
Abstract
Background:
It is recognized increasingly that common surgical infections of the peritoneal cavity may be treated with antibiotic agents alone, or source control surgery with short-course antimicrobial therapy. By extension, testable hypotheses have emerged that such infections may not actually be infectious diseases, but rather represent inflammation that can be treated successfully with neither surgery nor antibiotic agents. The aim of this review is to examine extant data to determine which of uncomplicated acute appendicitis (uAA), uncomplicated acute calculous cholecystitis (uACC), or uncomplicated mild acute diverticulitis (umAD) might be amenable to management using supportive therapy alone, consistent with the principles of antimicrobial stewardship.
Methods:
Review of pertinent English-language literature and expert opinion.
Results:
Only two small trials have examined whether uAA can be managed with observation and supportive therapy alone, one of which is underpowered and was stopped prematurely because of challenging patient recruitment. Data are insufficient to determine the safety and efficacy of non-antibiotic therapy of uAA. Uncomplicated acute calculous cholecystitis is not primarily an infectious disease; infection is a secondary phenomenon. Even when bactibilia is present, there is no high-quality evidence to suggest that mild disease should be treated with antibiotic agents. There is evidence to indicate that antibiotic prophylaxis is indicated for urgent/emergency cholecystectomy for uACC, but not in the post-operative period. Uncomplicated mild acute diverticulitis, generally Hinchey 1a or 1b in current nomenclature, does not benefit from antimicrobial agents based on multiple clinical studies. The implication is that umAD is inflammatory and not an infectious disease. Non-antimicrobial management is reasonable.
Conclusions:
Among the considered disease entities, the evidence is strongest that umAD is not an infectious disease and can be treated without antibiotic agents, intermediate regarding uACC, and lacking for uAA. A plausible hypothesis is that these inflammatory conditions are related to disruption of the normal microbiome, resulting in dysbiosis, which is defined as an imbalance of the natural microflora, especially of the gut, that is believed to contribute to a range of conditions of ill health. As for restorative pre- or probiotic therapy to reconstitute the microbiome, no recommendation can be made in terms of treatment, but it is not recommended for prevention of primary or recurrent disease.
With increasing recognition that common surgical infections of the peritoneal cavity (e.g., uncomplicated acute appendicitis [uAA], uncomplicated acute calculous cholecystitis [uACC], and uncomplicated mild acute diverticulitis [umAD]) may be treated with antibiotic agents alone,1–3 or source control surgery with short-course antimicrobial therapy,4,5 plausible, testable hypotheses have emerged that such infections might be treatable successfully with neither, using supportive therapy alone. To do so, numerous obstacles must be overcome. Randomized controlled trials (RCTs) of surgical therapy are difficult to conduct, 6 especially if a comparator arm is non-surgical. 7 Potential reasons are multiple, including a treatment that is perceived to be a radical departure from the standard of care; discomfort with randomization, especially on the part of patients; lack of equipoise regarding preferences for treatment on the part of patients and clinicians; and imbalanced presentation of interventions. 7 Diagnosis of the diseases under study must be made as accurately as possible, to avoid underpowering a study inadvertently by enrollment of ineligible subjects. 8
Distinguishment of inflammation and infection has been sought by medical practitioners for more than 150 years since the time of Joseph Lister 9 (Fig. 1) and Louis Pasteur10,11 (Fig. 2). The quest, ever more sophisticated, continues to this day. History and physical examination, although indispensable to evaluation, are neither sensitive nor specific.12–15 Fever, which appears to be a salutary host response,16,17 is an unreliable criterion, being a marker of inflammation as commonly as infection.18,19 Systemic inflammatory response syndrome (SIRS) criteria, an amalgam of physical and laboratory findings (fever or hypothermia, tachycardia, tachypnea or hypocapnia, and leukocytosis or leukopenia) lack diagnostic accuracy but can inform prognostication in serious cases.19,20 Disappointment with the performance of standard laboratory diagnostics has led to evaluation of additional biomarkers such as C-reactive protein and procalcitonin, with only modest diagnostic improvement.21–26

The Right Honorable Lord Joseph Lister, First Baron Lister, OM, PC, PRS, FRCS (Edin), FRCP (Glas) (1827–1912), 10 years before his death at age 84. Source: www.wikipedia.com. Image in the public domain.

