
Abstract
Background:
Parvovirus B19 (B19V) infection is a rare cause of severe anemia in liver transplant recipients. However, few studies have systematically reviewed reported cases and summarized experience in managing this disease.
Objective:
We described a retrospective case series of eight adult liver transplant recipients with B19V-associated severe anemia and performed a literature review of epidemiology, etiology, clinical courses, diagnosis, treatment options available, and outcomes of B19V-associated anemia in adult liver transplant recipients.
Patients and Methods:
We systematically reviewed articles describing adult liver transplant recipients with B19V-associated anemia from PubMed and ScienceDirect databases from database inception to May 2022.
Results:
Eight articles containing 23 cases were identified in addition to eight cases from our center for a total of 31 patients (mean age, 45.7 ± 9.7 years; 74.2% male). Eighty-seven percent developed transfusion-dependent anemia within two months after liver transplantation (LT). Fever and progressive anemia are among the major manifestations. Intravenous immunoglobulin (IVIG)-based therapy was given to all patients and the treatment protocols varied among different centers. Except for two cases who died of comorbidities, 17 patients obtained long-term recovery from anemia after one course of treatment and six (19%) experienced relapses that were reversed by repeated courses of IVIG therapy. Two recipients presented with IVIG-associated side effects and two developed acute cellular rejection (ACR) after reduction of immunosuppression.
Conclusions:
B19V infection should be suspected early as a cause of severe anemia of unknown etiology in adult liver transplant recipients. The clearance of B19V typically lags behind recovery of anemia, and inadequate clearance of virus after cessation of IVIG appears to be a potential risk of anemia recurrence. Moreover, more attention should be paid to the side effects of high-dose IVIG infusion and ACR because of reduction of immunosuppression.
Post-operative anemia is a common complication of solid organ transplantation (SOT), and aggressive anemia correction in the early post-operative period has been strongly recommended to speed recovery.1–3 However, cases of refractory anemia after SOT have been reported constantly over the past few years, most of which turned out to be correlated with unexpected infection of parvovirus B19 (B19V).4–8 The small DNA virus was initially described in 1974 as a human-pathogenic subgroup of the Parvoviridae family, and virus infection symptoms differ greatly among individuals with different immunologic status.9,10 In immunocompetent individuals, B19V infection causes mild diseases ranging from erythema infectiosum to acute symmetric polyarthropathy, whereas immunocompromised individuals typically present with aforementioned anemia characterized by pure erythroid aplasia, also known as pure red cell aplasia (PRCA). 11
To date, most of the cases with post-transplant B19V-associated anemia reported in the literature are kidney transplant recipients.12–14 Few have been described after liver transplantation (LT). We describe a retrospective case series of eight adult liver transplant recipients who were found to have refractory anemia secondary to B19V infection. Moreover, we also systematically reviewed reported cases of adult liver transplant recipients with B19V-induced anemia and summarized experience in managing this disease.
Case Series
Eight recipients (ages 41–57) who received LT in our center were seen with progressively worsening anemia within two months after LT. Demographics, clinical presentations, treatments, and outcomes are detailed in Table 1; the dynamic courses of hemoglobin (Hb) levels, reticulocyte counts and viremia are illustrated in Figure 1. On review of the pre-operative serologic results, mild to moderate anemia was noted in each case as a result of malnutrition and hypersplenism. Immediately after LT, their Hb levels increased and held steady for at least one week. Consequently, they presented with progressively worsening anemia, which was red blood cell (RBC) transfusion-dependent. The main clinical manifestations included obvious fatigue (7/8), arthralgia (2/8), and moderate fever (1/8). Reticulocyte count (performed in 4 patients) showed varying degrees of reticulocytopenia.
