
Abstract
Background:
To evaluate systematically the failure rate of short versus long courses of antibiotic agents for prosthetic joint infections (PJIs).
Methods:
PubMed, Embase, and Cochrane Library databases were searched for controlled studies of short- and long-course antibiotic agents for joint prosthesis infections, all from the time of database creation to April 2022. Literature search, quality evaluation, and data extraction were performed independently by two researchers, and the primary outcome was the rate of surgical failure after antibiotic treatment. Stata 11.0 software was then applied for meta-analysis. Publication bias was assessed using Begg test. Heterogeneity was assessed using the I2 test, and fixed or random effects models were used accordingly. Meta-regression was used to determine the causes of heterogeneity.
Results:
A total of 14 articles involving 1,971 participants met the inclusion criteria, including 12 observational studies and two randomized controlled trials. Meta-analysis showed no difference between short and long courses of antibiotic agents (relative risk, 1.08; 95% confidence interval [CI], 0.89–1.32). The results of the subgroup analysis showed no differences between the failure rates of patients with PJI treated with short and long courses of antibiotic agents in studies with different study areas, different treatment modalities, and different locations of the artificial joints.
Conclusions:
Patients with PJIs may not require long-term or lifelong antibiotic agents after surgical treatment, and short-term (four to six weeks) antibiotic therapy is usually safe.
Prosthetic joint infection (PJI) is a catastrophic complication after arthroplasty with an incidence of 1% [1] and is challenging and costly to treat [2,3]. The main treatment modalities for PJI include debridement, antibiotic agents, and implant retention (DAIR); arthroplasty, including stage 1 arthroplasty and stage II arthroplasty (staged exchange arthroplasty [SEA]); and permanent removal of the prosthesis, including amputation in very severe cases such as necrotizing fasciitis [4].
There is no consensus on the duration of post-operative antibiotic therapy for patients with PJI, and in clinical practice, it is usually recommended that patients receive long-term antibiotic therapy, with one survey study showing that 41% of physicians would recommend lifelong oral antibiotic therapy for patients receiving DAIR for PJI [5]. In contrast, long-term antibiotic therapy may prolong the patient's hospital stay, increase the incidence of adverse events, add to the financial burden, and may lead to antibiotic resistance [6]. However, studies on the optimal duration of antibiotic therapy for patients with PJI have been reported inconsistently. A study by Byren et al. [7] showed a four-fold increase in treatment failure in patients with PJI after discontinuation of antibiotic agents. Laffer et al. [8] showed that in patients with PJI, antibiotic treatment for three to six months was similar to antibiotic treatment for more than six months. A large multicenter prospective randomized controlled study by Louis et al. [9] in 2021 showed that in patients with PJI, six weeks of antibiotic therapy was no less effective than 12 weeks of antibiotic therapy in these patients. Therefore, our goal was to summarize the available evidence and analyze the difference in efficacy of short- and medium-course antibiotic therapy versus long-course regimens.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Literature search
Studies comparing long- versus short-course antibiotic agents for PJI were searched in PubMed, Cochrane, and Embase databases with a search time frame from build to April 20, 2022. Advanced searches are performed using the following terms ((antibiotics) OR (Anti-Bacterial Agents)) AND ((treatment duration) OR (Duration of Therapy)) AND ((PJI) OR (Prosthetic joint infection)). Duplicate articles in the database were removed. Two researchers read the titles and abstracts of the literature separately for screening studies.
Inclusion and exclusion criteria
We included studies that incorporated studies comparing the effects of long-term and short-term antibiotic therapy in patients with PJI. Exclusion criteria was: studies for which full text was not available; studies not in English; duplicate studies; studies lacking post-treatment failure rates; and studies of PJI caused by non-bacterial organisms. Two researchers performed literature screening based on inclusion and exclusion criteria by reading the full text. Disagreements emerged and were resolved through discussion with a third researcher.
Quality evaluation
For case-control studies, quality was evaluated using the Newcastle-Ottawa Quality Assessment Scale (NOS). The total score of this scale is nine, and studies with a score greater than or equal to six are considered as medium- to high-quality studies. For randomized controlled studies, the quality of the studies was assessed using the Jadad scale [10], which has a total score of five.
