
Abstract

To the Editor:
Radiographic imaging has revolutionized the evaluation and diagnosis of hollow viscous perforation. 1 Physician assessment and judgment remains vital for correlation in the clinical setting. We present a case illustrating the importance of physician judgment in the setting of a confusing clinical presentation.
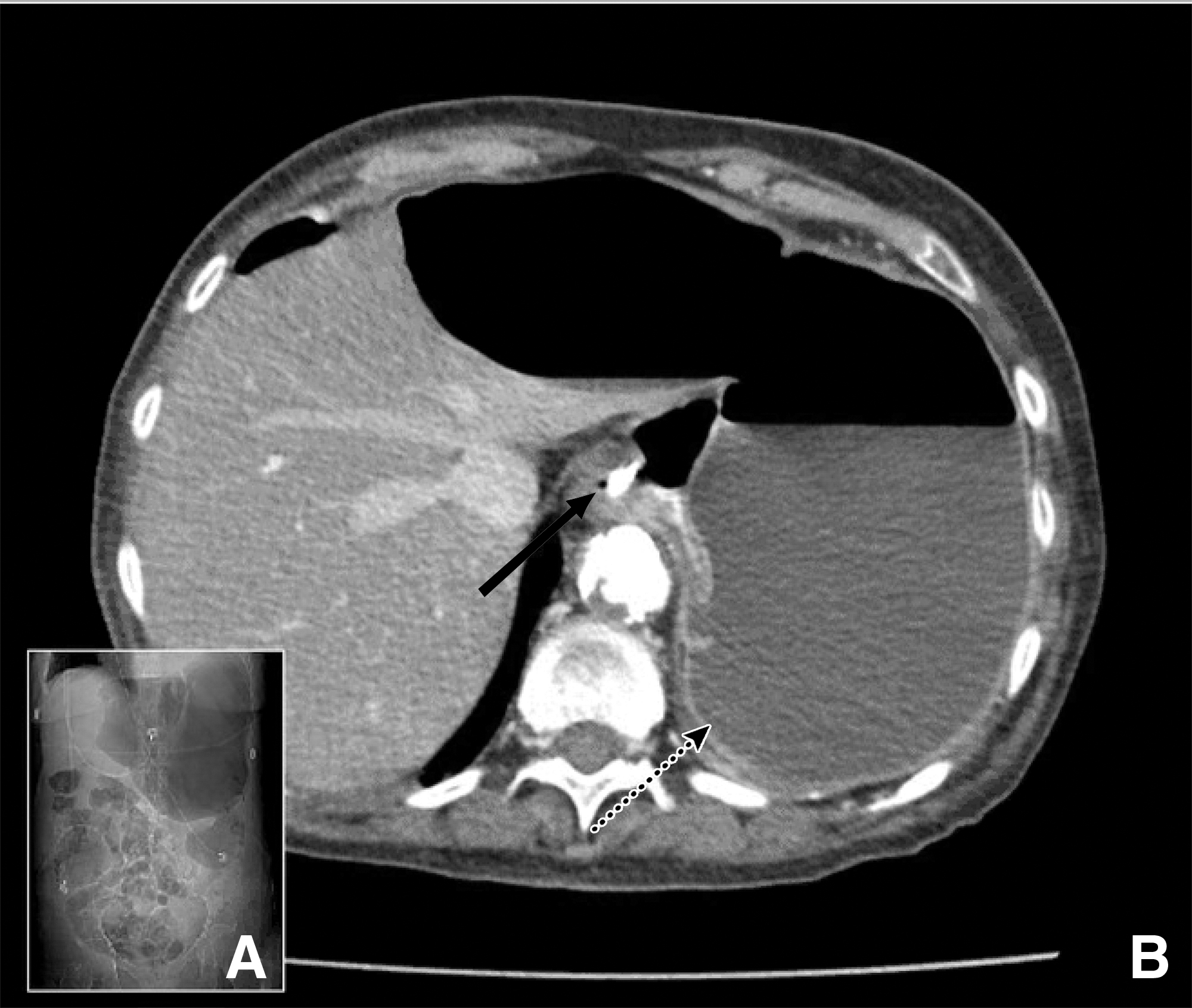
A 74-year-old female presented with one week of abdominal pain. Pertinent history included chronic obstructive pulmonary disease (COPD), recently medically treated non-ST segment elevation myocardial infarction (NSTEMI) with associated new systolic heart failure (ejection fraction, 30%), and Graham patch repair for perforated duodenal ulcer two years prior to presentation. Vitals were normal, abdomen without signs of peritonitis, and laboratory tests were notable for white blood cell (WBC) count of 21,000/μL. A computed tomography (CT) abdomen/pelvis without contrast suggested large gastric distention (Fig. 1). The working diagnosis was peptic ulcer disease causing gastric outlet obstruction. A nasogastric tube (NGT) was placed; proton pump inhibitors and broad-spectrum antibiotics were started. Nasogastric tube output was low, and a follow-up abdominal radiograph showed continued “gastric” distention despite adequate NGT position. High suspicion for an alternate diagnosis led to a repeat CT of the abdomen/pelvis with intravenous and oral contrast, which identified the cavity as a large abscess secondary to perforated sigmoid diverticulitis. The multidisciplinary team discussed risks and benefits of surgery with the patient, and a decision was made to pursue non-operative management and comfort measures. A CT-guided drain was placed, and antibiotic agents were narrowed according to cultures. The patient was discharged home with hospice and died two weeks later.
The use of diagnostic cross-sectional imaging has increased dramatically over the past two decades and has become an integral part of the diagnostic process. 2 However, this case highlights the importance of clinical assessment where physician evaluation remained vital in directing the diagnostic workup and making the final diagnosis. This is essential when the diagnosis is ambiguous and imaging and clinical assessments are discordant. This is particularly important as outcomes can be detrimental to patients if the management offered does not align with the disease process.
Finally, surgical intervention is often recommended in patients with intra-abdominal abscess and pneumoperitoneum. 3 Unfortunately, geriatric patients with multiple comorbidities who develop emergency general surgical conditions often have worse baseline health and functional status and are at risk for poor outcomes. 4 Offering operative intervention can be fatal to these high-risk patients, and palliative care measures are frequently underutilized. 5
Discussing goals of care with the patient is imperative and non-operative measures can be offered when aligned with a patient's goals and priorities. For patients who are extremely high risk for operative interventions, non-operative management strategies may allow a patient to maintain mental status and spend quality time with loved ones prior to death.