
Abstract
Abstract
Background:
Pseudomonas aeruginosa is an opportunistic pathogen that can cause various life-threatening infections. Several unique characteristics make it the ability of survivability and adaptable and develop resistance to antimicrobial agents through multiple mechanisms. Heteroresistance, which is a subpopulation-mediated resistance, has received increasing attention in recent years. Heteroresistance may lead to unexpected treatment failure if not diagnosed in time and treated properly. Therefore, heteroresistant Pseudomonas aeruginosa infections pose considerable problems for hospital-acquired infections. However, the clinical prevalence and implications of Pseudomonas aeruginosa heteroresistance have not been reviewed.
Results:
In this work, the aspects of the clinically reported heteroresistance of Pseudomonas aeruginosa to commonly used antibiotic agents are reviewed. The prevalence, mechanisms, and clinical relevance of each reported heteroresistant Pseudomonas aeruginosa are discussed.
Pseudomonas aeruginosa is an opportunistic pathogen in humans and the third most common cause of nosocomial infections. Pseudomonas aeruginosa can cause various life-threatening acute and chronic infections, such as ventilator-associated pneumonia, 1 burn wound infections, 2 urinary tract infections (UTIs), 3 device-related infections, 4 otitis externa, 5 bone and joint infections, 6 gastrointestinal infections, bacteremia and systemic infections,7,8 and so on. Several unique characteristics, including multiple virulence factors, survivability, environmental transmission, and widespread resistance to antimicrobial agents, make it a potential pathogen, especially for people with compromised immune systems.9,10 Eight categories of antimicrobial agents are commonly used to treat Pseudomonas aeruginosa infection: penicillins with β-lactamase inhibitors, cephalosporins, monobactams, carbapenems, aminoglycosides, fluoroquinolones, polymyxins, and phosphonic acids.11,12 Because of increasing resistance to antibiotic agents, Pseudomonas aeruginosa has become a serious health-care–associated pathogen with high morbidity and mortality. 13
Pseudomonas aeruginosa is a public health threat worldwide because of a range of mechanisms for adaptation, survival, and resistance to multiple antibiotic agents. It displays resistance to various antibiotic agents, including β-lactams, aminoglycosides, quinolones, and polymyxins 14 . Multi-drug–resistant Pseudomonas aeruginosa has been classified as a serious threat by the U.S. Centers for Disease Control and Prevention. 15
In addition to the conventional drug resistance phenotypes, Pseudomonas aeruginosa has also developed a special form of drug resistance, that is, heteroresistance. In contrast to full resistance, heteroresistance is a form of subpopulation-mediated resistance in which a seemingly isogenic strain harbors one or several minority subpopulations that exhibit increased levels of antibiotic resistance compared with the main population. 16 The resistant subpopulation of the heteroresistant strain is enriched and predominated in the presence of a given antibiotic but can return to baseline after antibiotic withdrawal, indicating that heteroresistance is an unstable phenotype. 17
As demonstrated in several in vivo animal studies,19-23 heteroresistance may cause antibiotic treatment failure because of the selection of resistant subpopulations during antibiotic treatment. 18 A case report of vancomycin heteroresistance in Staphylococcus aureus involved in neonatal sepsis has shown a clinical influence on vancomycin treatment. 24 Because of the low frequency of the presence of resistant subpopulations and unstable phenotypes and genetics, heteroresistance is often undetected by traditional standard antimicrobial susceptibility testing (AST) methods. 16 Therefore, in clinical practice, antibiotic heteroresistance cannot be identified without any specific identification, and its clinical relevance remains unclear. Notably, the clinical outcomes of Pseudomonas aeruginosa infections, which may be related to heteroresistance, are generally worse than those of other gram-negative organisms. Despite the risk of poor treatment outcomes, 25 heteroresistance has not received much attention in Pseudomonas aeruginosa studies.
Several excellent reviews have been conducted on the antibiotic resistance of Pseudomonas aeruginosa, including some aspects of mechanisms, alternative therapeutic options, and management.26–32 However, the heteroresistance of Pseudomonas aeruginosa isolates and mechanisms in clinics has rarely been reviewed. Thus, this review focuses on the reported epidemiology and mechanisms, as well as the clinical relevance, of Pseudomonas aeruginosa heteroresistance in clinical isolates. The lack of a standard definition and detection method for heteroresistance may lead to the misidentification of homogeneous strains as heteroresistance, hindering the proper assessment of their clinical relevance. 17 Here, we also discuss the latest canonical definition and detection methods of heteroresistance.