Data extraction
Data extraction was performed by a single investigator, and extracted data included study details, patient information, procedure, duration of antibiotic treatment, and definition of treatment failure.
Data analysis
I2 was used to assess the heterogeneity of the studies [10]. If I2 > 50%, it indicates high study heterogeneity and a random effects model was used to combine statistics, whereas if I2 < 50% it indicates low study heterogeneity and a fixed effects model was used to combine statistics; p < 0.05 was considered a statistically significant difference. Sensitivity analysis was used to assess the robustness and reliability of the combined results. Meta-regression was used to find sources of heterogeneity. Publication bias was assessed using Begg and Egger tests. Data analysis was performed using Stata, version 11 (StataCorp, College Station, TX) software.
Results
Search results
Fourteen articles [7–9,11–21] met our pre-defined inclusion criteria, including two RCTs and 12 observational studies (Fig. 1). The 14 studies included 1,971 patients. There were 750 patients in the short- and medium-term groups and 872 patients in the long-term group. Eight studies were from Europe, four from North America, and two2 from Asia, and the basic characteristics of the included studies are shown in Table 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram representing search and selection of studies.
Basic Characteristics of the Included Studies
TKA = total knee arthroplasty; THA = total hip arthroplasty; IV = intravenous; S/S = signs or symptoms; ALCS = antibiotic-loaded cement spacer; RA = rheumatoid arthritis; SD = standard deviation; IQR = interquartile range; DAIR = debridement, antibiotic agents, and implant retention; SEA = staged exchange arthroplasty; MSIS = Musculoskeletal Infection Society; PJI = prosthetic joint infection; RCT = randomized controlled trials; CRP = C-reactive protein.
Of the 12 observational studies, two prospectively collected data, whereas others retrospectively reviewed medical records. Most studies focused on total knee arthroplasty (TKA) or total hip arthroplasty (THA), however, one study also included ankle, shoulder, and elbow arthroplasty. Four studies focused on TKA and one on THA only. In seven observational studies, PJI received DAIR treatment, whereas in four studies, patients received SEA treatment. The other three studies used a mix of treatment types, including DAIR and SEA. In the quality assessment, five were considered good, five were considered fair, and two were considered poor.
Two randomized controlled trials (RCTs) were conducted, one for DAIR-treated TKA and THA with a Jadad score of two, the other was an RCT comparing DAIR, SEA-treated TKA and THA with a Jadad score of five.
Results of the meta-analysis
Most of the included studies evaluated the efficacy by assessing patients' symptoms, remission of signs, improvement in imaging images, or decrease in infection indicators (C-reactive protein [CRP] or erythrocyte sedimentation rate, etc.), whereas the study by Hsieh et al. [14] only considered persistent infection rather than re-infection as treatment failure. We defined the events of death, re-infection, and persistent infection associated with patients with PJI as treatment failure.
Our overall meta-analysis showed no significant difference between the short- and long-course groups (relative risk [RR], 1.08; 95% confidence interval [CI], 0.89–1.32; Fig. 2). Heterogeneity between studies was moderate (p = 0.05; I2 = 41.8%), and meta-analysis was performed using a fixed-effects model. According to Begg and Egger tests (p = 0.931, p = 0.911), there was no publication bias. The funnel plot showed no publication bias in the included studies (Fig. 3). When we excluded any individual study, the plots with effects showed no substantial change in the results (Fig. 4). Because there was moderate heterogeneity between studies, meta-regression was used to explore factors that may contribute to heterogeneity.

Forest plots of the effects of short- versus long-course antibiotic agents on treatment failure. The left side represents short course, the right side represents long course.

Funnel plot of the effects of short- versus long-course antibiotic agents on treatment failure in prosthetic joint infection (PJI).