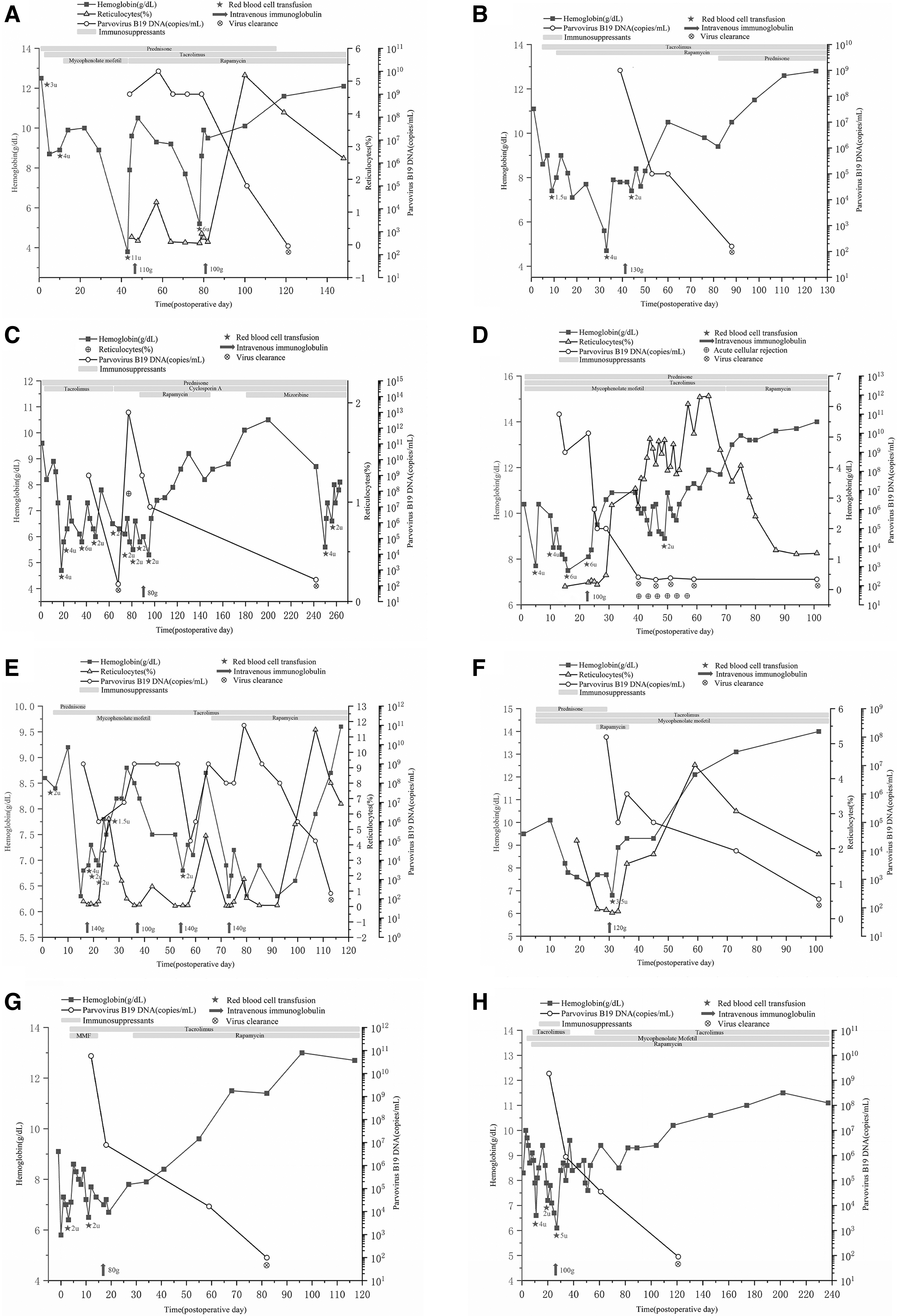
The dynamic courses of hemoglobin levels, reticulocyte counts, and viremia of eight adult liver transplant recipients with parvovirus B19 (B19V)-associated anemia.
Demographics and Clinical Characteristics of Eight Adult Liver Transplant Recipients with B19V-Associated Anemia
B19V = parvovirus B19; F = female; M = male; HCC = hepatocellular carcinoma; HBV = hepatitis B virus; ESRD = end-stage kidney disease; ALF = acute liver failure; LT = liver transplantation; ABO-incompatible LT* = donor AB Rh D positive, recipient B Rh D positive; MVT = multivisceral transplantation (liver, kidney, pancreas, and duodenum); SLKT = simultaneous liver-kidney transplantation; FK = FK506; CsA = cyclosporine A; MMF = mycophenolate mofetil; Co = corticosteroids; RAPA = rapamycin; POD = : post-operative day; IVIG = intravenous immunoglobulin.
Quantitative real-time polymerase chain reaction (qRT-PCR) revealed high levels of B19V DNA (>107 copies/mL) in peripheral blood of all patients. Bone marrow aspirate of one recipient showed selective erythroid hypoplasia with maturation arrest at the proerythroblast stage (Fig. 2). Together with peripheral blood findings and positive B19V serology, as well as exclusion of other etiologies, the diagnosis of pure red cell aplasia (PRCA) caused by B19V infection was established.
