and RCT studies.
Characteristics and Included Studies
US = United States; UK = United Kingdom; SWC = surgical wound class; SSI = surgical site infection; SAP = surgical antibiotic prophylaxis; RCTs = randomized controlled trials; LMIC = low- and-middle income country; UMIC = upper middle income country (included in LMIC for analysis); HIC = high income country; post-opAb = post-operative antibiotic agents; √ = given; X = not given; NS = not stated; NC = not clear; Ind = individual participant counted; Inc = each incision included as individual participant; Gen = general pediatric surgery; ENT = ear, nose, and throat; Card = cardiothoracic; Neuro = neurosurgery; Ortho = orthopedic surgery; Plast = plastic; C = centers; SC = single center; med = median.
Advocated for SAP use.
No evidence for use of SAP.
Bucher, Patients who did not return for review were logged in as negative for SSI.
Wood, Numbers did not add up.
Three studies from the United States used the Pediatric Health Information System (PHIS) database, containing data from more than 45 not-for-profit, tertiary care pediatric hospitals. These accounted for 80% of the total study participants; they reported data on three different procedures: circumcision, orchiopexy, and pyloromyotomy, respectively.53,63,67 The nine studies from LMICs (including four of the six RCTs) had a total of 3,348 participants.44–47,62,66,68,74,75 Twenty-seven studies44–52,54–56,58–62,64–66,68–74 were conducted in single centers, whereas five were multicenter studies.53,57,63,67,75 Twelve studies involved general pediatric surgical patients44–46,48,50,51,55,58,67, 70–72; four studies were focused on pediatric orthopedic surgery,56,61,73,74 three were conducted in urology,53,54,69 and one each in plastic surgery, dental surgery, and otolaryngology, respectively47,49,60; four studies included combinations of two or three specialties each,62,63,65,66 whereas six studies involved patients from all specialties.52,57,59,64,68,75
Risk factors for SSI
Five studies44,57,59,64,66 found a positive association between SWC and SSI. Other factors associated with SSI among study participants were length of surgical procedure and non-compliance with SAP guidelines (underuse and overuse).50,51,57,59,62,64–66 Varik et al. 66 reported a positive association between SSI and length of hospital stay (p = 0.001). Three studies did not find an association between age and SSI,51,57,59 and two of these did not find an association between weight and SSI.51,59 The risk factors identified by the different studies were varied and the data as reported could not be abstracted for subanalyses (Table 1).
Surgical antibiotic prophylaxis-related morbidity
Four studies reported SAP-related allergies,53,60,63,66 two of which found statistically significant higher odds (1.2 and 1.5) of allergic reactions among the SAP group compared with the no SAP group (p < 0.005).53,63 Varik et al. 66 did not comment on whether the allergies reported in their study were attributable to SAP. No SSI- or SAP-related deaths were reported in the included studies. Meta-analysis of the 32 included studies44–75 on the effect of SAP on SSI yielded an odds ratio (OR) of 1.20 (95% confidence interval [CI], 0.91–1.58), comparing children receiving SAP with those who did not (Fig. 2). Meta-analysis of observational studies revealed an OR of 1.34 (95% CI, 1.01–1.79; p = 0.04); meta-analysis of the RCTs favored the use of SAP, but this was not statistically significant (OR, 0.57; 95% CI, 0.26–1.24; p = 0.157).
