
Abstract

To the Editor:
H
A 27-year-old Chinese male was taken to The First Affiliated Hospital of Southwest Medical University (Lzhou, China) for acute abdominal pain and high fever. Computed tomography (CT) showed hepatosplenomegaly with multiple low-density nodules (Fig. 1A and 1B). Routine blood tests suggested an increased ratio of white blood cells and neutrophils, indicating the possible presence of bacterial infection. There were no abnormal changes in related oncology indicators. The patient has a two-year history of methamphetamine use and has been drug-free for approximately six years. Relevant infection index examination also found no abnormalities. Bone marrow tissue puncture showed that bone marrow hematopoietic cells proliferated actively, and the distribution and morphology of the three lines were normal. Immunohistochemistry showed MPO (granulocytes) and CD235α (red blood cells) positive (Fig. 2A and 2B). The results of liver nodule puncture suggested classic Hodgkin lymphoma. The immunohistochemical results of CD3, CD30, CD15, EBV, LCA, MUMI, and Ki-67 were all positive (Fig. 3A, 3B, and 3C).
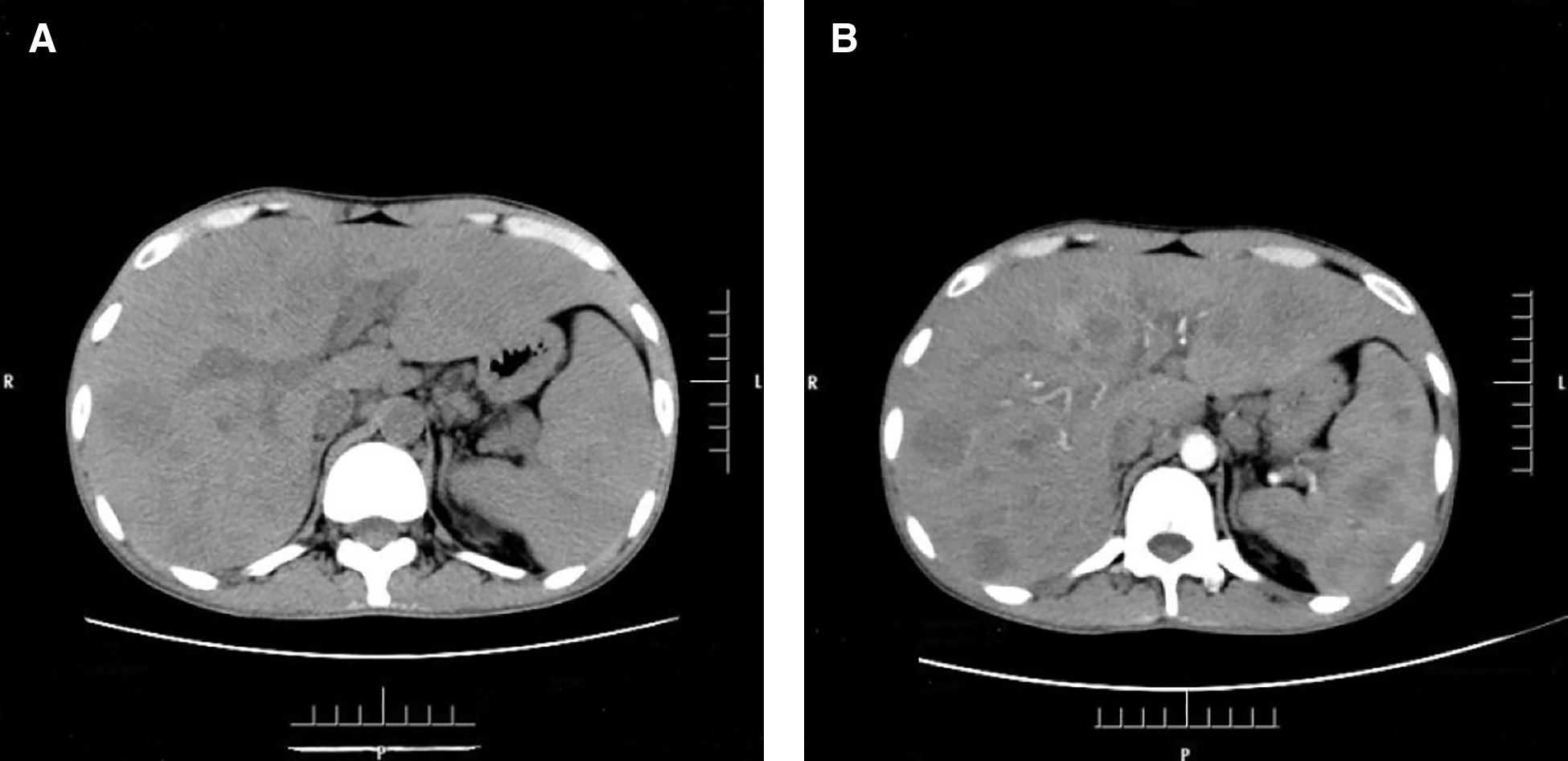
Computed tomography scan. (

