
Abstract
Background:
Exploration of the risk factors of recurrent appendiceal abscess after initial non-surgical treatment without drainage in children with appendiceal abscess.
Patients and Methods:
The medical records of all children diagnosed with appendiceal abscess and who were treated conservatively in the Children's Hospital of Chongqing Medical University from June 2012 to June 2020 were collected. The collected cases were divided into the recurrent group and the non-recurrent group, and all clinical indicators were compared. Logistic regression analysis was used to determine the risk factors for recurrent appendiceal abscess in children.
Results:
One hundred twenty-four patients were included and among them, 62 (50.0%) had clinical manifestations of recurrent appendiceal abscess (the recurrent group) and five patients (8%) suffered several instances of recurrence. Duration of intravenous antibiotic agents (odds ratio [OR], 0.905; 95% confidence interval [CI], 0.820–1.000) was independently associated with the recurrence of appendiceal abscess. The risk of recurrence was increased in children with the white blood cell (WBC) count at discharge greater than 8 × 109/L (OR, 2.702; 95% CI,1.172–6.231), the ratio of mass size to body surface area (BSA) at discharge greater than 4.255 (OR, 1.369; 95% CI, 1.104–1.697), and without continuous oral antibiotic agents after discharge (OR, 3.111; 95% CI, 1.240–7. 802).
Conclusions:
Interval appendectomy is recommended for children with WBC count at discharge greater than 8 × 109/L, and the ratio of mass size to BSA at discharge greater than 4.255, because they are more likely to develop recurrent appendiceal abscess after initial conservative treatment. The duration of intravenous antibiotic agents is an independent factor of the recurrence of appendiceal abscess, and a longer course of intravenous antibiotic agents is strongly associated with a reduced risk of recurrence. Continued oral antibiotic agents after discharge can effectively reduce the risk of recurrence of appendiceal abscesses.
Appendiceal abscess is one of the common complications in pediatric general surgery. It is mainly caused by the delayed diagnosis or treatment of acute appendicitis, which leads to appendiceal gangrene perforation. Subsequently the appendix is wrapped by greater omentum, accounting for 4% to 10% of acute appendicitis.1,2 With the development of imaging and ultrasound, the diagnosis of appendiceal abscess is relatively easy, but the treatment remains controversial. Initial surgical treatment of appendiceal abscess is usually considered with complications, so conservative management has become the well-accepted treatment, including antibiotic agents alone or percutaneous drainage of abscesses in combination with antibiotic agents. After successful initial conservative treatment, most clinicians choose interval appendectomy to prevent recurrent appendiceal abscess. However, some believe that the recurrence rate after successful conservative treatment of appendiceal abscess is low, about 5%.3,4 Therefore, it is debatable whether it is necessary to perform interval appendectomy.
Research has shown that the recurrence rate is related to certain factors.5–8 Thus, this study aims to explore the relation between various risk factors and the risk of recurrence, to improve the predictability of the recurrence of appendiceal abscesses, and to implement interval appendectomy more specifically.
Patients and Methods
A retrospective single-center study was conducted on children admitted to the Children's Hospital affiliated with Chongqing Medical University.
Eligible population
From June 2012 through June 2020, all children diagnosed with appendiceal abscess and treated conservatively were included in the study. Cases with incomplete medical records, cases with other malignant diseases, or cases with conservative treatment failure were excluded from the study. Recurrence was defined as those children with re-occurrence of abdominal pain and signs of fixed right-lower quadrant tenderness and rebound pain, with an ultrasonographic image of hypoechoic or anechoic area in the right-lower quadrant of the abdomen. Among the collected cases, all children who were hospitalized for the second time or multiple times because of recurrence of appendiceal abscess were included in the recurrent group. All children who did not develop manifestation of recurrent appendiceal abscess during the study period were considered to have no recurrence, and they were all included in the non-recurrent group. The criteria for discharge were remaining afebrile for 48 hours, improvement of abdominal signs and symptoms, and decreasing white blood cell (WBC) count and C-reactive protein (CRP) levels.
