
Abstract
Background:
Peri-prosthetic joint infection (PJI) has long been a devastating complication after total knee arthroplasty (TKA), with native skin flora always identified as the causative agents. The aim of this study was to investigate the efficacy of pre-admission use of chlorhexidine-impregnated gauze for pre-operative skin preparation on infection rates after primary TKA surgeries.
Patients and Methods:
Patients undergoing TKAs performed from January 2017 until January 2021 were prospectively recruited. The experimental group included patients who used chlorhexidine-impregnated gauze the evening before surgery for skin preparation. These patients were compared with a retrospective cohort of TKAs performed during the previous four years without this step as control group. During a one-year follow-up, complications including PJI and superficial infections were collected as the primary outcomes for analysis.
Results:
A total of 1,218 TKAs in the experimental group and 1,033 TKAs in the control group were included in the study. A total of seven (0.6%) cases of PJI were identified in the experimental group, whereas 16 (1.5%) cases were diagnosed in the control group; a significant difference was detected (χ2 = 5.245; p = 0.022). Eighteen (1.5%) cases of superficial infection were identified in the experimental group, and 28 (2.7%) cases were observed in the control group; a significant difference was found between groups (χ2 = 4.243; p = 0.039). No significant differences were found on other wound-related complications.
Conclusions:
Pre-admission use of chlorhexidine-impregnated gauze for skin preparation was found to be an effective practice in reducing the incidence of PJI after TKA procedures, which has the potential of being utilized for patients undergoing TKA surgeries.
Total knee arthroplasty (TKA) has been identified as the most successful and cost-effective procedure for reducing pain and restoring function in patients with end-stage osteoarthritis affecting the knee.1,2 Peri-prosthetic joint infection (PJI) is commonly considered one of the most severe complications after TKA surgery, with a reported incidence of 1%–3% post-operatively.3–5 Not only does this complication have devastating impact on patients with mortality rate nearly doubling, but it also causes economic burdens because it substantially delays recovery and requires multiple re-operations thus increasing lifetime expenditures.6,7 With an aging population, the number of patients needing arthroplasty has increased dramatically, all of whom are exposed to PJI. 8 Therefore, prevention of PJI has become important to the practice of a TKA procedure because of the overwhelming consequences.
Operating room air and native skin flora have been identified as the main sources of surgical site contamination.9,10 Many interventions targeting the causes have been proposed to reduce PJI risks, which include reducing operation room foot traffic, positive pressure ventilated or laminar airflow for decreasing airborne microbe load, 11 as well use of a wrap with antiseptic reagents for lessening the colonization of the skin flora. 12 Chlorhexidine is one of the most widely used antiseptic agents against a variety of gram-positive and gram-negative organisms. It exerts both bactericidal and bacteriostatic mechanisms of action through the mechanism of direct disruption on the organisms' membrane permeability.13,14 Therefore, pre-admission use of chlorhexidine-impregnated gauze the evening before surgery may demonstrate its ability to decrease post-operative infection risk.
Although a few studies have attempted to investigate the topic, inconsistent conclusions arrive have been drawn15–17 and evidence is limited, whereas the level of the evidence is low thus far as well. Therefore, we conducted this prospective cohort study with retrospective controls to investigate the efficacy of pre-admission use of chlorhexidine-impregnated gauze for skin preparation pre-operatively on infection rates after primary TKA procedures.
Patients and Methods
Patient selection
This prospective cohort study with retrospective controls was conducted at a tertiary care center, after Institutional Review Board approval. According to clinical practice, patients undergoing a primary unilateral TKA with chlorhexidine-impregnated gauze utilized for skin preparation the evening before surgery were prospectively enrolled from January 2017 until January 2021 as the experimental group. Arthroplasties performed in the four years prior to January 2017 served as controls, because chlorhexidine-impregnated gauze was not used before this date. Patients were excluded based on the following criteria: unable to comply with the study requirements or chose not to participate; revision TKA surgery; rheumatoid arthritis or tuberculous arthritis; medical history of immunosuppression, such as status post-organ transplantation, human immunodeficiency virus, or long-term hormone usage; poorly controlled diabetes mellitus; chronic hepatitis B or C infection; had surgeries on the ipsilateral lower extremity; experienced an inflammatory or irritation because of the closed-prolonged contact with the chlorhexidine gluconate and isopropyl alcohol.