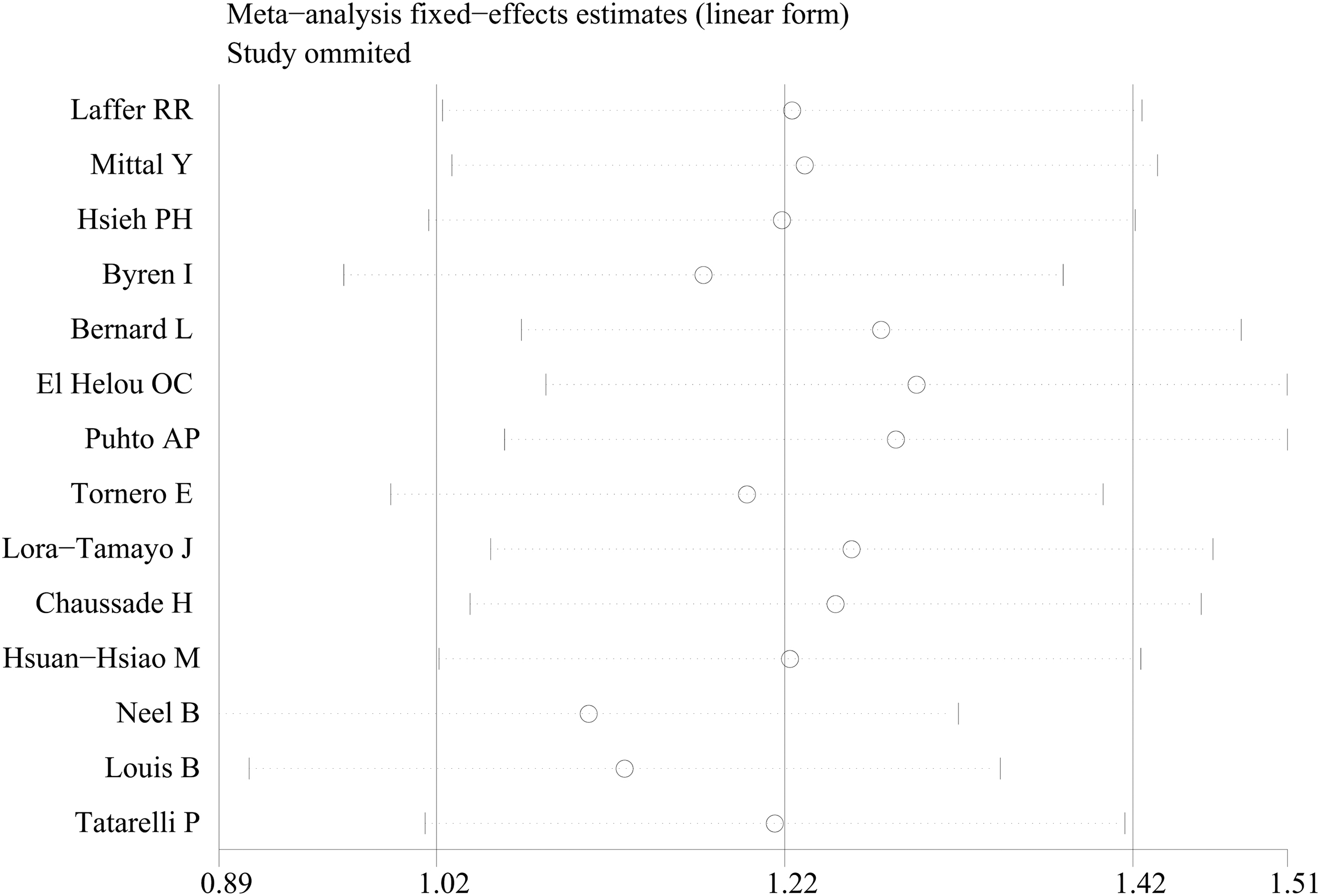
Sensitivity analysis chart for the main results.
Regression results indicated that treatment modality, anatomic location and study area were not sources of heterogeneity (p = 0.826, p = 0.210, p = 0.138). However, considering that a stratified analysis of patients' treatment modality, anatomic location, and study area is still meaningful, a subgroup analysis was performed according to treatment modality, anatomic location, and study area.