Treatment
An antibiotic regimen was prescribed when children were admitted with stable vital signs and a well-defined abscess in the right-lower quadrant of the abdomen on ultrasound imaging, and without clinical manifestation of septic shock, diffuse peritonitis, intestinal perforation, intestinal necrosis, etc. The selected antibiotic regimen was two combinations (ceftizoxime sodium and metronidazole or ampicillin sodium and metronidazole) or three combinations (ceftizoxime sodium, ampicillin sodium, and metronidazole) that was prescribed according to the clinicians' assessment based on the children's general condition and abdominal signs. Other general treatment included fasting, re-hydration, gastrointestinal decompression if necessary, maintaining water and electrolyte balance, and paying attention to abdominal symptoms and signs. Surgery should be performed as soon as symptoms and signs become severe after 48-hour antibiotic agent administration. We prescribed cefixime granule as oral antibiotic agent after discharge with a dosage of 100 mg (weight ≥30 kg) or 1.5–3 mg/kg (weight <30 kg), twice per day, for a week.
Statistical analysis
Statistical analysis was performed by using SPSS Statistics, version 25 (IBM Corp, Armonk, NY). All continuous variables were tested by the Kolmogorov-Smirnov test. Those conforming to the normal distribution were described with mean ± standard deviation; otherwise, the median (range) was used. The t-test or Wilcoxon test were used to compare continuous data between the groups. To compare categorical data, χ 2 or the Fisher exact test were performed when appropriate. Then, all the above indicators were analyzed with logistic regression analysis, and the independent risking factors of recurrence were observed. GraphPad Prism 8.0 (GraphPad Software, Inc., San Diego, CA) was used to make the receiver operating characteristic (ROC) curve to obtain the cutoff value. A p value <0.05 was significant. This study does not include any intervention in human subjects, and therefore ethical approval was not required.
Results
Among 124 children who met the study criteria, 62 children (50.0%) in the recurrent group had re-occurrence of clinical manifestations of appendiceal abscess and five patients (8%) suffered several instances of recurrence. There were no deaths in our study and all cases were treated successfully non-surgically. Table 1 shows the difference of all descriptive indicators, among which, age (3.75 vs. 5.3 years), length of stay (10 vs. 13 days), intravenous antibiotic agent duration (9 vs. 13 days), CRP at discharge (8 vs. 8 mg/L), size of mass at discharge (2.80 vs. 2.15 cm), proportion of abscess reduction (45.5% vs. 59%), and no oral antibiotic agents after discharge (42.9% vs. 19.4%) were significantly different. In addition, there was significant difference in the WBC count at discharge between groups (8.645 vs. 6.685 × 109/L; p < 0.001), but not in the WBC count at admission (17.04 vs. 17.225 × 109/L; p = 0.845). Thus, we made the ROC curve for the WBC count at discharge and determined the cutoff value of 8.0 × 109/L.
Clinical Data between the Recurrent Group and Non-Recurrent Group
WBC = white blood cell; CRP = C-reaction protein; BSA = body surface area; NEUT% = neutrophil.
p < 0.05.
Our results showed that there were 37 patients in the recurrent group whose WBC count at discharge was over 8.0 × 109/L, which was more than that in the non-recurrent group (17 patients; p < 0.001). Our study found that the size of mass at discharge in the recurrent group was higher than that in the non-recurrent group (2.80 vs. 2.15 cm; p = 0.003). However, different sizes of mass have different effects on children with different BSA. Therefore, we analyzed statistically the ratio of mass size to BSA at discharge; the results are shown in Figure 1. The ratio of mass size to BSA at discharge in the recurrent group was than that in the non-recurrent group (4.01 vs. 2.875; p < 0.001).