Louis Pasteur, ForMemRS, (1822–1895), experimenting in his laboratory (date unknown). Source: www.wikipedia.com. Image in the public domain.
Advancing technology and enhanced safety protocols that minimize exposure to ionizing radiation have made imaging of the acute abdomen almost ubiquitous,27,28 with ultrasound often favored for imaging of children, during pregnancy, and for the biliary tree of adults. Imaging has better diagnostic performance than routine laboratory testing, but falls short of infallibility,29–34 even for computed tomography (CT). Nuclear medicine has progressed from the days of 67 Ga scintigraphy, which is non-specific for distinguishing inflammation from infection, and not especially useful for abdominal imaging because of excretion via the colon. 111 In-tagged leukocyte imaging was superior to 67 Ga for acute infections, including of the abdomen and pelvis, but is now seldom used. Difficulty in distinguishing between bacterial infection and sterile inflammation using radiopharmaceuticals has led to study of 67 Ga- or 99mTc-labeled antimicrobial agents 35-38 and peptides, 39 but these remain investigational.
Variable ensembles of diagnostic tests, due to lack of standardization and variable test performance, have led to development of various scoring systems 40 and the application of artificial intelligence to clinical diagnostics. 41 Accurate diagnostics are important to conduct studies of alternative therapies of infection, but so too is the opportunity to determine whether uAA, uACC, or umAD might be treatable without antimicrobial therapy. Such an approach would be consistent with the principles of antimicrobial stewardship.42,43 Succinctly, stewardship encompasses use of the narrowest-spectrum antimicrobial agent in the correct dose for the shortest possible duration. The ability to exclude an infectious source, and to withhold antibiotic therapy, is a high expression of the art of antimicrobial stewardship and is rightly a point of emphasis in surgical practice.44–46
Is Uncomplicated Acute Appendicitis an Infectious Disease?
Data are scant regarding whether uAA can be treated without antibiotic agents or surgery. It may be informative for the reader to consider the nearly 300-year history of appendicitis management as a paradigm for how long it can take for medical dogma to change. 47 Only recently has the possibility of non-operative management (NOM) of uAA (without surgery) been considered rigorously.
Since the first recorded appendectomy in 1735, the pathogenesis and management of appendicitis have been debated continuously, but progress was glacial for 150 years. 47 In 1886, a seminal contribution by Reginald Fitz 48 described the pathogenesis in modern terms, but concurrent surgical discourse centered on when and how to operate,49–51 not whether. It was not until 1901 that NOM of complicated appendicitis was first broached by Albert Ochsner. 52 Operative mortality at the time was approximately 15% (Fig. 3) 53 ; Ochsner proposed not operating on severe cases with likely poor surgical outcomes (i.e., generalized peritonitis with shock) to, essentially, get them “off the books.” By so doing, Ochsner reported an 80% decrease of operative mortality, but his observations went unheeded for more than 50 years.