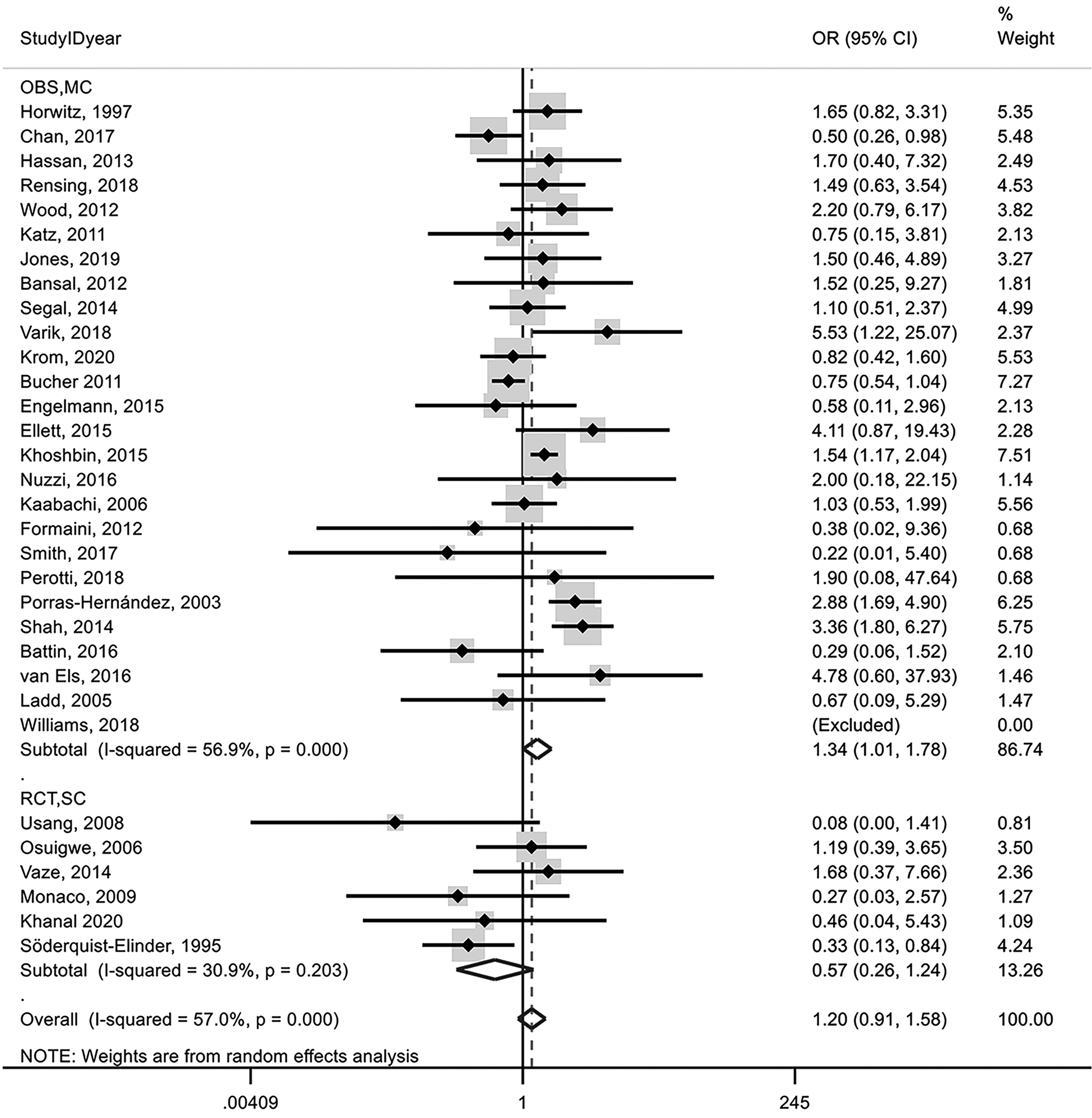
Meta-analysis of all studies. OBS = observational studies; MC = multi-center; RCT = randomized clinical trial; SC = single center; CI = confidence interval.
Usang et al. 44 did not record any SSI in the SAP group, but follow-up was short (7 days) resulting in an OR of 0.08, (95% CI, 0.00–1.41); although this study was a relative outlier, a sensitivity analysis excluding this study did not change the overall pooled results.