Intervention
All surgeries were performed under the standardized protocol of a TKA procedure at our institution so that the only procedural change during the study period was the pre-operative skin preparation. The evening before surgery, the operative knees in the experimental group were wrapped with chlorhexidine-impregnated gauze containing 2% and 70% isopropyl alcohol (ChloraPrep, CareFusion, Leawood, KS). Those patients were prospectively enrolled after January 2017 at the beginning of the research period. Those patients who underwent TKA surgeries before January 2017 without pre-operative skin preparation were retrospectively reviewed as controls. All patients enrolled underwent a standard infection control practice during the peri-operative period other than the pre-operative skin preparation. The surgical site was sterilized with aniodine povacrylex and isopropyl alcohol solution (3M DuraPrep Surgical Solution, Saint Paul, MN). Non-permeable sterile drapes were used with adhesive films containing iodine for asepsis. Intravenous antibiotic prophylaxis was administrated half an hour before the start of surgery and was stopped within 48 hours post-operatively. Drainage was removed within 48 hours, and gauze was changed every two days to assess incision healing status.
Outcomes
Patients were followed for at least one year post-operatively to monitor any incision-related complications. Peri-prosthetic joint infection was identified as defined by the Musculoskeletal Infection Society 18 ; these patients were followed with debridement, drainage, or revisions. Superficial infections involving the skin and subcutaneous tissue of the incision were documented based on the diagnostic criteria proposed by the U.S. Centers for Disease Control and Prevention (CDC). 19 Other complications were collected and recorded in detail as well.
Statistical analysis
Data analysis was performed using standard statistical software SPSS, Version 22 (IBM Corp, Armonk, NY). Pearson χ 2 tests or Fisher exact tests and independent Student t-tests were used to compare the baseline and outcome variables between groups. A p value <0.05 was considered as statistically significant.
Results
A total of 2,572 TKAs were screened for eligibility during the study period, among which 316 TKAs were initially excluded according to the exclusion criteria. Thus, 2,256 TKAs were enrolled in the study based on January 2017 being the point at which a different pre-operative skin preparation was used. Of these, 1,223 TKAs were allocated to the experimental group for prospective investigation and 1,033 TKAs allocated to the control group for retrospective review; incomplete data were excluded at the beginning for the retrospective cohort. In the prospective cohort, five patients were lost to follow-up and were thus excluded from the study during the one-year follow-up, with 1,218 TKAs remaining for final analysis. A flow diagram is presented in Figure 1.