Heteroresistance of Pseudomonas aeruginosa
Heteroresistance phenomenon of bacteria
Heteroresistance is a phenomenon in which one or more heterogeneous subpopulations of bacteria are resistant to antibiotic agents at a higher level than the main population in the same culture. 17 Because the proportion of resistant colonies is very small and usually undetected, heteroresistant isolates are usually determined as susceptible by the clinically commonly used AST methods such as E-test, K-B method, broth or agar dilution method, and automatic instrument method. 33 During antibiotic treatment, the susceptible main populations are killed by a given antibiotic, whereas the resistant subpopulations can be enriched and grow to high numbers in the infected host and ultimately leading to conventional antimicrobial treatment failure, as shown in Figures 1 and 2.
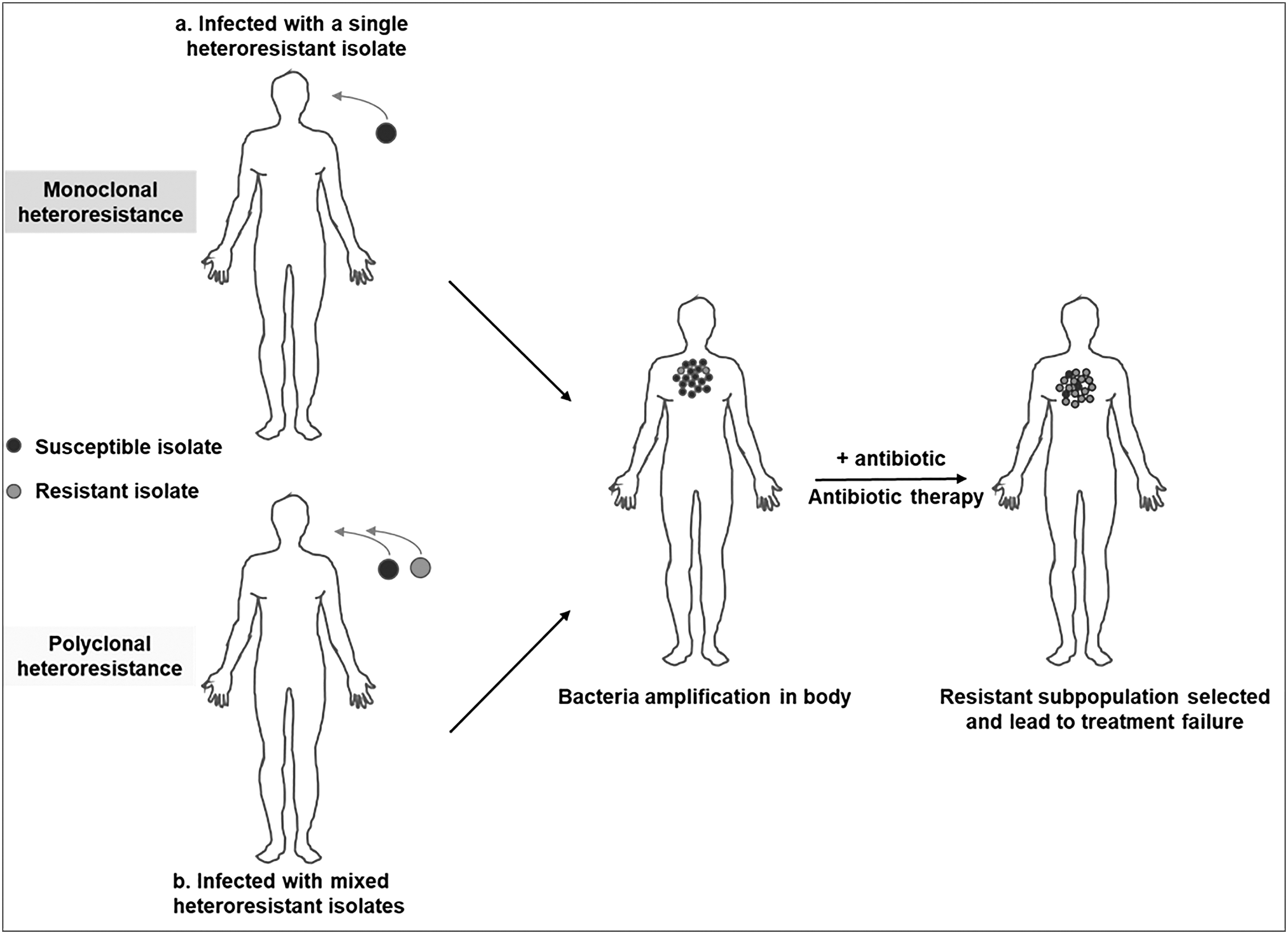
Heteroresistant bacterial infections may cause clinical antibiotic treatment failure. A patient infected with a heteroresistant bacterial isolate contains both a susceptible main population and a resistant subpopulation. Because of the small fraction of the resistant subpopulation, it may not be detected by clinical antibiotic susceptibility (AST) testing methods, and the AST results would be incorrectly assessed as susceptible to a given antibiotic. When treated with the antibiotic in which the isolate shows heteroresistance, the resistant subpopulation is selected and can grow in the presence of the drug. Therefore, inappropriate antibiotic treatment may lead to treatment failure. Heteroresistance is classified into monoclonal and polyclonal types according to its origin and mechanism. Monoclonal heteroresistance refers to a single heteroresistant isolate that can differentiate into two or more populations (a main susceptible and one or more resistant subpopulation) at a high frequency (commonly greater than 1 × 10−7, which is higher than mutations that cause full antibiotic resistance in susceptible cells) in the absence of antibiotic pressure. Therefore, monoclonal heteroresistance is present and can be detected in pure clones. Polyclonal heteroresistance refers to a mixed infection of susceptible and resistant bacteria. Thus, polyclonal heteroresistance can only be detected in populations.

Stability of the heteroresistance phenotype. A patient infected with a heteroresistant bacterial isolate containing a susceptible main population and a resistant subpopulation. The heteroresistant bacteria are subcultured without antibiotic agents, and clinical antibiotic susceptibility testing (AST) is then performed using commonly used AST methods, such as K-B or E-test or automatic instrument methods. The AST results show that the bacterial isolate is susceptible, and the patient is treated with a selected antibiotic guided by the AST results. Antibiotic therapy leads to unexpected treatment failure due to the presence of heteroresistance. Clinical AST is performed again, and the isolated sample is subcultured without antibiotic agents. (
