
Abstract
Background:
Coronavirus 2019 (COVID-19) is a systemic disease associated with severe gastrointestinal complications including life-threatening mesenteric ischemia. We sought to review and summarize the currently available literature on the presentation, management, and outcomes of mesenteric ischemia in patients with COVID-19.
Patients and Methods:
The PubMed database was searched to identify studies published between January 2020 and January 2021 that reported one or more adult (≥18 years) patients with COVID-19 who developed mesenteric ischemia during hospitalization. The demographic characteristics, clinical and imaging findings, management, and outcomes of patients from each study were extracted and summarized.
Results:
A total of 35 articles reporting on 61 patients with COVID-19 with mesenteric ischemia met the eligibility and were included in our study. The mean age was 60 (±15.9) years, and 53% of patients were male. Imaging findings of these patients included mesenteric arterial or venous thromboembolism, followed by signs of mesenteric ischemia. Sixty-seven percent of patients were taken to the operating room for an exploratory laparotomy and bowel resection and 21% were managed conservatively. The terminal ileum was the most commonly involved area of necrosis (26%). The mortality rate of patients with COVID-19 with mesenteric ischemia was 33%, and the most common cause of death was multiorgan failure or refractory septic shock. Twenty-seven percent of patients managed operatively died during the post-operative period.
Conclusions:
Mesenteric ischemia in patients with COVID-19 is a devastating complication associated with a high rate of morbidity and mortality. Further efforts should focus on developing strategies for early recognition and management.
The coronavirus disease 2019 (COVID-19) pandemic continues to be a serious global threat. 1 What was originally thought to be an exclusively respiratory infection is now acknowledged to be a disease that involves multiple organ systems. 2 Infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) triggers an inflammatory cascade that rapidly evolves into viral sepsis and multiorgan dysfunction. 3 The gastrointestinal (GI) system is commonly involved with 16-33% of patients with COVID-19 experiencing GI manifestations and nearly 75% of critically ill patients developing at least one GI-related complication during hospitalization.4,5 The most frequently reported complications include transaminitis and paralytic ileus; the most life-threatening complication is mesenteric ischemia.4,5
Mesenteric ischemia affects the small or large intestine and results from reduced intestinal blood flow either from thromboembolic occlusion of the mesenteric vessels (arteries or veins) or from systemic hypotension leading to intestinal tissue hypoperfusion. 6 Acute ischemia is associated with high mortality rates and a rapid diagnosis is often imperative to prevent further deterioration. 7 Although not fully understood or fully proven, early reports and studies suggest that the coagulopathy caused by COVID-19 increases the risk of mesenteric ischemia. 8 However, large comprehensive studies on COVID-19–associated mesenteric ischemia are still missing, and most available data are in the form of case reports or small cohort studies. As a result, we sought to review and summarize the currently available literature on the presentation, management, and outcomes of mesenteric ischemia in patients with COVID-19. A scoping review methodology was selected as the most suitable to achieve this aim (Supplementary Table S1).
Patients and Methods
Search strategy
The authors (A.G., M.E.M., D.A., and H.M.) systematically searched the PubMed (Medline) database from January 1, 2020, to January 1, 2021, using an advanced search strategy to identify studies that reported on mesenteric ischemia in patients with COVID-19. The following keywords were used in the search strategy: “coronavirus,” “COVID*,” “2019-nCoV,” “SARS-CoV-2,” “abdom*,” “intestin*,” “bowel*,” “ischemi*,” “infarct*,” and “necro*.”
Study selection
We included all studies published in English that described one or more adult (18 years of age or older) patients with COVID-19 who developed mesenteric ischemia during hospitalization. A diagnosis of COVID-19 was established clinically, via imaging, or via reverse transcription-polymerase chain reaction (RT-PCR). The authors (A.G., M.E.M., D.A., and H.M.) examined the title and abstracts of the articles followed by full-text review to identify relevant studies. The authors (A.G., M.E.M., D.A., H.M., R.G., J.H., G.V., and H.M.A.K.) performed quality assessment of the selected studies. Duplicates, conference abstracts, and studies without available full text were excluded.
Data extraction
Four authors (A.G., M.E.M., D.A., and H.M.) independently extracted the following datapoints from each eligible study: name of the first author, country where the study was conducted, study design, patients' age, gender, initial symptoms at presentation, physical examination findings, laboratory values, imaging findings, management, intra-operative data, pathology report, post-operative complications, and outcomes. Any disagreements were resolved by consulting with a third reviewer.
Outcome measures
Our primary outcome was in-hospital mortality. Additionally, we also examined the development of several complications commonly associated with SARS-CoV-2 infection such as the use of invasive ventilation, multiple organ system failure, and septic shock. The definitions of these complications were determined by the authors of the original manuscripts.