The studies exhibited a high degree of heterogeneity (I 2 = 95.15%) in SSI prevalence; 2% (95% CI, 2%–3%) of SAP recipients developed SSI, whereas 1% (95% CI, 1%–1%) of those not receiving SAP developed SSI (Table 2). Subanalysis by specific SWC procedures did not show a statistically significant effect of SAP, albeit with huge heterogeneity (except for the studies focused on SWC I procedures). The pooled odds ratio comparing participants receiving and those not receiving SAP limited to studies including combined SWC I–IV procedures was 2.00 (95% CI, 1.44–2.79) with considerable heterogeneity across studies. Pooled proportions by SWC classes are reported in Table 2. Surgical antibiotic prophylaxis did not decrease the odds of SSI in children managed in general pediatric surgery (OR, 0.72; 95% CI, 0.47–1.18).44–46,48,50,51,55,58,67,70–72 Eight studies reported a positive association between length of surgery and SSI occurrence; in these studies, SAP recipients had 1.82 times higher odds of developing an SSI than those in the no SAP group (OR, 1.82; 95% CI, 1.27–2.63).50,51,57,59,62,66,68,73
Summary of Findings
SAP = surgical antibiotic prophylaxis; SSI = surgical site infection; OR = odds ratio; 95% CI = 95% confidence interval; RCTs = randomized controlled trials; HIC = high income country; US = United States; N = total number of participants in the group.
Subanalysis by resource setting did not show any effect of SAP in studies performed in HICs48–61,63–65,67,69–73 (OR, 1.06; 95% CI, 0.77–1.46), whereas patients receiving SAP in studies conducted in LMICs had higher odds of developing SSI44-47,62,66,68,74,75 (OR, 1.65; 95% CI, 0.99–2.76; I2 = 48.3%). Pooled prevalence of SSI in those not receiving SAP was 6% (95% CI, 2%–9%) in LMICs and 1% (95% CI, 1%–1%) in HICs (Table 2).
There was no difference in effect when investigating the effect of SAP in single versus multicenter studies. There were insufficient data on many factors known to be associated with SSI, such as cost, length of stay, re-admission, and re-operation; it was therefore not possible to perform subanalyses on these.
Heterogeneity and publication bias
The included studies were conducted across 17 countries, involved different pediatric surgical specialties and SWC procedures as well as age groups, creating substantial clinical heterogeneity. Statistical heterogeneity is reflected in the generally wide confidence intervals of the effect sizes and high I2 of pooled estimates. Meta-analysis of proportions of SSI in the two comparison groups yielded high heterogeneity (>38% to 96%). Figure 3 shows that most studies are located along the no effect line, with some outliers indicating heterogeneity.

L'Abbe plot.
Publication bias
The funnel plot of all included studies was asymmetrical suggesting publication bias (Fig. 4). There was no evidence against small study effects on both Egger's test (p = 0.622), and Begg's test (p = 0.793). 76

Funnel plot. OBS = observational studies; MC = multi-center; RCT = randomized clinical trial; SC = single center; CI = confidence interval.
Quality of included studies
The overall quality of the six randomized clinical trials44–49 was low with a placebo being used in only trial one 46 (Table 3). None of the RCTs included a sample size calculation and almost all were underpowered to detect a clinically relevant difference. One RCT 44 followed patients for only seven days likely resulting in outcome misclassification, and ascertainment bias.
Risk of Bias of RCTs
RCT = randomized controlled trial
The average Newcastle-Ottawa Scale scores for the 26 observational studies50–75 was 6.8 (Tables 4 and 5); these scores were converted to the AHRQ 77 standard thresholds: 25 studies were of good quality, whereas one was of fair quality. 55
Risk of Bias of Observational Studies
Newcastle-Ottawa Quality Assessment Scale: A study is awarded a maximum of one star (*) for each numbered item within the Selection and Exposure categories. A maximum of two stars can be given for Comparability. The total number of stars within each study give an aggregate (total) score, which reflects the quality of the study.
AHRQ Standard Thresholds for Risk of Bias of Observational Studies
Discussion
This systematic review and meta-analysis found no evidence of a preventive effect of SAP on SSI in children overall and in subanalyses conducted across SWC procedures, resource setting, and study design. Meta-analysis of the observational studies favored the no SAP group (OR, 0.342; p = 0.043), whereas RCTs favored the SAP group (OR, 0.570; p = 157), and a pooled OR of 1.199, p = 0.198, in favor of the no SAP group. Meta-analysis of proportions of SSI in the two comparison groups yielded high heterogeneity (38% to 96%).