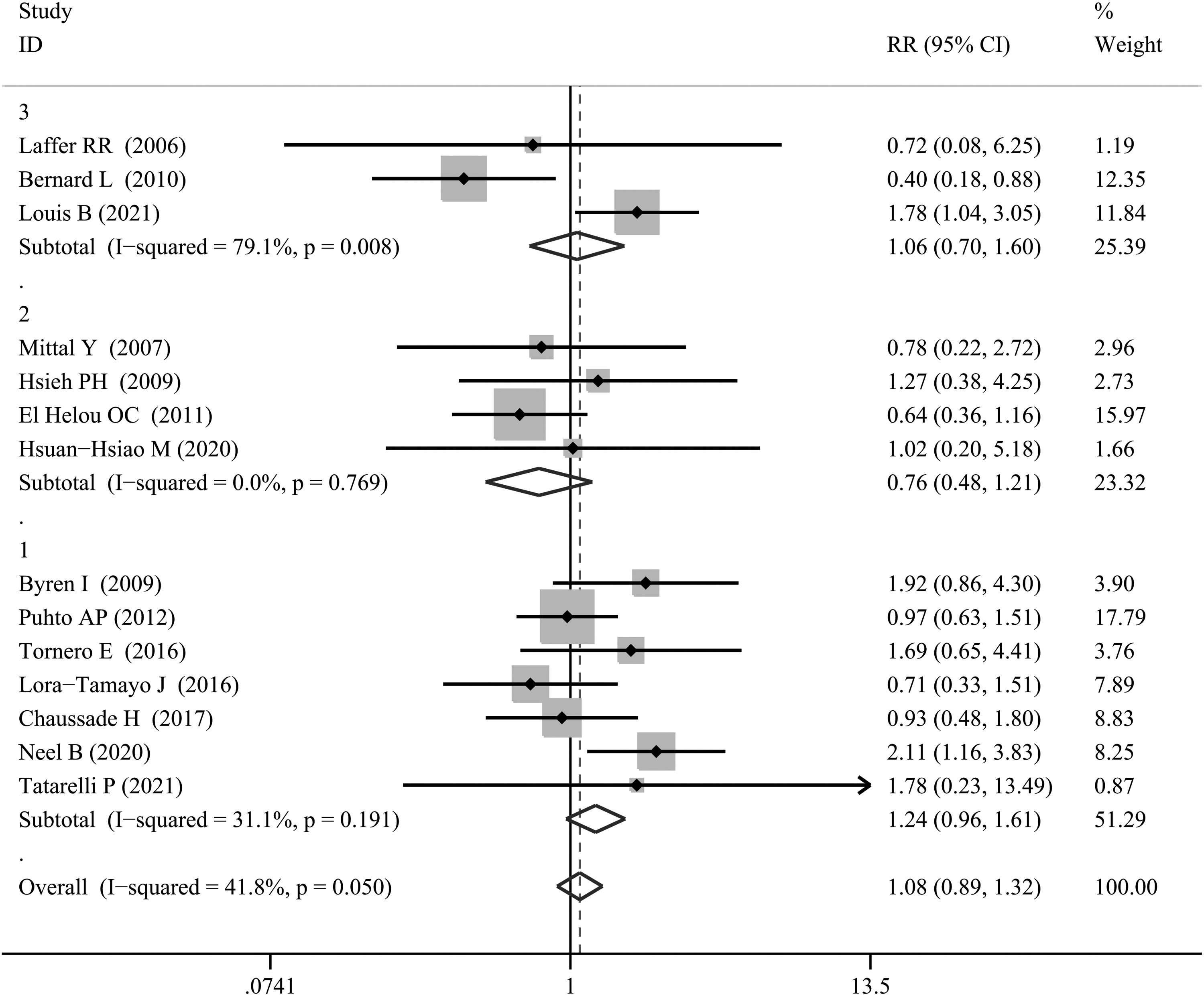
We divided the study into three subgroups for analysis according to the treatment modality chosen for the study (DAIR, SEA, or DAIR and SEA) and showed no significant difference in failure rates between the short and long treatment groups within each of the three subgroups (Fig. 5). We divided the study into three subgroups for analysis based on the location of the prosthetic joint replacement surgery targeted by the study (TKA; THA; or TKA and THA), and the results showed no significant difference in failure rates between the short- and long-course groups within each of the three subgroups (Fig. 6). We analyzed the studies into three subgroups according to the region for which the study was conducted (United States; Asia; or Europe) and showed no significant difference in failure rates between the short- and long-course groups within each of the three subgroups (Fig. 7).