Results
The study Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram is shown in Figure 1. Our search strategy yielded a total of 304 articles. Fifty studies were identified as potentially eligible through title and abstract screening, of which 35 met the eligibility criteria after full manuscript review. The final analysis included data from 26 case reports, five cohort studies, and four case series. Most studies were conducted in the United States (26%), Italy (17%), and the United Kingdom (14%). Sixty-one patients with a mean age of 60 (standard deviation [SD], 15.9; range, 28–85; interquartile range [IQR], 48–72.5) years were included, of which 32 were male (53%), 10 (16%) were female, and 19 were of unknown gender. Supplementary Table S2 summarizes the clinical characteristics, imaging findings, operative procedures, and outcomes of these patients.
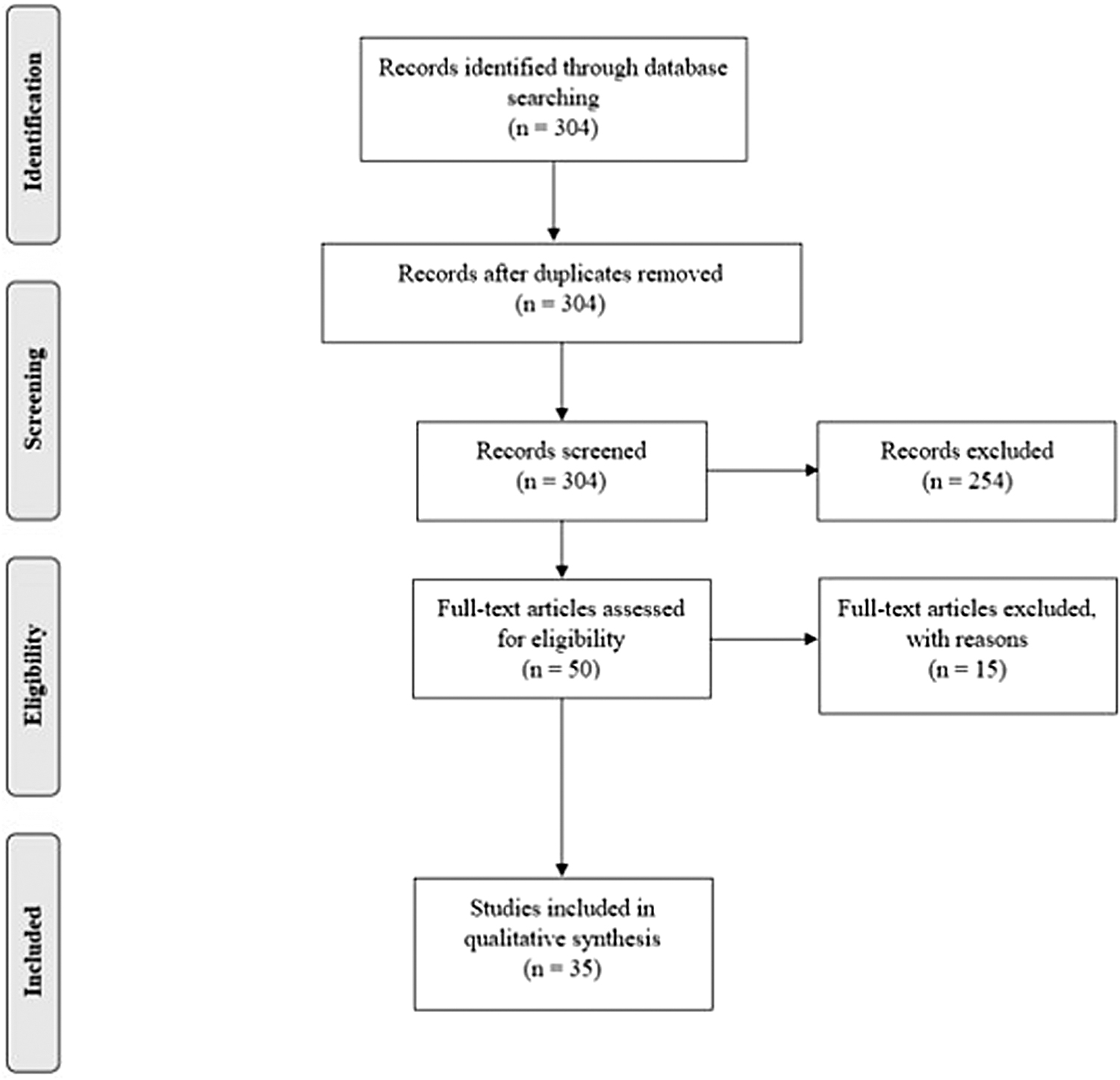
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram detailing the selection process of studies.