Heteroresistance must be distinguished from other forms of subpopulation-mediated resistance, such as persistence and tolerance. Persistence is also caused by a small fraction of the isogenic subpopulation that displays increased resistance to antibiotic agents.34–37 In the presence of antibiotic agents, persistent cells are temporarily quiescent or grow slowly, whereas the heteroresistant subpopulation can grow rapidly and become the dominant population. 37 . Bacterial tolerance means that no pre-existing resistant bacteria may be present before exposure to antibiotic agents; however, the entire bacterial population can survive the moment of exposure to a high concentration of antibiotic. 36
The heteroresistance phenomenon has been reported in a wide range of clinical pathogenic bacteria, such as Enterobacter cloacae,38,39 Staphylococcus aureus,40,41 Klebsiella pneumoniae,42,43 Escherichia coli,44,45 Acinetobacter baumannii,23,46,47 Pseudomonas aeruginosa,48,49 and so on. Antibiotic agents found in heteroresistance phenomena mainly include carbapenems (imipenem [IPM] and meropenem [MEM]) and polymyxins (colistin and polymyxin B). 50
Definition of heteroresistance
Before El-Halfawy et al. 17 recommended an operational definition and uniform criteria for the assessment of heteroresistant bacteria, the term “heteroresistance” had been applied willfully, and heteroresistance-determining methods vary greatly among different laboratories. El-Halfawy et al. 17 focused on the existence of a subpopulation of resistant cells with minimum inhibitory concentration (MIC) values at least eightfold higher than the highest drug concentration that does not inhibit the growth of the main susceptible population. To easily compare future studies on heteroresistance, Andersson et al. 50 suggested an update of the heteroresistance definition provided by El-Halfawy et al. 17 and proposed that the four factors of heteroresistance should be clearly defined and measured whenever possible. The factors mentioned are: (1) the clonality of resistant subpopulations: depending on the origin and mechanism, heteroresistance can be classified into monoclonal and polyclonal types23,50,51; (2) the resistance level of resistant subpopulations: the MICs of the potentially heteroresistant subpopulation are at least eightfold higher than that of the susceptible main population; (3) the frequency of resistant subpopulations: a potential resistant subpopulation present at a high frequency mostly greater than 1 × 10−7; and (4) stability of heteroresistant phenotype.