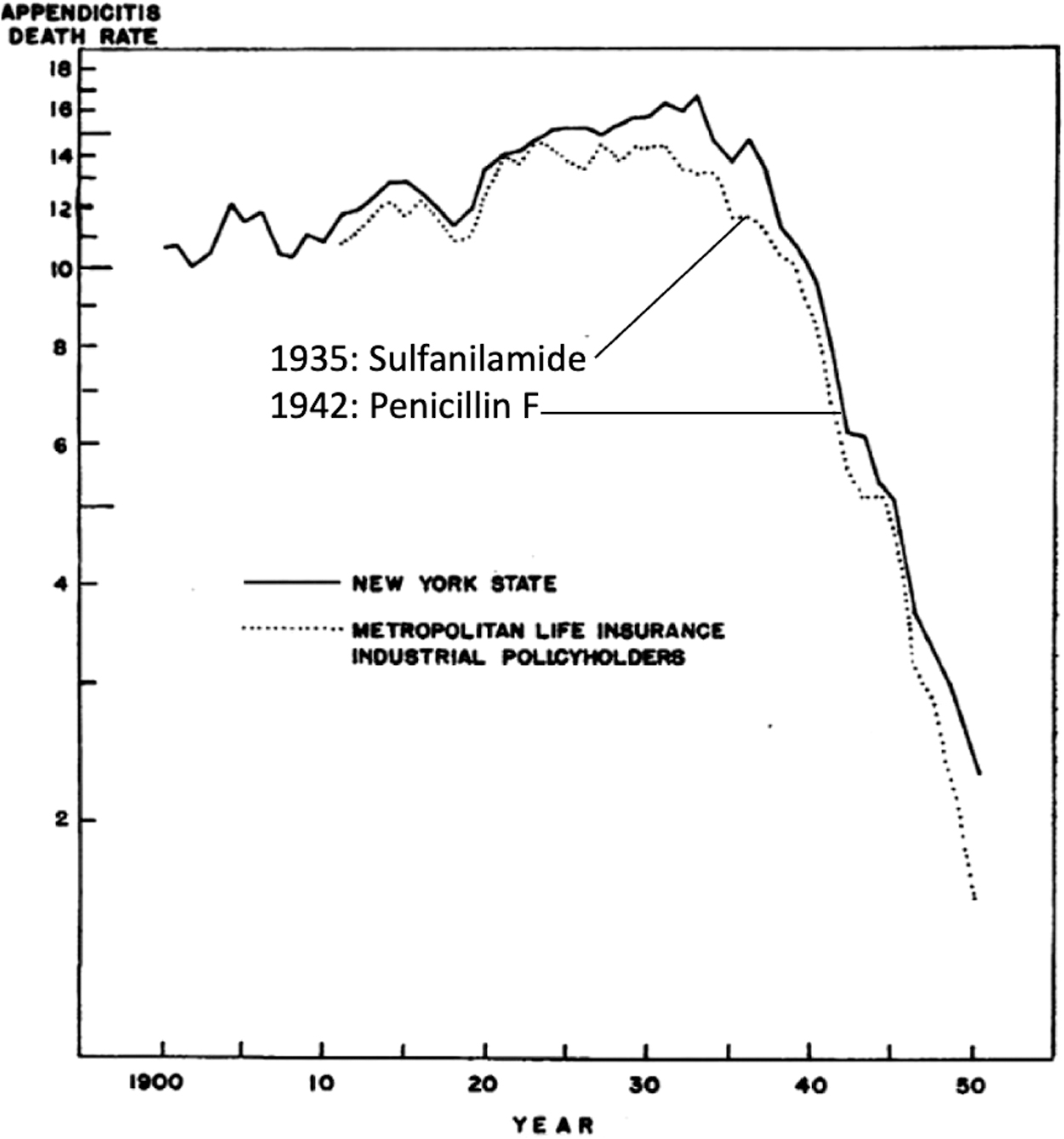
Actuarial data published in 1952 of appendicitis mortality 1900–1950, with clinical introductions of sulfanilamide and penicillin F superimposed. The association of antibiotic treatment with appendicitis mortality is apparent. Modified from Lembcke. 53 Image in the public domain.