Presentation
The most common initial presentations were fever (28%), cough (20%), and shortness of breath (20%). The most common GI manifestations were abdominal pain (33%) followed by nausea and vomiting (18%). Seven patients (11%) who did not exhibit GI symptoms on presentation went on to develop one or more during their hospital stay. Twelve patients (20%) experienced increasing abdominal distension, seven (11%) required new or increasing amounts of vasopressors, and nine (15%) suffered from ileus.
Imaging finding
All patients with suspected mesenteric ischemia had an abdominal computed tomography (CT) scan performed to confirm the diagnosis that demonstrated bowel wall thickening, mesenteric stranding, or pneumatosis intestinalis. Patients with severe ischemia and frank necrosis had evidence of bowel perforation. 9 Nine patients (15%) showed thrombosis of the superior mesenteric vein (SMV) or portal vein, nine (15%) other had signs of occlusion of the superior mesenteric artery (SMA), and one had thrombosis of both the SMA and the SMV. Additionally, three patients (5%) with mesenteric ischemia had patent and well-perfusing mesenteric vessels on CT scan.
Intra-operative and pathology findings
Sixty-seven percent of patients were taken to the operating room for an exploratory laparotomy and bowel resection, and 21% were managed non-operatively or palliatively. The management was not described in 12% of patients. Intra-operative thrombectomy was performed in two cases (3%). The terminal ileum was the most commonly involved area of necrosis (26%) followed by the ascending colon (18%), jejunum (15%), and sigmoid colon (8%). The gross and pathologic examination in all cases was consistent with mesenteric ischemia. Areas of necrosis frequently seen had a distinct well-demarcated yellow discoloration involving the antimesenteric side with patchy or circumferential distribution. 9 Pathology examination in 10 patients reported the presence of fibrin microthrombi in the capillaries underlying areas of necrosis.
Outcomes
In-hospital complications were reported in 14 studies on a total of 20 patients and included multiorgan failure (20%), invasive ventilation (20%), septic shock (20%), isolated renal failure (20%), bleeding (10%), sepsis (10%), and cardiac arrest (5%).
The pooled mortality rate of patients with COVID-19 who developed mesenteric ischemia was 34% with all deaths occurring within the first few days of symptom onset or within five days of surgery (the median time to death was two days [range, 1–4]). Death was most commonly caused by multiorgan failure or refractory septic shock in seven of eight patients who had a reported cause of death. Among patients who were managed operatively, 27% died during the post-operative period. Of the patients who were managed non-operatively or palliatively, 69% died in the hospital, 23% were discharged alive, and 8% had unknown outcomes. Anticoagulation was part of the regimen of 48% of those patients, whereas 15% did not receive any anticoagulant and 37% had no reported data. Among patients who received anticoagulation, 17 patients received prophylactic anticoagulation most commonly with low-molecular weight heparin with a range of 4,000–7,500 IU. Twelve patients were therapeutically anticoagulated with heparin infusion.
Discussion
The exact pathophysiology of mesenteric ischemia in COVID-19 remains elusive. There are currently three prevailing hypotheses that can explain the mechanism of this disease. First, patients with COVID-19 may develop mesenteric ischemia because of systemic hypotension from viral sepsis or because of the high doses of vasopressors they receive. In fact, hemodynamic compromise is implicated in several COVID-19–related complications including acute kidney injury and liver failure.10,11 This phenomenon is not specific to COVID-19 because the risk of mesenteric ischemia has been long described in critically ill patients requiring intensive care. 12 However, this condition typically affects watershed areas, whereas intra-operative findings of patients with “COVID bowel” demonstrated patchy areas of necrosis spanning the entire small bowel.4,5,9,13–36 A recent study by El Moheb et al. 37 showed that patients with COVID-19 are more likely to develop mesenteric ischemia than comparably ill patients without COVID-19. As such, disease severity alone is likely insufficient to explain the high incidence of mesenteric ischemia, and other mechanisms specific to SARS-CoV2 infection are possibly implicated in the development of this complication, as discussed below.
Second, thromboembolic events are a well-established complication of COVID-19. 38 The hypercoagulable state could result in the formation of clots that disrupt the blood supply to the small intestine leading to ischemia. Some patients with COVID-19 who developed mesenteric ischemia had patent and well-perfusing mesenteric vessels on CT scan suggesting occlusion at the microvascular level.4,39 In fact, microscopic examination of resected bowel specimens showed fibrin microthrombi lodged in the capillaries underlying areas of necrosis which was seen in 10 patients in our review. 39 Additionally, patients with COVID-19 have been found to have high levels of von Willebrand factor (vWF). Angiotensin-converting enzyme 2 (ACE2) is a target receptor for SARS-CoV2 and is highly expressed by endothelial cells. It is possible that the virus is binding to ACE2 receptors and damaging endothelial cells thereby releasing vWF into circulation and provoking a hypercoagulable response.14,15 This would explain why thrombosis is observed at the microvascular level and not in larger caliber vessels.