Surgical wound classification was introduced by the National Academy of Sciences in 1964; it divides surgical wounds into four categories based on the potential bacterial load of the wound, and therefore increasing risk of SSI: clean (SWC I), clean-contaminated (SWC II), contaminated (SWC III), and dirty (SWC IV). 78 Surgical wound classification in adults is an important determinant of SSI risk, with SSI guidelines indicating increasing SSI rates with increasing wound contamination (1%–5% for SWC I; 3%–11% for SWC II; 10%–17% for SWC III; and over 27% for SWC IV) 79 ; SWC is also one of the three components that make up the National Nosocomial Infections Surveillance (NNIS) risk index, the most commonly used SSI risk stratification index in adults. 80
Fourteen studies that exclusively focused on SWC I procedures comprised 81.5% of all participants in the included studies. Many authorities hold the view that the risk of SSI in SWC I is so low that SAP does not provide any additional benefit to patients.81,82 Whereas SSI prevention guidelines are unanimous on SAP administration for SWC II to IV for adults,83–85 the management of SWC I remains contentious. Current guidelines on SAP in adults do not recommend SAP for SWC I procedures, except for patients undergoing surgery with placement of prostheses or implants, and the occasional specialty-specific, patient-specific, or institution-specific recommendations. 83 Surgical antibiotic prophylaxis may also be justified for any procedure if the patient has an underlying medical condition associated with a high risk of SSI.83–85 The WHO and CDC SSI prevention guidelines do not provide guidance on SWC-specific SAP, but rather have left it to local or specialty guidelines to determine local practice.24,28
The incidence of SSI in pediatric patients in HICs is estimated at 2% to 5%. 86 In this study, the incidence of SSI in all included studies ranged between 0% and 18.7%; in 10 studies, all from HICs, the SSI incidence was below 1%.52–54,56,60,61,63 The incidence of SSIs in studies conducted in LMICs (1.19%–18.7%) was higher compared with studies from HICs. The pooled SSI proportion among children who did not receive SAP was 1% and 6% in HIC and LMIC studies, respectively. High SSI rates have been reported among adults in LMIC,17,87 but have not yet been systematically reviewed in children.68,88 Our findings are consistent with a WHO SSI estimate of 12.7%, (95% CI, 6.7–20.3) among children in LMIC settings. 28 Although children in LMICs experience higher rates of SSI than those in HICs, there is no evidence that SAP prevents SSIs in LMICs, and multimodal interventions are more likely to lead to successful reduction of SSI rates even in this setting. 17 Surgical antibiotic prophylaxis administration in studies including combined SWC I–IV procedures50,51,57,59,62 64–66 was paradoxically associated with a 1.87 increased odds of SSI among SAP recipients, compared with the no SAP group; inappropriate use of SAP (under- or overuse), allocation bias (if SAP recipients received SAP because of a perceived higher risk of infection), and residual confounding are possible explanations for this result.
A number of authors have not found an association between SAP administration and SSI in children, across different resource settings.86,88,89 Their findings of no benefit of SAP in children are consistent with the results of this review and meta-analysis.
The incidence of SSI in children across all procedures in this review was low: 1% to 2%, with an even lower incidence in children undergoing SWC I procedures (<0.01%). Studies performing only SWC I procedures had limited heterogeneity (I2 = 0%), a statistically non-significant SSI reduction in the SAP group compared with the no SAP group (OR, 0.85; 95% CI, 0.577–1.256; p = 0.416), and equivalent metaproportions between the SAP and no SAP groups with SSI (<0.001%; Table 2). Thus, in SWC I procedures, excluding cardiovascular, spine, and neurosurgic procedures, with such a low SSI incidence, the number needed to treat with antibiotic agents to prevent an SSI would be vast even if SAP were to provide 100% protection, and therefore, the benefit of SAP would be questionable even if a protective effect existed. Unfortunately, except for SWC I studies, the number of patients receiving SAP by SWC was not reported in studies with mixed surgical wound classes, therefore stratified SWC analyses could not be performed to determine the effect of SAP for the different SWC procedures (Table 1).