Subgroup analysis chart according to treatment modality (DAIR; SEA; or DAIR and SEA). The left side represents short course, the right side represents long course. DAIR = debridement, antibiotic agents, and implant retention; SEA = staged exchange arthroplasty.
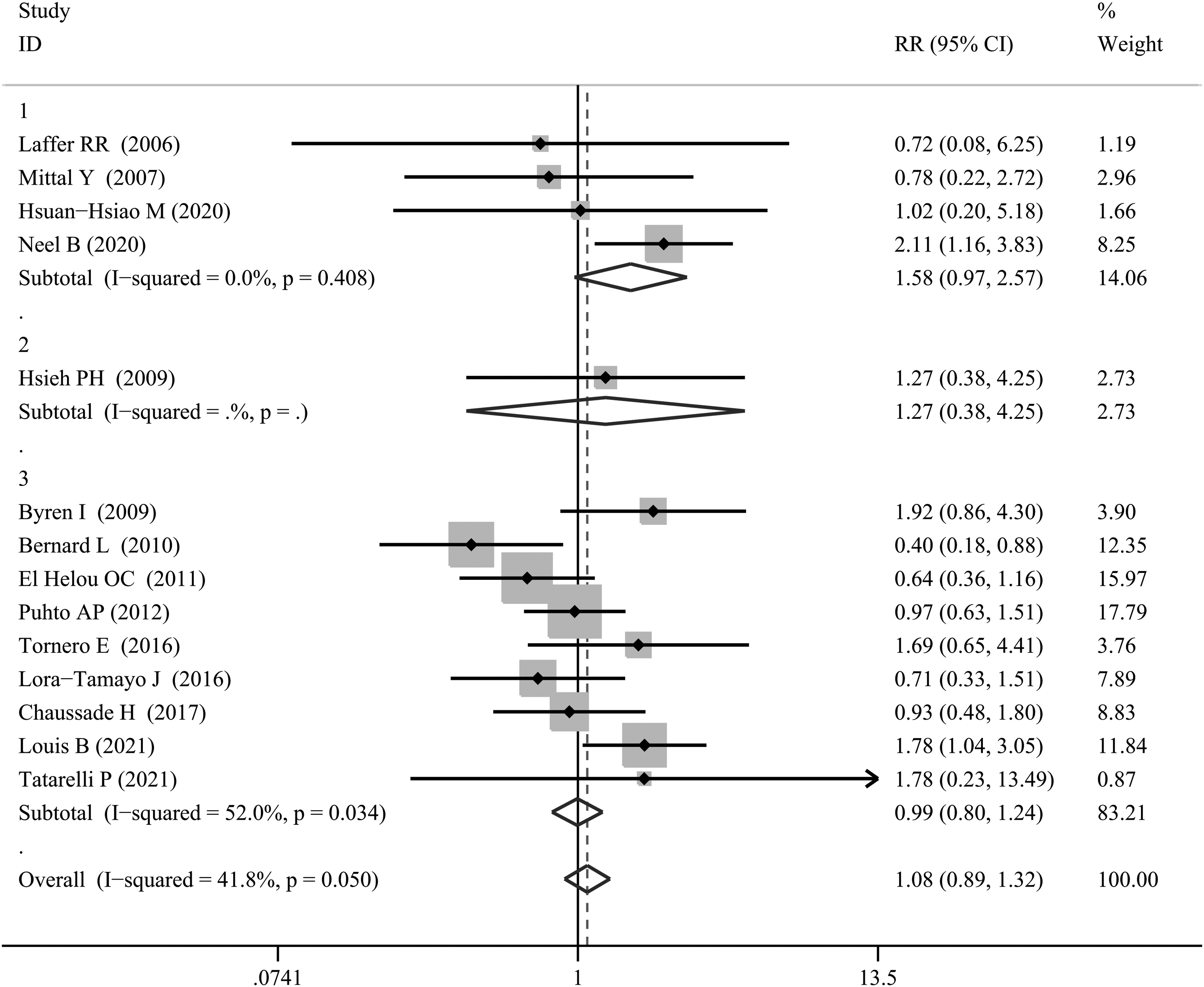
Subgroup analysis chart according to the anatomical position of the artificial joint (TKA; THA; or TKA and THA). The left side represents short course, the right side represents long course. TKA = total knee arthroplasty; THA = total hip arthroplasty.