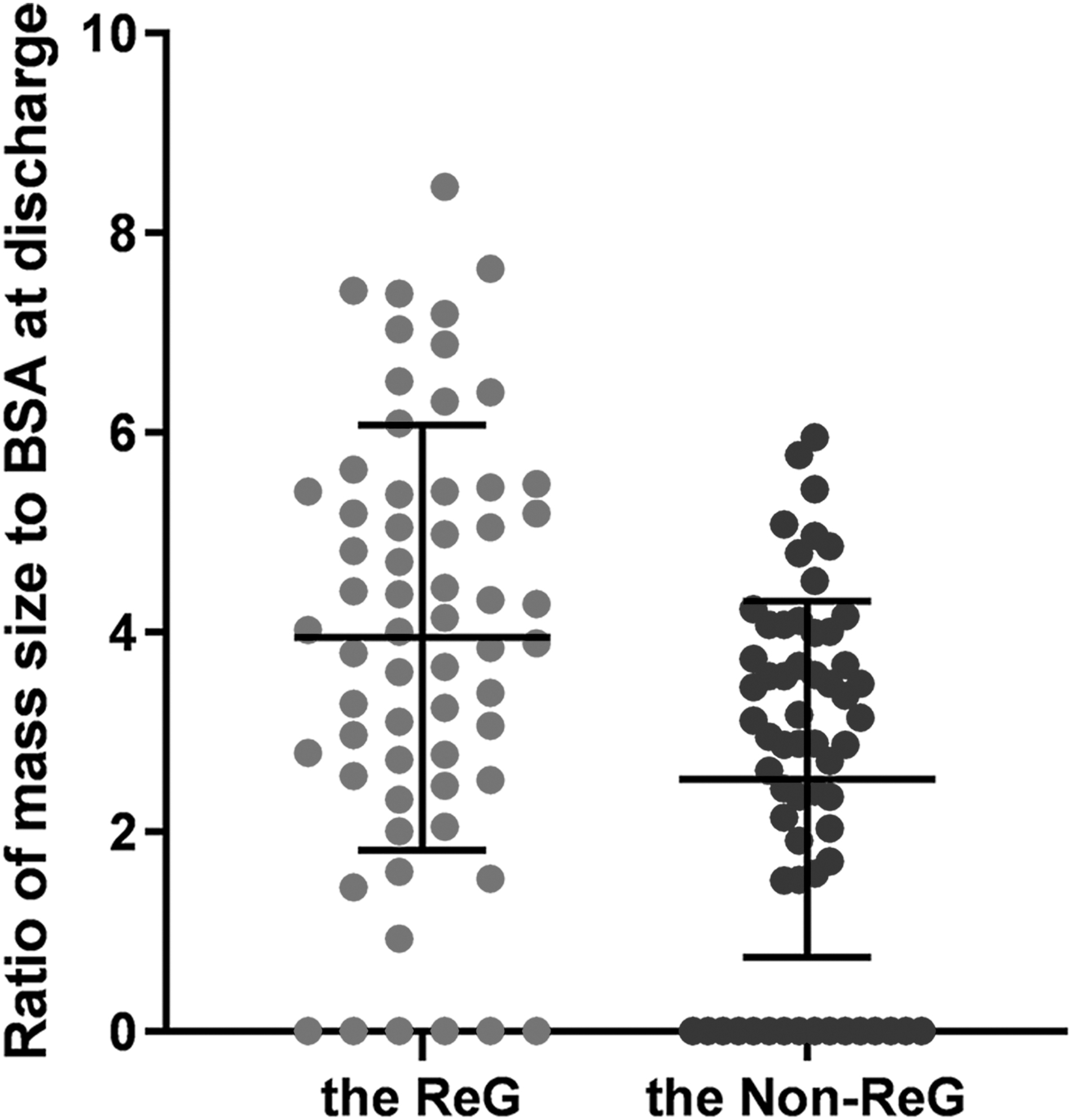
The ratio of mass size to body surface area (BSA) at discharge between groups. The ratio of mass size to BSA at discharge in the recurrent group (ReG; 4.01) was higher than that in the non-recurrent group (Non-ReG; 2.875; p = 0.000).
Table 2 shows the result of logistics regression analysis for all the clinical indicators in Table 1. Duration of intravenous antibiotic agents (odds ratio [OR], 0.905; 95% confidence interval [CI], 0.820–1.000) was independently associated with the recurrence of appendiceal abscess. Also, the duration of antibiotic agents in the recurrent group was lower than that in the non-recurrent group (9 vs. 13 days; p < 0.001). GraphPad Prism 8.0 was used to make ROC curves for ratio of mass size to BSA at discharge (Fig. 2). The results showed that the cutoff value for the ratio of mass size to BSA at discharge was 4.255 (area under the curve [AUC], 0.6908; sensitivity, 46.77%; specificity, 87.1%). These results may imply that the risk of recurrence for the children with the ratio of mass size to BSA at discharge greater than 4.255 (OR, 1.369; 95% CI, 1.104–1.697), or without continued oral antibiotic agents after discharge (OR, 3.217; 95% CI, 1.291–8.019) was increased.