Although five studies included in this review reported a positive association between SWC and SSI,44,57,59,64,66 two large studies have questioned the utility of the current surgical wound classification in children, arguing that it does not reflect SSI risk in children.15,90 Furthermore, significant inter-observer differences in pediatric surgical wound classification have been reported. 91 Similarly, a number of authors have questioned the value of NNIS risk index among children,32,92 with some proposing either local adaptation of the NNIS index, or even the creation of a new SSI risk index.92,93
Although SAP may be the most important SSI prevention measure in adults, it is not without complications. Surgical antibiotic prophylaxis-related adverse effects include allergic reactions ranging from minor skin rashes to anaphylaxis, Clostridium difficile infection, the emergence of resistant organisms, and mortality. Antimicrobial stewardship is an essential component of SSI prevention, in ensuring appropriate use of SAP, because inappropriate use (both under- and overuse), may increase the rate of SAP-related adverse events including the occurrence of preventable SSIs, the development of multi-drug resistance, and allergies, among other undesirable outcomes; overuse is more frequent among pediatric patients.27,94–97 These complications often lead to increased length of hospital stay, and an increase in health care costs at individual, and the population level.63,94,95,98 Of the 32 included studies, only four reported adverse effects53,60,63 66; it was therefore not possible to perform a subgroup analysis of adverse events.
Given the heterogeneity of the included studies, the absence of a clear benefit of SAP for SSI prevention, and the potential adverse effects resulting from SAP administration, well-designed studies are needed to determine the value and effectiveness of SAP in SWC II to IV, whereas guidelines should at least recommend against SAP administration in SWC I procedures in children, with appropriate exceptions. 30
Surgical antibiotic prophylaxis use and SSI prevention in children
The notion that “children are not just small adults”99–101 is an important consideration in applying SSI prevention measures. These should not be borrowed from adults and applied directly to children: “absence of evidence is not evidence of absence.” 102 This review and meta-analysis presents evidence on pediatric SSIs that suggests the need for a re-analysis of SSI risk factors and therefore preventive interventions in this patient population. Currently, the risk factors are not well defined, whereas SWC and the NNIS risk index are under contention.15,32,90 In adults, the hierarchy of SSI risk factors is well established, allowing for an ethically acceptable and achievable evidence-based prioritization of preventive measures in any resource setting,3,17,23 a situation that is desirable for children as well.
This review and meta-analysis has a number of limitations: included studies had to be in English and only six fairly small RCTs were retrieved, whereas observational studies were heterogenous, with limited abstractable data for subgroup analyses; the bulk of the studies were from HICs, with a disproportionately large contribution from the United States.
This review nevertheless has a number of strengths. It included studies from all types of economies, geographical locations, surgical wound classes, and pediatric specialties. In addition, the study identified a number of gaps in SAP and SSIs in children that will hopefully stimulate research and help improve patient outcomes.
Conclusions
This review and metanalysis did not find a preventive action of SAP against SSI, however, in general, it is to be noted that because of the low-quality RCTs and preponderance of observational studies, residual confounding likely affected the direction of the effect estimates. Furthermore, allocation bias may have led to patients with a high risk of SSI receiving SAP leading to the observed paradoxical higher SSI rates among SAP recipients; these results should therefore be interpreted with caution.
The principal message of this study is in highlighting the absence of quality data to drive evidence-based decision-making in SSI prevention in children, and in advocating for more research in this field. Our results suggest that SAP should not be used in SWC I procedures in children.
Footnotes
Acknowledgments
Part of this work was presented by P.M.N. as a thesis at the London School of Hygiene and Tropical Medicine.
Authors' Contributions
P.M.N. and K.K. designed the study. P.M.N. and Y.H. screened records, extracted data, and assessed risk of bias. P.M.N. performed the statistical analysis. P.M.N., Y.H., G.P., and K.K. analyzed and interpreted the data. P.M.N. drafted the manuscript. All authors provided critical conceptual input, interpreted the data analysis, and critically revised the manuscript, and read and approved the final manuscript.
Funding Information
No funding was received.
Author Disclosure Statement
All authors declare that there are no competing financial interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.