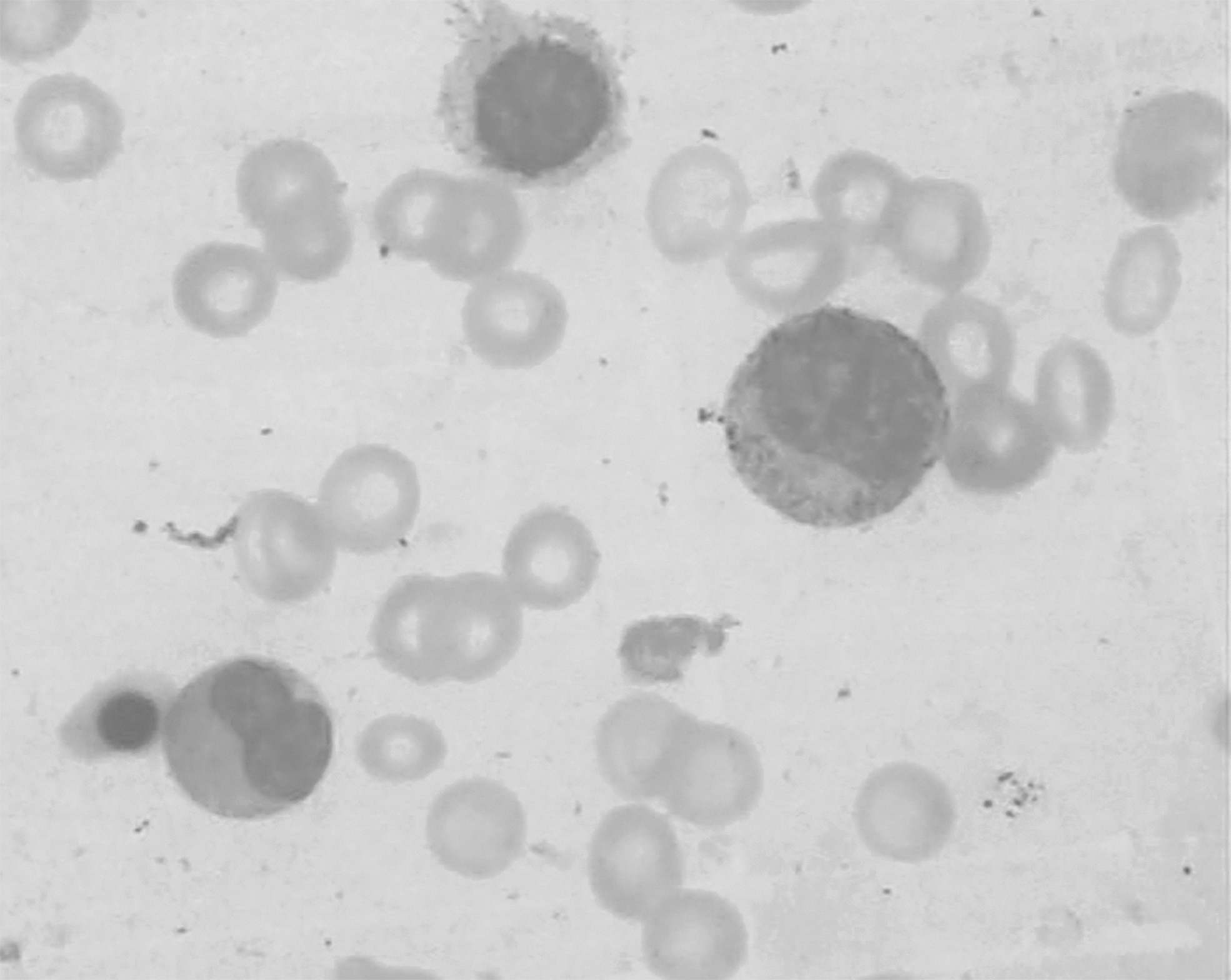
Bone marrow aspirate of one recipient showed selective inhibition of erythropoiesis with scattered giant erythroid precursors.