Heteroresistance detection methods
The reported cases of heteroresistance in clinical pathogens were detected by all kinds of methods commonly or infrequently used in clinical laboratories.
Population analysis profiling
The population analysis profiling (PAP) test is the gold standard method for detecting heteroresistance. 17 The bacterial population was subjected to a gradient of antibiotic concentrations (generally with twofold increments) on plates, and bacterial growth at each concentration was quantified by counting the colony forming units (CFU). The frequency of heteroresistant subpopulations was calculated by dividing the number of colonies grown on the plate with the highest concentration of antibiotic agents by the number of colonies growing on the same bacterial inoculum on the antibiotic-free plate.
Turbidimetric PAP assay refers to PAP performed by the broth dilution method in a liquid medium. Bacterial cultures were treated with twofold increments or increments of twofold of antibiotic concentrations, and bacterial growth in broth at each concentration was measured by turbidimetry.52,53
The population analysis profiling-area under the curve (PAP-AUC) assay is a modified PAP method used to determine the heteroresistance of Staphylococcus aureus to vancomycin by comparing the AUC between the tested strain and the reference heteroresistant strain Mu3.54–57 However, this method depends on the response of the reference strain to antibiotic agents, and if the resistance of the control strain is not stable, the results are greatly affected.
The microdilution plating method for population analysis (mPAP) of antibiotic-resistant Staphylococci using CFU per milliliter determinations in 10 μL droplets was performed.23,58 The mPAP technique yielded similar population resistance profiles to the typical reference PAP test and was highly efficient and rapid and used less resources. However, it may have poor sensitivity for heteroresistance screening, as potential inaccuracies in dropping a smaller volume of such a low frequency of resistant cells onto a plate. In addition, a “coffee rings” phenomenon often occurs, which may lead to an inaccurate count of resistance cells.33,59
Even though the PAP method is reliable and can provide good information on the frequency and MIC values of resistant subpopulations in the detection of heteroresistance, it is time-consuming, complicated, and difficult to apply for clinical diagnosis.
Disk diffusion and E-test
Traditional AST methods, such as disk diffusion (K-B) and E-test strips, are also used to detect heteroresistance. 60 Heteroresistance is indicated by the presence of distinct colonies growing within the clear zone of inhibition in disk diffusion or E-test assays. A special E-test strip (GRD E-test) was used for glycopeptide resistance detection.60–62 The limitation of disk diffusion and the E-test method is that they are not quantitative and often yield false-positive or negative results because of the low density of cells on plates.23,63,64
Modified E-tests (macromethod E-test) with cell densities higher than usual were used to increase the probability of the presence of resistant bacteria in the subpopulation.23,54 Regarding cell densities, colonies on Mueller–Hinton plates were re-suspended with phosphate-buffered saline (PBS) or saline solution to two MacFarland units (approximatively 6 × 108 cells mL−1), or the bacteria grown overnight in Mueller–Hinton broth were diluted at a ratio of 1:7 with PBS. Even though high cell density on the plate increases the probability of detecting resistant subpopulations, there is also a higher risk of false-positives due to inoculation effects.
The E-test or disk diffusion method is simple and convenient and can be used for the rapid screening of clinical isolates. However, its detection of resistant subpopulations with low frequency is poor, and it is prone to false-positive results due to its low specificity in detecting heteroresistance.