The third plausible mechanism for mesenteric ischemia is direct interaction between SARS-CoV2 and the intestinal tissue. The gut epithelium has the highest expression of ACE2 receptors in the body second only to the lungs. 16 Interestingly, the expression of ACE2 is especially high in the ileum, which was the most commonly involved region of ischemia in patients with “COVID bowel.”4,5,9,16,20,21,23,24,33,40 The virus could be binding to the gut receptors and translocating to the submucosal tissue, subsequently damaging the underlying vasculature and resulting in thrombosis followed by ischemia. This would also explain why large mesenteric vessels remained unaffected whereas capillaries exhibited thrombosis. COVID-induced hepatic injury occurs through a similar mechanism and is likely the result of SARS-CoV2 targeting ACE2 receptors found on cholangiocytes. 41
The current diagnosis of mesenteric ischemia is primarily based on imaging findings. Contrast-enhanced CT scan of the abdomen is particularly important in the early diagnosis of this disease and should therefore be considered in critically ill patients who exhibit GI symptoms. 18 Presence of thick edematous bowel, pneumatosis intestinalis, or portal venous gas should raise suspicion for ischemic bowel. However, imaging findings should be correlated to patients' clinical picture since pneumatosis can also develop as a result of prolonged mechanical ventilation in severely ill patients with COVID-19. 18
Laboratory values such as rising lactate, elevated
Nevertheless, there remains utility in using laboratory values to identify patients who are at high risk of developing severe GI complications. Recent studies have demonstrated that routine monitoring of the coagulation profile of critically ill patients with COVID-19 may be beneficial in early diagnosis of mesenteric ischemia. 43
The findings in the literature raise the question as to whether anticoagulants play a role in preventing mesenteric ischemia. Interestingly, critically ill patients with COVID-19 who were admitted to the intensive care unit developed mesenteric ischemia despite receiving prophylactic anticoagulation. 44 When matched on baseline characteristics and disease severity, patients with COVID-19 were as likely to develop pulmonary embolism and deep venous thrombosis as critically ill patients without COVID-19 but were significantly more likely to develop mesenteric ischemia. 37 Therefore, it could be that higher doses of anticoagulation are needed in high-risk patients with COVID-19 to prevent this life-threatening complication. However, the appropriate dose is still the subject of debate ranging from prophylactic, intermediate, and therapeutic.
The mainstay treatment of mesenteric ischemia in patients with COVID-19 is surgical and involves urgent resection of any necrotic bowel. Endovascular thrombectomy is occasionally performed to recanalize the occluded mesenteric vessels and restore blood flow to the intestines.20,34 There are also reports of hemodynamically stable patients who likely had reversible ischemia and were managed conservatively with anticoagulation without undergoing surgery.13,45
Our study has several limitations. First, our search was limited to one database, and it is possible that other published manuscripts discussing COVID-19–related mesenteric ischemia were missed as a result. Second, we only examined articles published during the first wave of the pandemic. This provides a better understanding of COVID-19–related mesenteric ischemia in the absence of vaccines or therapies that could alter the effect of SARS-CoV2 on the intestines. More recent evidence in the era of widespread vaccination and antiviral therapies deserves a separate review of its own. Third, we relied on the definitions of mesenteric ischemia and its complications used by the authors of the original manuscripts. Many case reports were brief with limited information pertaining to diagnostic criteria used for in-hospital complications.
Conclusions
Mesenteric ischemia is a devastating complication in patients with COVID-19 and is associated with a high rate of morbidity and mortality. Although laboratory tests are useful in identifying at-risk patients, CT imaging of the abdomen is the mainstay for diagnosing this condition. Further efforts should focus on identifying predictors and early markers of disease and determining whether high-dose anticoagulation could prevent mesenteric ischemia in at risk patients. Additional efforts should focus on elucidating the incidence of mesenteric ischemia after infection with new COVID-19 variants.
Footnotes
Funding Information
No grants or other forms of funding or assistance were utilized in the creation of this manuscript.
Author Disclosure Statement
We certify that all listed co-authors have no commercial associations that might create a conflict of interest in connection with submitted manuscripts.
All the co-authors were integrally involved in the writing of this manuscript via study conception/design and/or data acquisition and analysis/interpretation. Furthermore, all authors made significant contributions to the drafting or critical revisions of the manuscript, and all authors gave final approval prior to submission for publication and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.