All eight patients received immediate intravenous immunoglobulin (IVIG) infusions and repeated RBC transfusions, although reduction of immunosuppression was considered in seven patients. The patients received IVIG therapy at the dosage of 0.2–0.4 g/kg/d for four to eight days or 2 g/kg over a period of three to five days. Simultaneous immunosuppression adjustment included dosage reduction of tacrolimus (FK506) or mycophenolate mofetil (MMF), conversion from MMF to mammalian target of rapamycin (mTOR) inhibitor, and switch from FK506 to cyclosporine A (CsA). After the first course of treatment, five patients achieved anemia recovery and viral clearance, whereas three patients experienced relapses (one experienced four relapses in total) requiring repeated IVIG infusions. So far, all recipients have obtained long-term remission of anemia and virus eradication. Notably, one recipient developed mild acute cellular rejection (ACR) confirmed by liver biopsy after reduction of immunosuppression and one presented with hypertension and persistently severe headache refractory to conventional analgesics, which was ultimately cured by diuretics.
Patients and Methods
A systematic search of PubMed and ScienceDirect databases for case reports published in English from database inception to May 2022 was performed using the following MeSH terms: anemia, refractory anemia, liver transplantation, liver transplant, and parvovirus B19. References of the retrieved articles were examined for additional cases. Recipients 18 years of age or older with confirmed B19V-associated anemia and detailed descriptions of clinical courses were included. Recipients with refractory anemia attributed primarily to non-B19V causes (i.e., hemorrhage or hemolysis), pediatric recipients, and adult cases without detailed clinical data were excluded. For each recipient, clinical data including demographics, comorbid conditions, clinical symptoms, immunosuppressive regimens at onset, laboratory findings, therapeutic regimens, and outcomes were collected and analyzed.
Results
Eight articles were identified containing 23 adult liver transplant recipients with B19V-associated anemia. The first case was reported in 1994. Since then, 22 additional cases have been reported to have developed B19V-associated anemia. The main characteristics of the 23 recipients are presented in Table 2.5,12,15–20 The mean age (± standard deviation [SD]) was 45.8 ± 10.9 years. Seven of the 23 patients were female. Eighty-seven percent had FK506-based immunosuppressive regimens at onset. Severe anemia with reticulocytopenia was noticed within two months after LT in most of the cases. The lowest mean hemoglobin level (± SD) was 45.91 ± 11.83 g/L. Fever and progressive anemia including fatigue and paleness were among the major manifestations at onset.
Reported Cases of B19V Infection in Adult Liver Transplant Recipients
B19V = parvovirus B19; F = female; M = male; FK = FK506; CsA = cyclosporine A; AZA = azathioprine; MMF = mycophenolate mofetil; Co = corticoteroids; LT = liver transplantation; Hb = hemoglobin; GP = giant pronomorblasts; P = positive; N = negative; IVIG = intravenous immunoglobulin.
Repeated courses of IVIG therapy led to long-term recovery.
The diagnosis was frequently made by B19V PCR in peripheral blood and by immunohistochemistry in bone marrow biopsy. In cases who were tested for B19V-specific antibodies, one patient was positive for both immunoglobulin M (IgM) and IgG, and six were IgM positive. Bone marrow biopsies of all patients revealed erythroid hypoplasia with presence of giant pronormoblasts. In addition, all patients were positive for B19V PCR in peripheral blood. Except for two cases who died of severe infection and tumor recurrence, respectively, 18 cases obtained long-term recovery from anemia after one course of IVIG-based therapy and three experienced recurrence after the first course of treatment and repeated courses of IVIG therapy led to a complete reversion of B19V-associated PRCA.
Discussion
Liver transplantation is the gold standard treatment for various end-stage liver diseases refractory to medical therapy.21–23 Post-transplant anemia (PTA), a common complication in the early post-operative period, could be attributed to multiple factors including hemorrhage, sepsis, drug, nutritional deficiency, and hemolysis, 24 and aggressive correction of anemia is a crucial means to speed recovery. In recent years, B19V infection has been reported to be a rare cause of severe anemia in liver transplant recipients.5,12,15–20 This study systematically summarized experience in managing B19V-associated anemia after adult LT based on sporadic case reports. In addition, we reported the first case of multivisceral transplant (liver, kidney, pancreas, and duodenum) recipient with B19V-associated anemia and the first simultaneous liver–kidney transplant recipient with B19V-induced anemia.