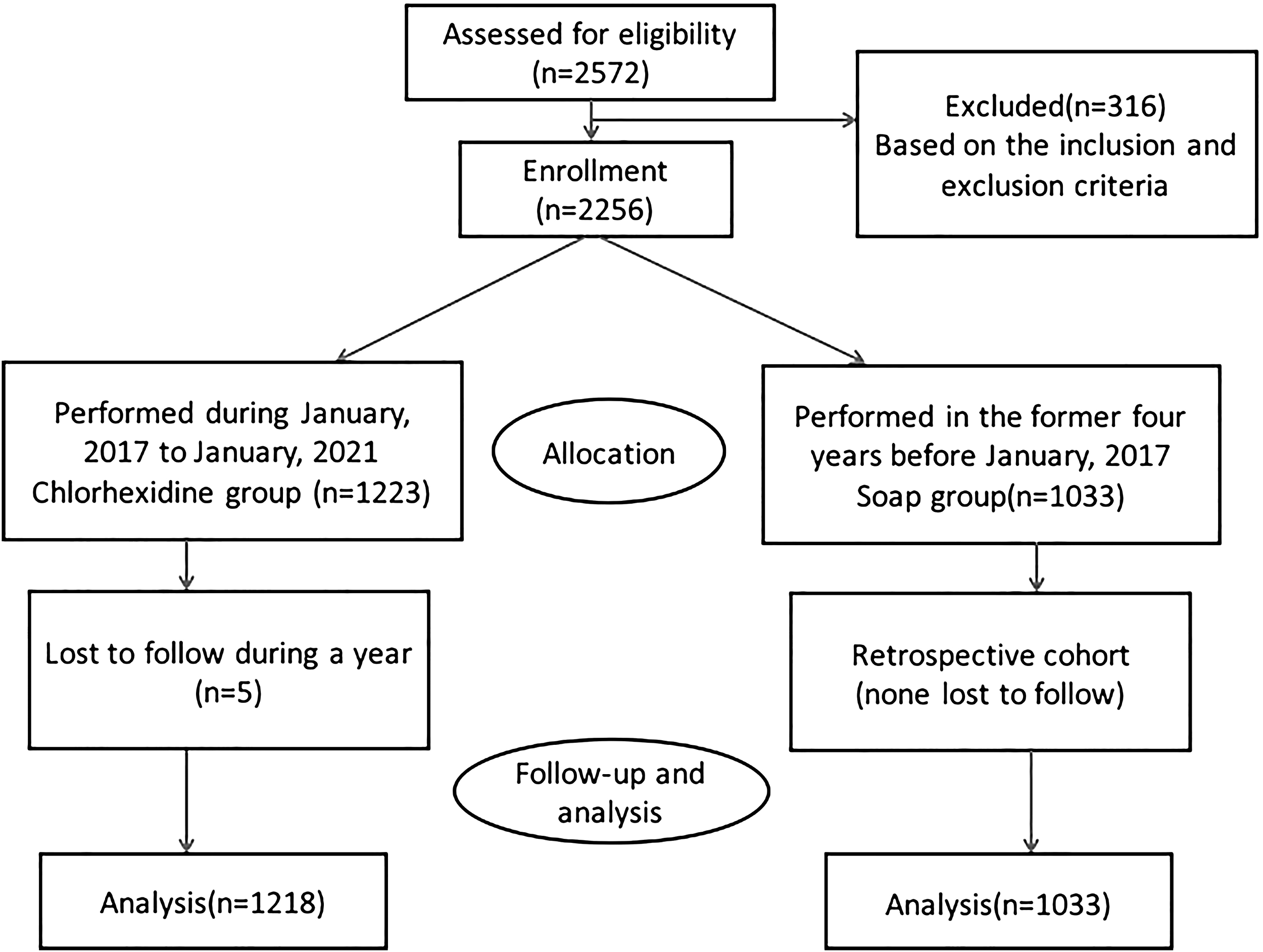
Patient flow diagram.
There were no significant differences in demographic characteristics among the groups in regard to age, gender, body mass index (BMI), operation side, and smoking status; 155 patients with diabetes mellitus were identified in the experimental group and 122 patients in the control group; no significant difference was found between groups. Other parameters such as operation time and blood transfusion cases were similar between groups with no significant differences detected. Detailed data was shown in Table 1.
Patient Demographics
BMI = body mass index.
At a minimum of one-year follow-up, a total of seven (0.6%) PJI cases were detected in the experimental group and 16 (1.5%) cases of PJI were diagnosed in the control group; a significant difference was found between groups (χ2 = 5.245; p = 0.022). Additionally, 18 (1.5%) cases of superficial infection were identified in the experimental group, and a total of 28 (2.7%) cases were observed in the control group; significant difference was detected between groups (χ2 = 4.243; p = 0.039). No significant difference was found for symptomatic deep vein thrombosis (DVT). Regarding the common incision complications, there were 35 (2.9 %) cases identified in the experimental group, and a total of 36 (3.5%) cases were reviewed in the control group without significant difference found between groups (Table 2).
Complications Identified
PJI = peri-prosthetic joint infection; DVT = deep vein thrombosis.
Indicates significant difference.
Discussion
Peri-prosthetic joint infection is a devastating complication after TKA surgery for which the best treatment remains prevention. 20 Many preventive strategies have been attempted to reduce the risks, because the economic burden imposed by such an event might be financially as crippling to the healthcare system as the infection is to the patient's overall lifetime.21,22 In the present study, we found that pre-admission use of chlorhexidine-impregnated gauze for skin preparation the evening before surgery substantially decreases the incidence of PJI and superficial infection after TKA, which has the potential to be used in all patients undergoing TKA surgeries.
