
Abstract

To the Editor:
I
A six-year-old girl presented with paroxysmal abdominal pain after swallowing a toothpick. She was treated with antibiotic agents at the local hospital and discharged with improved abdominal pain. Ten days later, a mass appeared on the child's navel. The mass was gradually enlarged and slightly elevated to the skin surface, which was firm and weak in texture, with poor mobility and tenderness. There was no swelling, rupture, or ulceration on the skin surface. She had slight abdominal pain with no fever or vomiting. She reported to our hospital for further evaluation and treatment.
A thin hyperechoic mass measuring approximately 5 cm was seen on ultrasound, one end in the muscular layer of the abdominal wall and the other end in the ascending bowel (Fig. 1). An abscess was formed around the outside part of the bowel (Fig. 2). The diagnosis of gastrointestinal foreign body and intestinal perforation was considered, and open surgery was performed immediately. During the operation, extensive adhesion of intestinal tube and omentum to the abdominal wall around the umbilical region was observed, resulting in incomplete intestinal obstruction. One end of the toothpick was located in the ascending colon and the other in abdominal muscle layer (Fig. 3). The toothpick was removed, and the ascending colon repaired. The patient recovered without complications.
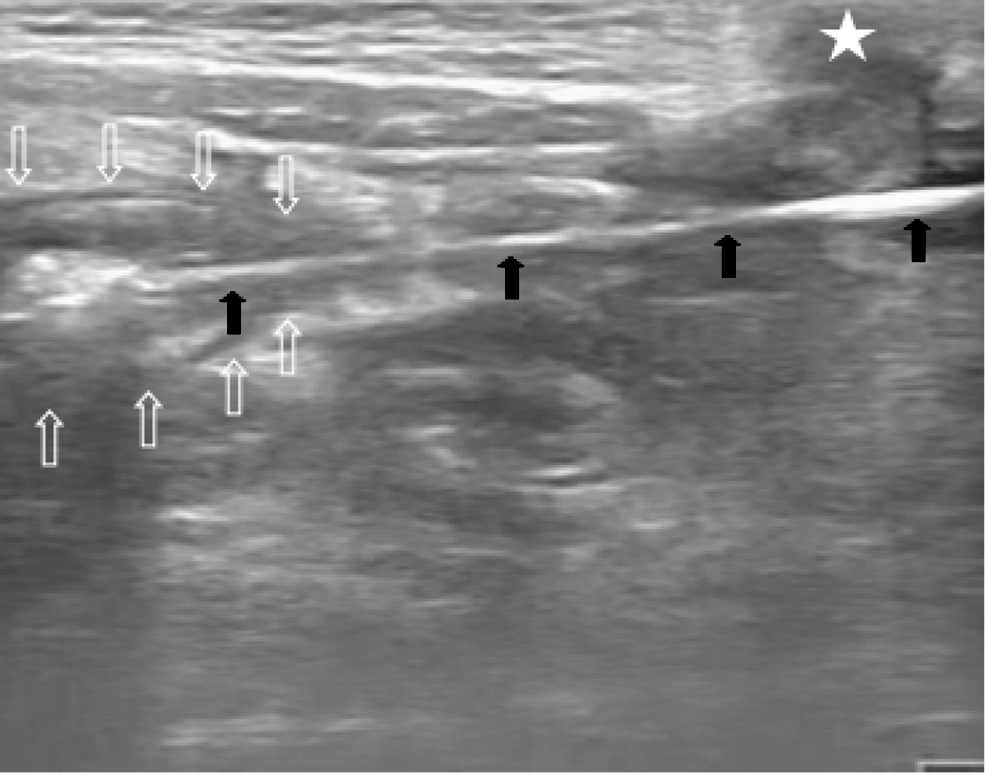
Ultrasound examination of the abdomen. A toothpick (black arrows) was observed in the abdomen, with one end located in the bowel (white arrows) and the other end in the muscular layer of the abdominal wall (arrowhead) next to the navel (star).

Ultrasonic examination of abdomen. An abscess (arrowhead) was formed around the toothpick (black arrows) in the rectus abdominis muscle layer around the navel (star).