The introduction of sulfanilamide in 1935
54
and
The first laparoscopic appendectomy by Kurt Semm in 1980 58 and the description of cross-sectional imaging to facilitate accurate diagnosis in 1998 59 heralded the modern era of operative appendicitis care. Diagnostic confidence that appendicitis is uncomplicated, imparted particularly by contrast-enhanced CT, led to numerous trials and meta-analyses that argue that NOM of appendicitis is non-inferior to laparoscopic appendectomy in the short term (up to 30 days),2,60 although ineligible subgroups have been identified.61,62 Moreover, concerns persist regarding a one-year failure rate of NOM of approximately 30% that may go even higher with longer follow-up, a higher incidence of appendiceal neoplasia among patients so treated,63,64 and a lack of cost-effectiveness. 65
The classical theory that AA progresses over time from uAA to complicated disease has been espoused for more than a century, 48 but an alternative hypothesis has emerged. To hypothesize that uAA is possible to manage with supportive therapy (e.g., fluids, bowel rest) alone, one need consider whether phlegmonous and gangrenous appendicitis are distinct entities, thus indicating a differential approach to therapy. Gene profiling of a small number (n = 29) of individuals showed that phlegmonous AA expresses a antiviral genotype, whereas gangrenous AA expresses an antibacterial genotype. 66 The hypothesis that uAA and gangrenous AA are distinct entities is supported further by observation that the appendiceal microbiome differs among uAA patients undergoing NOM and those with uAA or complicated appendicitis undergoing appendectomy.67,68 However, it is unknown whether alterations of the microbiome are causal or consequential to pathogenesis. One need consider further that uAA may undergo spontaneous resolution. Spontaneous resolution of AA was first observed more than a century ago. Clinical, epidemiologic, radiologic, and pathologic evidence suggests that disease can resolve spontaneously in “many” patients with uAA.69,70 However, supporting documentation is scant and of low quality. 70 As to how many, the prevalence of spontaneous resolution has been estimated between 8% and 13% based on ultrasound evaluation. 71 Of interest, estimated failure rates of as high as 40% and appendiceal diameter >8 mm as a risk factor for failure 71 are reminiscent of recent trials of NOM in the literature.2,62,70
Only two small trials have examined whether uAA can be managed with observation and supportive therapy alone (i.e., no antibiotic agents.) Park et al. 72 conducted a prospective, single-blind (radiologist was blind to clinical status and decision making), placebo-controlled RCT of 245 patients with CT-confirmed uAA. Excluded patients were those with appendiceal diameter >11 mm, appendicolith, extraluminal gas, intra-peritoneal fluid, or abscess or phlegmon. Patients were randomized 1:1 to receive supportive care (i.e., fluid, analgesia, antipyresis) and a four-day course of cefmetazole plus metronidazole or placebo drug (intravenous-to-oral switch therapy.) Median follow-up was 19 months. The primary endpoint, i.e., total treatment failure, was defined as initial treatment failure within one month and recurrent appendicitis during follow-up. There was no difference in failure rate (p = 0.61): no antibiotic agents 29 of 124 (23.4%) versus antibiotic agents 26 of 121 (20.7%).
The APPendicitis Acuta III (APPAC III) trial protocol was published in 2018. 73 APPAC III is a placebo-controlled, double-blinded, multicenter RCT of adults aged 18 to 60 years with low-dose CT-confirmed uAA. Hypotheses were two: Antibiotic therapy is necessary in the treatment of uAA and antibiotic therapy is superior to supportive care without antibiotic agents when the primary endpoint is evaluated at 10-days post-intervention. Inclusion criteria included CT evidence of appendiceal diameter >6 mm, with thickening and contrast enhancement of the wall, and peri-appendiceal edema with or without a minor fluid collection. Clinical exclusion criteria included: Age outside of range, allergy to antibiotic or contrast medium, chronic kidney disease, type 2 diabetes mellitus treated with metformin, pregnancy/lactation, and severe systemic illness. Exclusion criteria by CT included abscess, appendicolith, perforation, or tumor.
Versus placebo medications, the antibiotic regimen for APPAC III consisted of ertapenem 1 g intravenously for three days in-hospital, followed by levofloxacin 500 mg orally every day and metronidazole 500 mg orally every day for four days. The primary endpoint was resolution resulting in hospital discharge within 10 days of study initiation. Multiple secondary endpoints included: Post-intervention complications, recurrent symptoms less than one year, late recurrence of appendicitis more than one year, a quality-of-life evaluation, and several economic endpoints. Analysis was by intention-to-treat. A 94% success rate was assumed for the antibiotic agents group. A difference of 15 percentage points was considered clinically important. A sample size calculation, assuming a power of 0.8, a one-sided α of 0.05 (Fisher exact test), and a 10% dropout rate yielded a sample size of 142 patients (71 per group). Enrollment challenges acknowledged by the authors meant that only 66 evaluable patients were enrolled despite 3,783 patients being approached for participation. That sample size would have provided adequate statistical power only if the difference between groups was 25 percentage points. Thus, the study was substantially underpowered given the 10-day treatment success rate for antibiotic agents was 97% (95% confidence interval [CI], 92%–100%) and 87% (95% CI, 75%–99%) for placebo. 74
In summary, data are insufficient to determine the safety and efficacy of non-antibiotic therapy of uAA. This should be considered plausible, and a testable hypothesis.