Puncture immunohistochemistry was performed on the bone marrow. MPO (granulocyte, +), CD235α (erythrocyte +).

Hepatic puncture histology and immunohistochemical staining.
Because the patient's condition deteriorated, he could not receive chemotherapy or other treatments. The patient eventually chose to leave the hospital. After being discharged, he was followed up by telephone and it was found that the patient still had abdominal pain and high fever. The physical condition further deteriorated and developed into a cachexia state.
Hodgkin lymphoma is an uncommon B-cell lymphoid malignancy composed of two distinct disease entities: the more commonly diagnosed classic Hodgkin lymphoma and the rare nodular lymphocyte-predominant Hodgkin lymphoma [3]. The disease is more frequent in males than in females, and peaks in incidence are noted in young adults and in people older than 60 years [3,4]. The incidence of Hodgkin lymphoma is different in different ethnic groups around the world, with the highest incidence of Hodgkin lymphoma in whites, followed by African and Hispanic, and the least in the east. According to the data of the International Cancer Research Institute, the incidence of Hodgkin lymphoma in Europe and the United States is (2.7 ≤ 2.8)/100,000, whereas that in Asians is (0.3 ≤ 0.7)/100,000 [1,2].
At present there does not appear to be strong evidence to support specific etiologic factors responsible for the development of Hodgkin lymphoma, but some studies have suggested that a link with Epstein-Barr virus (EBV) may be a possible cause. Epstein-Barr virus infection most probably leads to NF-jB activation in EBV-associated cases, and mutations of genes encoding inhibitors and regulators of NF-jB have been detected in a large proportion of EBV-negative cases but the exact etiology and pathogenesis of Hodgkin lymphoma remains unclear [5].
The typical manifestation of Hodgkin lymphoma was painless lymph node enlargement, most of which were found in the neck or clavicle. More than 50% of the patients had mediastinal masses, asymptomatic cough, dysphagia, superior vena cava obstruction, and so on. Twenty-five percent of the patients had systemic symptoms, and B symptoms (fever, night sweats, weight loss) had an impact on prognosis. Unexplained weight loss accounted for more than 10% of body weight within 6 months, and other patients had fatigue and itching.
In determining the optimal treatment for patients with Hodgkin lymphoma, the factors that play a major role include the histologic features of the disease (classic Hodgkin lymphoma compared with nodular lymphocyte-predominant Hodgkin lymphoma), the stage of the disease (particularly whether the patient has early or advanced stage disease), the presence of clinical factors that suggest a poor prognosis, and the presence of systemic symptoms. In general, patients with early-stage disease receive shorter courses of combination chemotherapy followed by involved-field radiation therapy. In contrast, patients with advanced-stage disease typically receive more prolonged courses of chemotherapy, and radiation is added only in select cases [12].
At admission, our patient's general condition was poor and he could not receive chemotherapy and radiotherapy; he could only be treated symptomatically. The treatment effect was poor, as was the prognosis. At present, there is no consensus on the diagnosis and treatment of this typical Hodgkin lymphoma. Other reports will enhance our understanding of this rare disease and help improve its management.