Parvovirus B19 infection is reported to be common in childhood and approximately one-half of the population is positive for B19V IgG antibody by the age of 15.25,26 Furthermore, healthy blood donors have been found to have circulating B19V DNA in peripheral blood. 27 The epidemiology of B19V infection in SOT recipients remains largely unknown with incidences varying between 0% and 58% across studies. 28 A high-level viremia appears to be associated with severe anemia.28,29 Currently, most of the cases with post-transplant B19V-associated anemia reported in the literature are kidney transplant recipients, the reason for which remains unclear but may be related to their stronger immunosuppression compared with other types of SOT recipients because of a relatively higher risk of rejection for transplanted kidney.30–32
Additionally, it has been found that T-cell responses play a role in anti-B19V immunity, and most of the kidney transplant recipients receive T-cell–depleting antibodies for induction, which may contribute to the increased susceptibility to virus infection. 33 Here, we described B19V-associated severe anemia in adult liver transplant recipients. According to the literature review and analysis of data from our center, viral reactivation with a low-level DNAemia (<105 copies/mL) in liver transplant recipients is not uncommon and may not be clinically significant, while high-level viremia (>106 copies/mL) is typically correlated with destruction of erythrocyte progenitor cells leading to severe PRCA 28 Few studies to date, however, have investigated the incidence of high-level B19V viremia (>106 copies/mL) in non-anemic liver transplant recipients.
Moreover, we observed a higher incidence of B19V-associated PRCA in male recipients (7/8 in our center and 16/23 in the literature review), suggesting that male gender might be a potential risk factor for B19V-associated PRCA in adult LT recipients. However, the specific correlation between them remains elusive because of limited cases reported in the literature. Meanwhile, most of the recipients who received LT in our center were male, which might lead to an inherent bias. Future studies are needed to investigate the epidemiology and risk factors of B19V infection in adult liver transplant recipients.
Our study indicates that B19V-associated anemia generally occurs within two months after surgery in adult liver transplant recipients. Most cases initially complain of fatigue, malaise, and arthralgia, although moderate fever is observed in a small proportion of patients. The diagnosis of B19V-associated anemia primarily relies on the detection of viral DNA by PCR in peripheral blood or bone marrow specimens and by immunohistochemistry in bone marrow biopsy. However, a positive PCR for B19V DNA does not always indicate acute infection or warrant immediate clinical intervention in that recipients with ongoing, low-level viremia (<105 copies/mL) are normally asymptomatic and persistent low-grade DNAemia (<105 copies/mL) may last for months despite adequate clinical response to IVIG-based therapy. 28 Conversely, a higher viral load (>106 copies/mL) is more likely to be associated with symptomatic disease (i.e., B19V-associated PRCA). In our study, the viral load of B19V in peripheral blood at onset is elevated (all above 107 copies/mL).
Currently, no specific qPCR threshold with clinical significance is available. Moreover, according to the American Society of Transplantation Infectious Diseases Community of Practice guidelines for B19V infection in SOT recipients, timely intervention is recommended for SOT recipients with symptomatic B19V infection. 28 As a result, it is not qPCR assay, which is generally used for the diagnosis of B19V infection, but obvious clinical symptoms (i.e., progressively worsening anemia) that determine immediate clinical intervention in most cases. Bone marrow biopsy is another reliable method for the diagnosis of B19V-associated anemia, which is typically characterized by selective inhibition of erythropoiesis with scattered giant erythroid precursors. Actually, only a few patients are willing to undergo this invasive procedure. Hence, bone marrow biopsy is not included in the initial work-up for suspected B19V-associated anemia in SOT recipients. The American Society of Transplantation Infectious Diseases Community of Practice recommended that bone marrow examination be performed when B19V infection is strongly suspected (i.e., developed refractory anemia with inappropriate reticulocyte response, fever, arthralgia, or rash), although the serology and serum PCR are negative. 28
Accordingly, bone marrow biopsy is necessary to establish the diagnosis of B19V-associated anemia for SOT recipients with unexplained anemia and low-level viremia prior to offering IVIG therapy or reduced immunosuppression. Besides, the red blood cells in peripheral blood remain normocytic and normochromic in most cases. Because of an insufficient antibody response in immunocompromised patients, the serologic detection of B19V IgM and IgG is not always contributory. It's worth noting that B19V-associated anemia in LT recipients may be easily ignored in the early post-operative period because these recipients are typically complicated with chronic anemia due to hypersplenism and long-term malnutrition.