Agar dilution
Agar plates containing dilutions of a linear gradient of antibiotic concentrations can also be used to detect heteroresistance. 65 It can determine the antibiotic susceptibility of clinical isolates and identify antibiotic-resistant cells in bacterial populations. 66 Information, such as the frequency and MIC value of the resistant subpopulation, can be acquired. In contrast to the PAP test, a single small inoculum was plated on an agar plate. Similar to the disk diffusion method, the gradient method can detect only high-rate heteroresistance.
Time-killing assay
Heteroresistance can also be detected by measuring bacterial growth over time after antibiotic treatment using the time-killing kinetic assay.43,46 The growth of heteroresistant bacteria decreased sharply in the initial period and then increased slowly at later time points, indicating that the susceptible subpopulations were killed in the presence of antibiotic agents and that the resistant subpopulations were selected and grew. Growth curves showed a longer lag phase and a shorter exponential phase for the heteroresistant subpopulations than for their respective native populations, indicating that an increased incubation time for the proliferation of less abundant and highly resistant members of the population was necessary in detecting the resistant subpopulations in phenotypic tests.17,48
Molecular and biochemical methods
Rapid molecular and biochemical methods were used to identify the heteroresistance of a specific antibiotic. Whole genome sequencing 67 and droplet digital polymerase chain reaction (PCR) 68 or random amplified polymorphism DNA (RAPD profile) 69 have been used to detect Helicobacter pylori heteroresistance. The inclusion of the genotype MTBDR line probe assay (LPA) with BACTEC MGIT drug susceptibility testing enabled the detection of heteroresistance in Mycobacterium tuberculosis. 70 Reverse transcription-polymerase chain reaction (RT-PCR) and microscopic observation drug susceptibility (MODS) exhibit synergistic effects on the speed of detection of heteroresistance in tubercle bacillus. 71 Flow cytometry using a fluorescent penicillin derivative is a novel approach employed to assess the heteroresistance of methicillin-resistant Staphylococcus aureus. 72
Two-step schedule for heteroresistance determination
El-Halfawy et al. 17 recommended a two-step scheme to rigorously determine heteroresistance by combining disk diffusion or E-test assay for preliminary screening with the PAP test for further confirmation.
Heteroresistance of Clinical Pseudomonas aeruginosa
Pseudomonas aeruginosa is heteroresistant to most commonly used therapeutic agents, including cephalosporins, penicillin combined with β-lactamase inhibitors, carbapenems, polymyxin, and fosfomycin. The reported heteroresistance of Pseudomonas aeruginosa is summarized in Table 1.
Summary of the Reported Heteroresistance in Pseudomonas aeruginosa
HR = heteroresistance; PAP = population analysis profiling; PFGE = Pulsed-field gel electrophoresis; FEP-HR = cefepime heteroresistance;
IMP-HR = imipenem heteroresistance; CAZ-HR = ceftazidime heteroresistance; MEM- HR = meropenem resistance; MLST = multilocus sequence typing.
Cefepime heteroresistance
The heteroresistance of Pseudomonas aeruginosa to cephalosporins has rarely been reported. The cefepime heteroresistance (FEP-HR) of Pseudomonas aeruginosa isolated from patients with bacteremia was reported for the first time in Chongqing, southwest China. 73 A high prevalence (57.3%) of FEP-HR was observed. Besides FEP-HR, some Pseudomonas aeruginosa isolates showed cross-heteroresistance to multiple antibiotic agents, such as ceftazidime, MEM, and IPM.