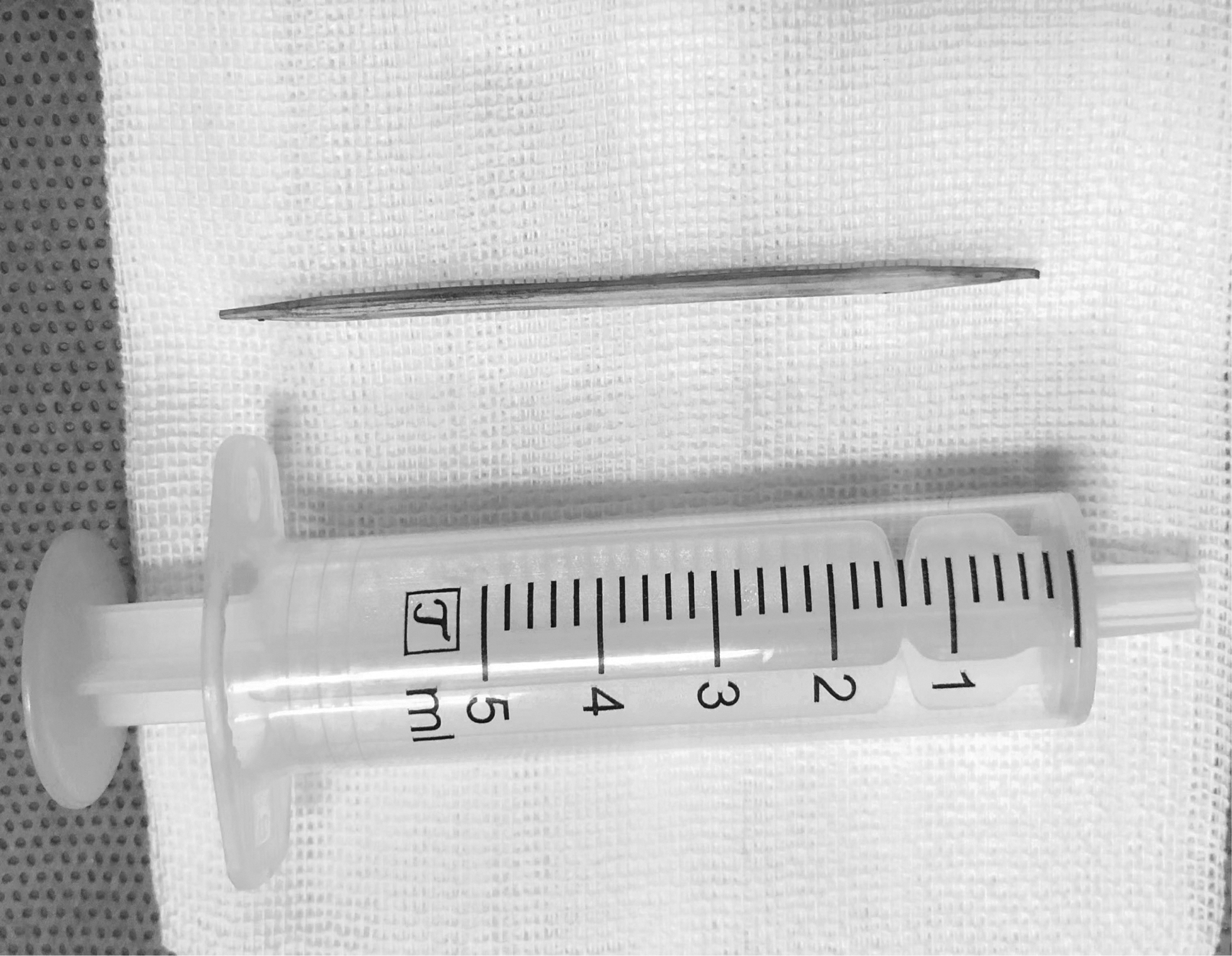
Surgical specimen. A toothpick measuring approximately 6 cm was removed during the operation.
Young children tend to try to understand surrounding objects by tasting and swallowing them. Toothpicks, which were once used as a tool to clean teeth, are now often used as kitchen utensils, thus increasing the risk of accidental ingestion. Studies have shown that only 12% of patients in studies remember that they had swallowed a toothpick,1,2 and most still cannot remember swallowing a toothpick after a definite diagnosis of toothpick ingestion. Non-specific symptoms such as abdominal pain and malignancy can occur less than one day to 15 years after the event.3,4 After swallowing toothpicks, young children cannot express themselves clearly or may hide their illness for fear of being reprimanded. Many sharp-pointed objects are not visible radiographically, therefore, a diagnosis of a gastrointestinal toothpick is difficult. Ultrasound is not affected by the physical characteristics of the foreign body, and it can be scanned from multiple angles. It can also be used to find foreign bodies during surgery. The abdominal wall and bowel wall in children are thin, the display is also clearer. Compared with computed tomography (CT), ultrasound has the advantages of no radiation, low cost, and strong repeatability. Therefore, ultrasound has a good applicability for foreign bodies in children.
Toothpicks, especially double-headed, sharp toothpicks, have a high risk of perforation. It is helpful to make a reasonable diagnosis and treatment for patients by choosing endoscopy, CT, nuclear magnetic resonance, or ultrasound examination according to the possible location of foreign bodies. Ultrasound has advantages in the monitoring of pediatric patients. Antibiotics should be used with caution to avoid obscuring the condition.