Is Uncomplicated Acute Cholecystitis an Infectious Disease?
Acute calculous cholecystitis ranges in presentation across a spectrum of severity. There are several grading systems for describing the severity of cholecystitis, including the Tokyo Guidelines 2018 (TG18) diagnostic criteria and severity grading, 75 the American Association for the Surgery of Trauma grading scale, 76 and the Parkland Grading Scale for Cholecystitis 77 (Table 1). Although not accepted universally, the TG18 grading system is the only one to include physiologic parameters. Additionally, TG18 grades are utilized by many studies to define inclusion and exclusion criteria and by guidelines on the management of acute cholecystitis (Table 2), such as those from the Surgical Infection Society (SIS) 78 and the World Society of Emergency Surgery (WSES). 79 Severity ranges from TG18 grade 1 (mild) where there is no evidence of marked local or systemic inflammation to grade 3 (severe), which is characterized by dysfunction of at least one organ system. Grade 1 ACC is considered uncomplicated (uACC).
Comparison of Components of Acute Cholecystitis Grading Systems
The Parkland Grading Scale includes only intra-operative findings. Both the Parkland Grading Scale and the AAST Grading Scale include only anatomic descriptions of acute cholecystitis, whereas the TG18 severity includes physiologic parameters.
Guidelines for Antibiotic Use in Acute Cholecystitis
The Tokyo Guidelines 2018 (TG18) and WSES guidelines discuss management of acute cholecystitis in general, whereas the SIS guidelines focus on antibiotic use specifically in patients undergoing cholecystectomy.
In considering whether or not uACC is an infectious disease, there are two questions to consider. Do bacteria have a role in the disease process? And what is the impact of using or not using antibiotic agents on clinical outcomes? To address the first question, the pathophysiology of acute calculous cholecystitis should be considered. Initially, acute cystic duct obstruction occurs, leading to gallbladder wall inflammation and edema.80,81 Over time, the gallbladder wall can become hemorrhagic and ischemic, and may progress subsequently to gangrene or perforation. Infection is considered a secondary phenomenon. 81
Do bacteria have a role in uACC and does failure to treat bactibilia have any clinical consequences? The TG18 does not recommend bile or blood cultures for uACC, only for patients with grades 2 to 3 acute cholecystitis. 82 Even so, cultures are not always obtained routinely. In recent studies reporting culture results in patients with varying grades of acute cholecystitis, bactibilia was present in 35%–65% of bile cultures,83–85 compared with 7.7%–15.8% of positive blood cultures.86,87 However, the clinical relevance of bactibilia is unclear. Several retrospective studies have reported an association between positive bile cultures and post-operative infections,84,88 whereas another study reported no association. 85
Although early laparoscopic cholecystectomy is the standard of care for ACC, the WSES guidelines state that NOM includes fluids, analgesia, and antibiotic agents. Furthermore, the guidelines recommend antibiotic agents for patients who are refusing or not candidates for surgery. 79 This recommendation is in accord with clinical practice in which patients are often started on antibiotic agents on admission, regardless of disease severity. However, the quality of evidence is low and the strength of the recommendation is weak. The best available data are derived from a RCT by Mazeh et al. 89 who compared intravenous amoxicillin-clavulanic acid or ciprofloxacin plus metronidazole to best supportive care, followed by delayed laparoscopic cholecystectomy in 215 patients with uACC. The sample size was powered based on non-inferiority in the primary outcome of length of stay for the index admission with a margin of one day; there was no difference between groups in this outcome. All patients were scheduled for surgery, but more patients in the antibiotic agents group underwent cholecystectomy (86% vs. 62%; p = 0.02), or percutaneous cholecystostomy (PC; 12% vs. 5%; p = 0.43). Of note, among the patients who underwent surgery, all had bile cultures but only 18% had positive cultures. Similar numbers of patients had positive bile cultures in the antibiotic agent group (22% vs. 12%; p = 0.50). Thus, despite the guidelines and clinical practice, this trial does not support antibiotic use in NOM of uACC.