Carbapenem heteroresistance
Carbapenems are one of the main and most commonly used antibiotic agents for the treatment of Pseudomonas aeruginosa infections. Among these, MEM and IPM are effective agents for the treatment of multiple drug-resistant Pseudomonas aeruginosa. The heteroresistance of Pseudomonas aeruginosa to carbapenems, mainly IPM and MEM, has been reported and studied the most compared with other antibiotic agents. Both MEM- and IPM-heteroresistant isolates were reported in the First Affiliated Hospital of Chongqing Medical University (Chongqing, China), 74 the Kunshan Hospital Affiliated to Nanjing University of Traditional Chinese Medicine and Changzhou Tumor Hospital Soochow University (Kunshan and Changzhou, China), 75 the First Affiliated Hospital of Wenzhou Medical University (Wenzhou, China), 76 the University Hospital of Larissa (Greece),48,77, and a hospital in Italy. 78
Polymyxin heteroresistance
Polymyxin B and colistin (i.e., polymyxin E) are the polymyxin antibiotic agents used in the clinic as a last resort treatment when no other effective antibiotic agents are available. However, recent clinical pharmacokinetic studies have shown that even at the recommended upper-limit daily dose, the plasma concentrations of colistin remain suboptimal in a large proportion of critically ill patients.79,80 The heteroresistance phenotype of Pseudomonas aeruginosa to polymyxins has also been reported relatively often. Colistin-heteroresistant Pseudomonas aeruginosa isolates were detected in Wenzhou (China), 81 Atlanta, Georgia (United States), 33 and Semmelweis University (Budapest, Hungary). 45 The reference Pseudomonas aeruginosa strain ATCC 27853 has also shown colistin heteroresistance phenotype in some studies. 82 Polymyxin B heteroresistance in Pseudomonas aeruginosa was first evaluated in the Hospital de Clı´nicas de Porto Alegre (Rio Grande do Sul, Brazil). 49
Piperacillin-tazobactam heteroresistance
Pseudomonas aeruginosa strain PA7171 was isolated from a UTI sample of a 38-year-old male who was hospitalized for seven days at the University Hospital of Larissa in November 2006. PA7171 was reported to be susceptible to piperacillin-tazobactam by automated systems and agar dilution methods. However, the isolate exhibited distinct colonies within the inhibition zone of the piperacillin-tazobactam disk and E-test strips. Population analysis showed that PA7171 can grow in up to 128 mg/L piperacillin-tazobactam, with a frequency of approximately 10−7. 83
Fosfomycin heteroresistance
Fosfomycin heteroresistance is defined as the presence of subpopulations that can grow on agar containing 64 mg/L fosfomycin within fosfomycin-susceptible isolates (i.e., MIC of ≤64 mg/L). A total of 64 clinical Pseudomonas aeruginosa isolates were investigated; among these, 59 isolates were obtained from Alfred Hospital (Melbourne, Australia), and five isolates were obtained from Royal Brisbane and Women's Hospital (Brisbane, Australia). 84 A total of 14 isolates were randomly selected from 39 fosfomycin-susceptible isolates, with MIC values of ≤64 mg/L, and the possible presence of fosfomycin-resistant subpopulations was determined via the PAP test. The results showed that heteroresistance was observed in all examined fosfomycin-susceptible isolates.
Clinical Relevance
Cefepime heteroresistance
Jia et al. 73 reported the first case of FEP-HR in Pseudomonas aeruginosa that affected clinical outcomes. This report was the first clinical evidence that heteroresistance is an intermediate stage in the evolution from susceptibility to full resistance in patients on long-term antibiotic treatment. Compared with the control patients with non-FEP-HR bacteremia, patients with FEP-HR bacteremia were significantly likelier to have advanced age, hematologic malignancies, central venous catheters, and exposure to cephalosporins and carbapenems, which were independent risk factors. Patients with FEP-HR infection generally have a higher risk of treatment failure than those with non-FEP-HR infection. In addition, functional status deterioration and a longer length of hospital stay were more common in patients with FEP-HR infection. However, no statistically significant differences were found in all-cause mortality and in-hospital mortality between the case group and the control group.
Carbapenem heteroresistance
He et al. 74 found that clinical features, such as male gender, hypoalbuminaemia, UTI, surgery in the past six months, drainage tube, urinary catheter, nasogastric catheter, and prior carbapenem exposure within the past three months, were more common in patients with IPM-HR than in patients with non-IPM-HR. Males, drainage tubes, and carbapenem exposure within the past three months were independent risk factors for the acquisition of IPM-HR isolates. In contrast, excluding urinary catheter and prior carbapenem usage, different risk factors, such as transfer from another hospital, intensive care unit (ICU) admission, gastrointestinal disease, and enema, were common in patients with MEM-HR isolates. Transfer from another hospital and prior carbapenem therapy were independent risk factors for the acquisition of MEM-HR isolates. The incidence of IPM and MEM heteroresistance was correlated with total carbapenem consumption. Regarding clinical outcomes, patients with MEM-HR isolates had a longer total length of hospital stay than those with non-MEM-HR isolates, and worsening functional status was more common; however, no difference was observed between patients with IPM-HR and non-IPM-HR isolates. Furthermore, no statistically significant difference was found in in-hospital mortality between the cases and the controls.