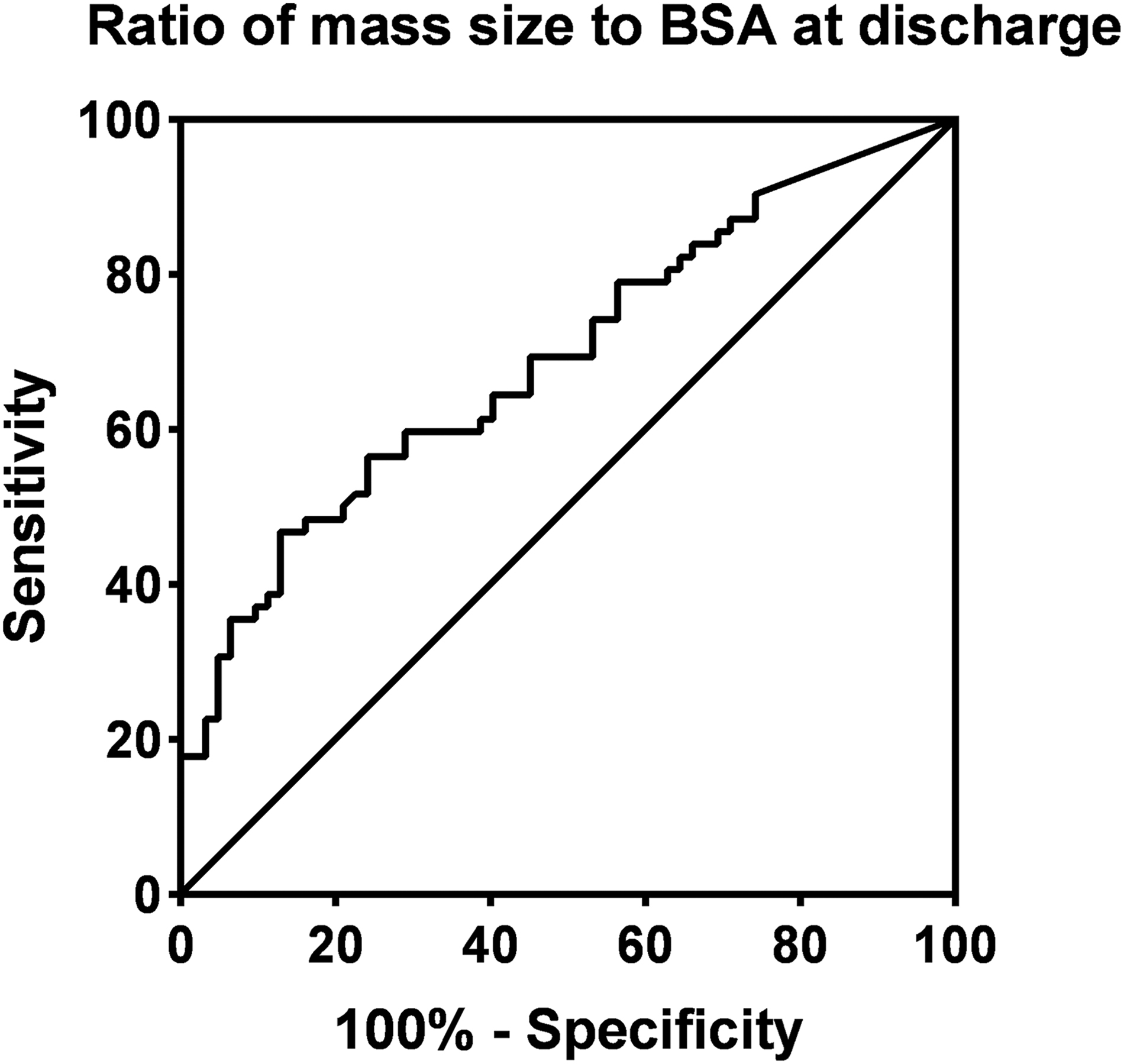
The receiver operating characteristic (ROC) curves for ratio of mass size to body surface area (BSA) at discharge (area under the curve [AUC], 0.6908; cutoff value 4.255; sensitivity, 46.77% specificity, 87.1%).