Chlorhexidine is currently used routinely as a disinfectant and antiseptic in several healthcare applications because of its broad-spectrum activity and rapid onset of action. 23 Multiple studies have demonstrated its efficacy at decreasing bacterial pathogen load, as well as reducing risk of infection.24,25 It inactivates micro-organisms on the skin surface by the mechanism of its binding to anionic molecules in the bacterial cell wall thus resulting in a rapid death of the organisms. 26 At various concentrations, it is used for skin sterilization, hand hygiene, catheter or wound site dressings, impregnated for disinfection of catheters or surgical meshes, or even added as preservation to cosmetics and other personal care products.27,28 Mostly it has replaced povidone-iodine as a standard-of-care against a variety of micro-organisms yet is safe for healthy soft tissue. 29
The CDC has suggested the inclusion of pre-operative antiseptic agents for skin preparation among other methods in surgical patients for sterilization protocols. 19 Peri-operative 0.12% chlorhexidine gluconate rinses in patients receiving dental implants decreased the infection complications rate to 4.1% versus the incidence of 8.7% in the saline control group. 30 In the study by Schwechter et al., 31 it was demonstrated that scrubbing a methicillin-resistant Staphylococcus aureus (MRSA)-coated titanium disk with chlorhexidine gluconate solution achieved superior biofilm eradication compared with various reagents tested. Although chlorhexidine has proven to be effective with antiseptic properties, there is a lack of evidence in place for the use of pre-operative chlorhexidine-impregnated gauze during TKA procedures for reducing infection risks. A recent meta-analysis 32 examining pre-operative chlorhexidine bathing in TKA procedure found a positive result that the strategy could reduce total incidence of infection and incidence of infection in moderate-risk and high-risk patients. Webster et al. 33 conducted a meta-analysis that found no clear evidence of benefit for pre-operative bathing with chlorhexidine over other products to decrease infections. Therefore, we recruited a large sample to investigate the efficacy of chlorhexidine-impregnated gauze in decreasing infections during TKA procedures. We found a positive result that pre-admission use of chlorhexidine-impregnated gauze substantially decreases the incidence of PJI.
Although a large sample size prospective cohort study with retrospective controls was conducted and accurate data collection was documented as much as possible, limitations still exist to this study. According to the standard practice of our clinic, the study was designed as a prospective cohort study with retrospective controls, which may have introduced bias because of the retrospective nature. Furthermore, various other factors that have been implicated were identified as risk factors for PJI, such as American Society of Anesthesiologists (ASA) grade, socioeconomic status, surgeons' experience, etc., which have not been evaluated in the study that may be the confounding factors. Additionally, the long period of the inclusion may have induced bias because other factors may have been promoted over a six-year period. We cannot control for possible changes to surgeon techniques over time, but it is guaranteed that during this time frame no other changes have been made in institutional protocols regarding the infection control and antibiotic prophylaxis. Even though there are limitations identified in the present study, we tried to conduct a large sample size prospective cohort study with retrospective controls, found that preadmission of chlorhexidine-impregnated gauze for skin preparation significantly decreases the incidence of PJI and superficial infections following TKA procedure. We are looking forward to multicenter prospective randomized controlled trials to further confirm our claims.
Conclusions
Peri-prosthetic joint infections are devastating complications after TKA surgery. The best treatment remains prevention. In the present study, we found that pre-admission use of chlorhexidine-impregnated gauze for skin preparation the evening before surgery substantially decreases the incidence of PJI after TKA. Although future multicenter prospective randomized controlled trials will be required to confirm the preliminary findings, the intervention is inexpensive, unlikely to be risky, and therefore has the potential to be utilized routinely for pre-operative preparation in patients undergoing TKA surgery.
Footnotes
Acknowledgments
We appreciate all the nursing staff of our orthopedic department for helping collect and record the data.
The Ethics Committee of Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine approved the study protocol. Informed consent was obtained from all participants and all methods were carried out in accordance with relevant guidelines and regulations. Written informed consent for publication was obtained from all participants.
Authors' Contributions
Both authors designed the study, accumulated the data, and drafted the manuscript; both authors read and approved the final manuscript.
Data Availability
The dataset supporting the conclusions of this article is available on request. Please contact the corresponding author. This is not an RCT study, so it is no need to register publicly. Administrative permission was received from Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine to access the medical records.
Author Disclosure Statement
The authors declare that they have no conflict of interests.