Colistin heteroresistance
The association between colistin heteroresistance in carbapenem-resistant Pseudomonas aeruginosa and clinical outcomes in patients without cystic fibrosis was evaluated in an observational study. 33 No statistically significant difference was observed in the 90-day mortality or 30-day mortality between the colistin heteroresistance group and the non-heteroresistant group. In addition, few differences were observed in demographics or clinical characteristics between patients with and without heteroresistant isolates. However, patients with HR2 isolates tended to have longer hospital lengths of stay than patients without HR2 isolates. 33
Piperacillin-tazobactam heteroresistance
The patient infected with piperacillin-tazobactam–heteroresistant Pseudomonas aeruginosa in the urinary tract had a good clinical response to piperacillin-tazobactam treatment. 83 The treatment regimen was not changed after the discovery of piperacillin-tazobactam heteroresistance, and no growth in the isolates was observed in repeated urine cultures one week after the end of therapy and one month after hospital discharge.
Heteroresistance Mechanism of Pseudomonas aeruginosa
Mechanism of FEP-HR
Jia et al. 73 investigated the mechanisms of FEP-HR in Pseudomonas aeruginosa. The results suggest that the elevated expression level of AmpC cephalosporinase, rather than extended-spectrum β-lactamases (ESBL) production, efflux pump overexpression, or OprD deficiency, is responsible for FEP-HR in Pseudomonas aeruginosa.
Mechanism of carbapenem heteroresistance
Most studies have demonstrated that carbapenem heteroresistance in Pseudomonas aeruginosa is mainly caused by the overexpression of the efflux system mexB, mexC, mexE, and mexX74–76,85 and the downregulation of outer membrane porin OprD.74,76,85 Biofilm formation may be involved in the carbapenem heteroresistance of Pseudomonas aeruginosa. Some carbapenem-heteroresistant Pseudomonas aeruginosa have increased levels of biofilm formation, 74 whereas others have not exhibited increased levels. 76 Neither the carbapenemases 76 nor metallo-β-lactamase (MBL)74,75,85 production was detected in all carbapenem-heteroresistant isolates. No difference in AmpC expression was found between carbapenem heteroresistance isolates and their native isolates. 74
Oikonomou et al. 77 proposed that Pseudomonas aeruginosa may produce two different types of heteroresistant subpopulations when carbapenem was used. A fraction of persisters results in unstable heteroresistant subpopulations, and a fraction of stable resistant mutants results in stable heteroresistant subpopulations. 77 However, this is questionable, because persistence is different from heteroresistance.
Mechanism of colistin heteroresistance
The resistance of Pseudomonas aeruginosa to polymyxins is mainly generated by lipid A modification by adding L-Ara4N through the pmrHFIJKLM operon and under the control of two-component systems (TCSs), pmrAB, and phoPQ.86,87 Lin et al. 81 explored the mechanisms of colistin heteroresistance in Pseudomonas aeruginosa isolates. Alteration of the PmrAB regulator system was the main mechanism of colistin heteroresistance. Major non-synonymous substitutions in PmrB were found in all colistin-(hetero)resistant isolates. Other TCSs, such as PhoPQ, ParRS, and CprRS, except for colRS, also mediate colistin heteroresistance. 81
The mechanisms of polymyxin B, piperacillin-tazobactam, and fosfomycin heteroresistance have not been studied.