Does antibiotic use have an impact on clinical outcomes when used in combination with laparoscopic cholecystectomy? Pre-operative antibiotic prophylaxis is recommended by the SIS for patients undergoing laparoscopic cholecystectomy for acute cholecystitis. 78 This recommendation is based on current practice and TG18. Furthermore, a large body of evidence demonstrates that antibiotic prophylaxis is effective in reducing surgical site infections (SSIs) after clean-contaminated (class 2) procedures (e.g., laparoscopic appendectomy or cholecystectomy for uAA or uACC, respectively), and moreover that the relative risk is consistent across levels of contamination. 90 The implication is that the absolute risk reduction with antibiotic prophylaxis increases with the baseline risk of SSI of the procedure. Since the publication of the SIS guidelines, disease-specific data have become available in the form of the Perioperative Antibiotic Prophylaxis in the Treatment of Acute Cholecystitis (PEANUTS II) trial. 91 This was a multicenter non-inferiority RCT that randomized patients with mild-to-moderate ACC requiring immediate cholecystectomy to preoperative cefazolin or no antibiotic. The incidences of 30-day infections in the no antibiotic group (12.6% vs. 7.1%) were within the 10% margin of the 95% confidence interval, therefore the results were not statistically significant (absolute difference, 5.5%; 95% CI, −0.4% to 11.3%). Of note, approximately 60% of the patients enrolled in this trial had grade 1 cholecystitis (uACC), and 45% of patients who had bile cultures had bactibilia (similar between groups). In post hoc subgroup analyses, there were no differences in treatment effect based on severity or bile culture results. Based on the trial, antibiotic agents should not be administered therapeutically prior to laparoscopic cholecystectomy for mild-to-moderate acute cholecystitis, but is indicated for incisional prophylaxis only.
Whereas pre-operative antibiotic agents are recommended, there is no role for post-operative antibiotic agents in patients with mild cholecystitis after cholecystectomy. Hajibandeh et al. 92 performed a systematic review and meta-analysis of extended post-operative antibiotic agents versus no post-operative antibiotic in patients undergoing emergency cholecystectomy for ACC. They defined extended post-operative antibiotic agents as three or more doses of antibiotic agents, any type or dose, after emergency cholecystectomy. Based on four RCTs that included 953 patients, there were no differences in any infectious or non-infectious complications. In particular, extended post-operative antibiotic use was not associated with decreased odds of SSI (odds ratio [OR], 1.13; 95% CI, 0.58–2.18) or infectious complications overall (OR, 0.94; 95% CI, 0.62–1.44). In accord with the findings of the meta-analysis, the SIS guidelines recommend against the use of post-operative antibiotic agents in patients undergoing laparoscopic cholecystectomy for mild-to-moderate acute cholecystitis. 78 This recommendation also holds for patients who undergo conversion from laparoscopic to open cholecystectomy for uACC. 78
Does antibiotic use have an impact on clinical outcomes when used in combination with PC? There are limited data to guide recommendations. In general, patients with uACC are not treated by PC. However, a retrospective study by Wang et al. 93 suggested that in patients with mild-to-moderate ACC not undergoing surgery, antibiotic agents plus PC may be associated with greater short- and long-term treatment success compared with antibiotic agents alone. These results should be interpreted cautiously given the inherent bias of retrospective studies. Nonetheless, PC tends to be reserved for patients who are poor surgical candidates because of organ dysfunction, severe disease, 79 or comorbidities. 78 Because PC is used primarily in high-risk patients, there are no relevant RCTs of antibiotic agents versus no antibiotic agents. A retrospective study by Loftus et al. 94 reported that outcomes were similar with a short (≤ 7 days) versus long course (> 7 days) of antibiotic agent(s) in patients with PCs. Further study is needed regarding antibiotic use in high-risk patients with mild cholecystitis undergoing PC.