Odds Ratio Value for the Risk Factors of Recurrence
WBC = white blood cell; CRP = C-reaction protein; BSA = body surface area; OR = odds ratio; CI = confidence interval.
p < 0.05.
In addition, by comparing the features between the first admission and the re-admission because of the recurrence of appendiceal abscess (Table 3), we found that the WBC count at admission (17.28 ± 4.99 vs. 12.59 ± 5.14 × 109/L; p < 0.001), CRP (61.5 vs. 12.5 mg/L; p < 0.001), and size of mass (5.48 ± 1.78 vs. 3.14 ± 1.81 cm; p < 0.001) were lower at re-admission than those at the first admission. All the recurrent cases were managed with conservative treatment.
Clinical Data between the First Admission and Re-Admission
WBC = white blood cell; NEUT = neutrophil; CRP = C-reaction protein.
p < 0.05.
Discussion
Acute appendicitis is a major cause of childhood morbidity and the most common surgical emergency in children, of whom approximately 4%–10% have already formed appendiceal abscess at admission.1,2 Because of the distorted structures around the appendix and the heavily adjacent tissues, urgent appendectomy is often considered with many complications, such as residual abscess, intestinal obstruction, and incision infection.9–11 On the contrary, the conservative treatment of appendiceal abscess is currently considered safe and effective. 12 This may be because the operation at the peak of the inflammatory process of appendicitis causes the overactivation of cytokine cascade, whereas conservative treatment can limit the inflammatory response and provide time for the recovery of intestine.13,14
With the improvement of ultrasound technology, many believe that ultrasound-guided percutaneous drainage of abscesses should be performed early under the co-guidance of clinicians and sonographers after the formation of appendiceal abscess. A study conducted by Luo et al. 15 divided 1,225 patients into an antibiotic agent only group and percutaneous drainage with antibiotic agents group, and the results showed that the interval appendectomy rate, the recurrence rate of appendicitis, and the incidence of complications after interval appendectomy in the percutaneous drainage with antibiotic agents group were all decreased. Zhang et al. 16 believes that patients treated with percutaneous drainage have a better prognosis and a lower incidence of complications, but not all patients are suitable for drainage. Percutaneous drainage is recommended only when the abscess is single, large-volume, and with puncture path. It is controversial when the abscesses are multiple, small volume, and separated because of the possibilities of multi-punctures and insufficient drainage. 16 In our tertiary hospital, the National Children's Regional Medical Center of Southwest China, we believe that the intestines may be injured during the puncture process because of the heavy abdominal adhesion after the formation of an appendiceal abscess. In addition, the abscess with irregular shape or separation may have poor drainage, and multiple punctures are needed. Moreover, young patients cannot cooperate with the puncture treatment and the treatment needs to be carried out under general anesthesia, which adds the risk of anesthesia. Therefore, we conclude that the indications should be strictly selected when percutaneous drainage of abscess is taken.
The pathogenic bacteria are mostly anaerobic cocci, Escherichia coli, and Enterococcus,17–20 so we chose metronidazole combined with penicillin and cephalosporin for treatment. Clinicians choose the antibiotic agent regimen according to the abdominal signs and the children's condition. Under the circumstances of the same discharging criteria, we found that there was no difference in the kinds of antibiotic agents between the groups. A possible reason may be that most children's condition was relatively severe at admission, and triple combinations of antibiotic agents were mostly prescribed (85.5% vs. 88.7%; p = 0.592). There may exist inevitable bias caused by the selection of antibiotic agent combinations. However, our findings suggest that a longer course of intravenous antibiotic agents was strongly associated with a reduced risk of recurrence. Cefixime granule was prescribed as oral antibiotic agents after discharge for a week, which was considered as a prolongation of the duration of intravenous antibiotic agents. This may further clarify that the antibiotic agent course was an independent factor of the recurrence of appendiceal abscess. Some studies have pointed out that resistance is a natural biologic outcome of antibiotic use and antibiotic overtreatment increases the speed of antimicrobial resistance. The use of antibiotic agents should be minimized wherever possible.21,22 Therefore, the course of antibiotic agents should be decided discreetly. Unfortunately, our research was not able to determine the optimal antibiotic agent duration, because clinicians made the decision based on their clinical experiences. Therefore, we need more prospective trials to focus more on the antibiotic agent regimen and determine the optimal timing.