Conclusion and Further Direction
Pseudomonas aeruginosa is an important clinical pathogen that causes a wide range of mild to severe infections. Eight classes of antibiotic agents are commonly used to treat Pseudomonas aeruginosa infections 31 ; however, strains resistant to these antibiotic agents have emerged. Resistance mechanisms include intrinsic, acquired, and adaptive resistance. 27 As a special resistance phenotype and an emerging field, heteroresistance has received increasing attention. Its genetics and phenotype are unstable and are not easy to accurately detect using commonly used clinical AST methods. The lack of a unified definition of heteroresistance and methodologies for rapid detection may hinder the proper assessment of its clinical relevance. 17 Therefore, the importance and clinical significance of heteroresistance are controversial.18,19,24,88,89
The heteroresistance to penicillin, cephalosporin, carbapenems, polymyxins, and fosfomycin of Pseudomonas aeruginosa has been reported, and the incidence is high in clinical isolates. These reported areas were mainly in China and European countries, as shown in Table 1. However, heteroresistance to rifampicin, fluoroquinolones, and aminoglycosides has not been reported. The heteroresistance of Pseudomonas aeruginosa to carbapenems and polymyxins has been reported relatively often, which may be related to their high clinical consumption. 74 Most of these heteroresistant Pseudomonas aeruginosa strains were preliminary screened by the K-B or E-test method and then identified by the PAP method or the time-killing assay. The PFGE patterns of the heteroresistant and native populations were identical. Homologous analysis by MLST showed that the different heteroresistant isolates investigated were epidemiologically unrelated. 81 All of these reported heteroresistant isolates were monoclonal, and the frequency was above 10−7. The MIC values of resistant subpopulations were four- to eightfold higher than those of the main populations, and the heteroresistant phenotype of most isolates was stable. Therefore, these reported heteroresistance phenomena basically meet the criterion of the definition recommended by Andersson et al., 50 and they are of reference significance for subsequent research.
The mechanism of Pseudomonas aeruginosa heteroresistance to cephalosporins is due to the production of the AmpC enzyme. 73 Carbapenem heteroresistance is mainly caused by the reduction of OprD and overexpression of the efflux system, whereas AmpC, MBL, and carbapenemase are not involved in heteroresistance.74–76,85 Polymyxin heteroresistance is mainly due to the alteration of the TCS, 81 as shown in Table 2.
Clinical Relevance of Heteroresistant Pseudomonas aeruginosa in Patients
HR = heteroresistance; IPM-HR = imipenem heteroresistance; MEM-HR = meropenem heteroresistance; ICU = intensive care unit.
Pseudomonas aeruginosa heteroresistance to FEP, 73 IMP, MEM, 74 and polymyxins 33 adversely affects clinical outcomes. However, heteroresistance to piperacillin-tazobactam exhibited no effect on clinical treatment outcome, 83 as shown in Table 3. Some clinically relevant risk factors for acquired infection with heteroresistant isolates, such as male gender, older age, invasive surgery, ICU admission, and previous antibiotic exposure, were found. 74 Antibiotic consumption was also positively correlated with the incidence of heteroresistance. Heteroresistant Pseudomonas aeruginosa infection may aggravate the patient's condition and functional status and remarkably prolong the duration of treatment and hospital stay. However, no effect on all-cause mortality was observed.
Summary of the Heteroresistance Mechanism of Pseudomonas aeruginosa to Antibiotic Agents
ESBL = extended-spectrum β-lactamase; MBL = metallo-β-lactamase; TCS = two-component system.
Heteroresistance of Pseudomonas aeruginosa has been relatively scarcely reported and later than other common clinical pathogens, and those reports were mainly conducted in the past 15 years, as shown in Table 1. No heteroresistance has been reported in other antibiotic agents commonly used to treat Pseudomonas aeruginosa, such as rifampicin, aminoglycosides, and fluoroquinolones. Is this because Pseudomonas aeruginosa does not develop heteroresistance to these antibiotic agents? Or has the phenomenon of heteroresistance not been noticed in these antibiotic agents before? The reported heteroresistance phenomenon of Pseudomonas aeruginosa remains relatively sparse and requires more attention. Hospitals and bacterial resistance surveillance institutions should monitor the clinical heteroresistance clone, molecular typing, and epidemiology of Pseudomonas aeruginosa. The four factors of heteroresistance proposed by Andersson et al. 50 should be considered to describe the heteroresistance of Pseudomonas aeruginosa in future reports so that different studies can be compared and analyzed, which will help to further clarify the clinical relevance and significance. In addition, given that no practical methods are currently available to accurately and rapidly detect heteroresistance in clinical microbiology laboratories, 50 a simpler AST method that meets the needs of clinical heteroresistance detection should be urgently developed.
Footnotes
Authors' Contributions
Zhao Chen had the idea for the article and wrote the manuscript and performed the literature search and data analysis.
Funding Information
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.