Subgroup analysis map according to the study area (United States; Asia; or Europe). The left side represents short course, the right side represents long course.
Discussion
Prolonged antibiotic regimens are associated with increased adverse events [22], and the emergence of antibiotic-resistant strains [23,24], whereas inadequate regimens can lead to treatment ineffectiveness and recurrence of infection [25]. The duration of antibiotic therapy in patients with PJI has not been determined. In this study, we compared the clinical outcomes of patients with PJI who received a short course and a long course of antibiotic therapy. Among the included studies, the failure rates were 23.2% and 20.1% for the short- and long-course groups, respectively, and interestingly, the meta-analysis found similar failure rates between the short- and long-course groups.
We divided the study into three subgroups for analysis according to the treatment modality chosen for the study (DAIR; SEA; or DAIR and SEA) and showed no significant difference in failure rates between the short- and long-treatment groups within each of the three subgroups. The duration of antibiotic agents depends on the surgical intervention and the type of micro-organism. Current guidelines recommend that patients with PJI receive six weeks of treatment after DAIR and four to six weeks after single-stage and two-stage revision arthroplasty [26,27]. The results of our meta-analysis showed no significant difference in failure rates between the short-course and long-course groups, with one study [19] in which patients with peri-prosthetic knee infections who underwent two-stage replacement arthroplasty received short-term antibiotic therapy for less than one week.
Patients with PJI treated with DAIR in another study received short courses of antibiotic agents for less than four weeks, and the duration of post-operative antibiotic use in patients with PJI in both studies was less than that recommended by the guidelines. In contrast, the duration of treatment in the short-course group in most of the included studies was four to six weeks, which is consistent with current guidelines.
In 2019, Yen et al. [28] conducted a meta-analysis of ten studies comparing the efficacy of short-term versus long-term antibiotic agents in PJIs and found no significant differences between short- and long-course antibiotic agents, consistent with the findings of this study. The present study has several advantages over the study by Yen et al. [28] First, the number of included studies is higher and the quality is higher compared with the study by Yen et al.28 The present study includes the most recent large prospective RCTs.
This meta-analysis has some shortcomings. First, this meta-analysis included non-randomized controlled studies and the data may be affected by confounding factors. Second, limited by the availability of detailed data in the original study, there was no way to stratify the analysis according to factors such as infection with different micro-organisms and duration of symptoms before treatment. Third, the length of follow-up varies between studies, which may affect the final results. Fourth, we used χ2 tests and the I2 statistic to assess heterogeneity between studies, and although meta-regression was used to look for sources of heterogeneity, the regression results indicated that treatment modality, anatomical location, and study area were not sources of heterogeneity. Fifth, studies differed in their inclusion and exclusion criteria, with some studies including only patients with artificial joint replacements infected with a single species of bacteria (e.g., Pseudomonas aeruginosa); however, we did not find significant heterogeneity in the studies by sensitivity analysis. Finally, the present meta-analysis is limited by the number and quality of included studies and the conclusions need to be validated by larger, multi-center, RCTs with longer follow-up.
Conclusions
In conclusion, based on the best available evidence, there is no significant difference in failure rates between short and long courses of post-operative antibiotic therapy in patients with PJI.
Footnotes
Authors' Contributions
Formal analysis: Jia. Data curation: Jia. Writing–original draft: Jia. Writing–reviewing and editing: Jia, Peng, Chen. Resources: Peng, Liang, Xiong. Supervision: Peng. Conceptualization: Wang. Methodology: Wang. Project administration: Wang. All authors read and approved the final manuscript
Data Availability
If required, detailed data can be provided by contacting the corresponding author.
Funding Information
No funding was received.
Author Disclosure Statement
The authors have no conflicts of interest to declare.