The specific mechanism of B19V infection remains unclear. According to literature reports, the glycosphingolipid (GSL) globoside (Gb4), also known as P-antigen receptor, is essential for parvovirus B19 (B19V) infection.34,35 This receptor is mainly expressed in human erythroid progenitor cells in the bone marrow, and thus virus invasion typically lead to PRCA. Moreover, α5β1 integrin and the Ku80 autoantigen were described as coreceptors for B19V infection.36,37 Additional research is needed to elucidate the pathogenic mechanisms of B19V.
Post-transplant B19V infection is mostly related to transmission via respiratory droplets and viral reactivation under immunosuppression. 12 In our case series, most of the recipients received triple immunosuppressive therapy, which may lead to B19V re-activation. Moreover, viral transmission through the respiratory tract should also be taken into consideration in that two recipients in our study shared the same room at onset. Hence, immediate isolation of infected individuals is necessary in transplant wards. Besides, previous studies have shown that transmission of B19V infection may derive from blood transfusions and donated organs.38,39 We did not test the donors for B19V infection prior to LT, so we could not exclude donor-derived transmission, which was a disadvantage of our study.
Although spontaneous recovery from B19V-associated anemia has been reported in some SOT recipients, which is possibly due to an absence of B19V P-antigen receptor, 6 early diagnosis and timely clinical intervention are still recommended. 28 To date, no specific therapy is available to treat B19V-associated PRCA in SOT recipients. Empirical strategies include high-dose IVIG infusion, reduction of immunosuppression, red blood cell transfusion, and iron/folic acid supplementation.40,41 In this study, all recipients received at least one course of IVIG-based therapy, underscoring the significance of IVIG infusion in reversing B19V-associated PRCA. The recommended dosage of IVIG varies between different transplant centers from 0.4 g/kg/d for five days to 2 g/kg for three days.42,43
Our results showed that high-dose IVIG therapy could terminate PRCA and inhibit virus replication, whereas insufficient dose might lead to inadequate clearance of virus and anemia recurrence. However, more attention should be paid to the side effects of high-dose IVIG administration. 44 In our study, two recipients presented with IVIG-associated side effects such as hypertension, headache, arthralgia, and renal failure during the course of IVIG therapy.
Post-transplant PRCA is induced either by immunosuppressive agents or PVB19 infection. 17 As a consequence, appropriate readjustment of immunosuppressive regimen is also of great importance to reverse B19V-associated PRCA. However, reduction of immunosuppression holds a risk for post-transplant graft rejection. In our study, two recipients developed ACR confirmed by liver biopsy after reduction of immunosuppression, which further complicated their conditions. Therefore, individualized risk assessment is imperative to prevent potential rejection.
According to literature reports, the recurrence rate of B19V-associated anemia in SOT recipients was 10%. 45 In this study, 22% (7/31) of the recipients experienced relapses. We observed that the clearance of B19V appeared to lag behind recovery of anemia, and inadequate clearance of virus after cessation of IVIG might represent a potential risk of anemia recurrence, which still necessitated periodic follow-up. Based on the literature review and our experience, repeated courses of IVIG infusion are recommended to reverse recurrence of viraemia and PRCA. 12
Conclusions
Parvovirus B19 infection is a rare cause of severe anemia in SOT recipients, which is likely to be overlooked and underdiagnosed. The objective of this study is to draw attention to the early diagnosis and timely clinical intervention of B19V infection in liver transplant recipients. Further studies are needed to develop more effective preventive and therapeutic strategies.
Footnotes
Authors' Contributions
Pengrui Cheng and Yi Ma conceptualized this work. Pengrui Cheng contributed to data collection of case series. Qian Jian and Zongli Fu performed the literature review. Pengrui Cheng drafted the first version of the manuscript. All authors reviewed and edited subsequent versions of the manuscript.
Funding Information
This study was supported by grants from National Natural Science Foundation of China, China (81873591 and 81670591), Natural Science Foundation of Guangdong Province, China (2016A030311028), The Science and Technology Planning Project of Guangdong Province, China (2018A050506030), and The Science and Technology Program of Guangzhou, China (201704020073). The Guangdong Provincial Key Laboratory Construction Projection on Organ Donation and Transplant Immunology (2013A061401007, 2017B030314018, and 2020B1212060026), Guangdong Provincial International Cooperation Base of Science and Technology (Organ Transplantation) (2015B050501002 and 2020A0505020003).
Author Disclosure Statement
No conflicts of interest are reported for any author.