Studies have revealed that appendicolith is an independent risk factor for the recurrent appendiceal abscess,5–7 but we found that there was no difference in appendicolith between groups (37.1% vs. 27.6%; p = 0.077). Zhang et al. 23 believed that after successful conservative treatment of appendiceal abscess with appendicolith, most appendicolith could be absorbed, whereas the persistence of appendicolith may increase the risk of recurrence of appendiceal abscesses. As our study failed to follow up the dissolution of appendicolith in the non-recurrent group, the persistence of appendicolith between groups could not be compared.
Further studies are needed to confirm the relation between appendicolith and recurrent appendiceal abscess. Furthermore, we analyzed the clinical data between the first admission and the re-admission because of the recurrence of appendiceal abscess and found that children suffered a lighter attack when appendiceal abscess recurred. This may be because of parents' increased alertness and in-time hospitalization after the experience of first admission. 8 This also supports the continued non-surgical regimen for children with recurrent appendiceal abscess.
Some research revealed that the WBC count and abscess size were strongly associated with the recurrence of the appendiceal abscess, which is consistent with our study.24–27 Nazarey et al. 25 found that a WBC count >15.0 × 109/L was associated with increased recurrence rate of appendiceal abscesses. We analyzed the WBC at discharge with the cutoff value of 8.0 × 109/L, and the results of logistic regression analysis showed that the WBC at discharge >8.0 × 109/L was an independent risk factor for the recurrence of appendiceal abscess.
Michael et al. 26 found that the risk of recurrence was increased when the child had ill-defined and large abscesses. Zerem et al. 27 conducted a prospective study comparing the therapeutic efficiency of percutaneous drainage with antibiotic agents versus antibiotic therapy alone, which suggested that recurrence of appendiceal abscess was more likely to develop when patients with a mass size ≥3 cm were treated with antibiotic agents alone. We used ultrasonography to diagnose appendiceal abscess and provide a measurement of the mass size. The imaging of irregular-shaped and ill-defined hypoechoic or anechoic area implies the diagnosis of appendiceal abscess. The longest diameter of the mass was used to describe the mass size. Inevitable bias might exist in the measurement of mass size for different radiologists. Those researchers did not mention that the mass size differs in children with different BSA. Therefore, we analyzed the ratio of mass size to BSA, which could reflect each individual's condition better, and the results showed that those indicators at discharge in the recurrent group were higher than those in non-recurrent group. In other words, children with appendiceal abscess whose WBC at discharge is > 8.0 × 109/L and ratio of mass size to BSA at discharge is > 4.255, are considered the higher risk of recurrence, and interval appendectomy is recommended.
As a retrospective study, our research has some limitations. One is that there may exist some degree of bias. Another is that the number of patients with recurrent appendiceal abscess was limited because of the low risk of recurrence. Further large-scale, prospective trials are needed to determine the generalizability of our conclusion about the relation between the risk factors and recurrent appendiceal abscess.
Conclusions
Our study concluded that a longer course of intravenous antibiotic agents was strongly associated with a reduced risk of recurrence and patients with a WBC count at discharge >8.0 × 109/L and the ratio of mass size to BSA at discharge >4.255 are more likely to develop recurrent appendiceal abscess after initial conservative treatment without drainage. Therefore, an interval appendectomy is recommended for such children because of high recurrence rate. Continued oral antibiotic agents after discharge can effectively reduce the risk of recurrence of appendiceal abscesses.
Footnotes
Authors' Contributions
PengCheng Luo conceived and designed the study, collected data, interpreted data, and prepared for manuscript writing. DengLiang Wang collected data, interpreted data, and prepared for manuscript writing. Quan Kang designed the study, interpreted data, and improved writing. All authors read and approved the final manuscript submission.
Funding Information
There was no funding for this study.
Author Disclosure Statement
The authors have no conflicts of interest or financial relations to declare.