The primary limitation to this literature is that there are no RCTs comparing antibiotic agents with no antibiotic agents for uACC treated solely with NOM. A challenge to conducting such a trial is that biliary colic is often difficult to distinguish from uACC, and there may be differences in degree of inflammation and in prevalence of bactibilia based on clinical diagnosis alone. Enrollment of patients with biliary colic only, without acute inflammation, would increase the sample size requirement of such a trial (given an expected bias towards a null effect). The existing literature includes patients with both uACC and moderate ACC who have undergone a subsequent cholecystectomy. Even though antibiotic agents are recommended for moderate ACC, there was no reported benefit to pre- and post-operative therapeutic antibiotic agents. These trials provide indirect evidence in support of restraint in antibiotic treatment for uACC.
In summary, based on pathophysiology, uACC is not primarily an infectious phenomenon. Even when bactibilia is present, there is no high-quality evidence to suggest that mild disease should be treated with therapeutic antibiotic agents. A single dose of pre-operative prophylaxis is indicated in uACC patients undergoing cholecystectomy, although the absolute risk reduction in 30-day infectious complications is modest.
Is Uncomplicated Mild Acute Diverticulitis an Infectious Disease?
Diverticulitis traditionally has been believed to be an infectious disease that requires treatment with antibiotic agents in all its manifestations. However, given recent understanding that alterations of the human microbiome can be related to inflammation that may not benefit from antibiotic treatment,95,96 researchers have begun to question whether less-severe forms of diverticulitis should be considered inflammatory diseases (i.e., caused by host responses) rather than infectious diseases (e.g., caused by bacterial pathogens). Currently, many episodes of diverticulitis are managed with antibiotic agents in the United States. However, in Europe there has been a recent move away from the use of antibiotic agents for the milder forms of diverticulitis, based on RCT evidence accumulated over a decade.
The Canadian surgeon E. John Hinchey first classified diverticulitis in 1978 (Table 3). 97 Hinchey type I diverticulitis included small, localized infections. Type II included larger abscesses that required local debridement and wide drainage. Type III included diverticulitis that was severe enough to have a non-localized infection (macroscopic pus throughout the abdomen, not just limited to the pelvis.) Type IV diverticulitis included feculent peritonitis (frank stool throughout the abdomen). Development of this classification system coincided temporally with the availability of diagnostic CT.
Original and Modified Hinchey Classifications
CT = computed tomography; N/A = not applicable.
The Hinchey classification has been modified several times. Neff and von Sonnenberg 98 described a CT-based modification that includes a stage 0 (mild disease limited entirely to the colon wall). Over time, Hinchey type I disease has been separated into two categories that have been adopted clinically.99–101 Class Ia includes inflammation or a phlegmon of the colon alone, limited largely to the wall but with some extracolonic extension, even including localized extraluminal air but no fluid collections. Class Ib includes smaller abscesses (Fig. 4) that can be localized by CT. 100

Modified Hinchey classification of acute diverticulitis as it applies to computerized tomographic findings. (
Further modification of this system was proposed by the WSES (Table 3). 102 These subclassifications were made possible by ever-improving precision of CT. Stage 0, uncomplicated diverticulitis, includes inflamed diverticula alone with thickening of the colon wall or increased density of peri-colonic fat with no extraluminal extension. Stage 1a uncomplicated diverticulitis includes peri-colic air bubbles or a small amount of fluid within five centimeters of the bowel, without clear abscess formation. Stage 1b mild, complicated disease includes abscesses ≤4 cm. The WSES further subdivided stage 2 disease. Stage 2a disease includes an abscess >4 cm diameter, whereas stage 2b disease includes pneumoperitoneum >5 cm distant from the colon. Stage 3 includes diffuse fluid with no distant free air or colon perforation, whereas Stage 4 includes diffuse fluid, distant pneumoperitoneum, and a persistent perforation.
The first major trial to assess the possibility of treating mild diverticulitis without antibiotic agents, known as the AVOD (Antibiotika Vid Okomplicerad Divertikulit [Swedish for antibiotic agents in uncomplicated diverticulitis]) study, was published by Chabok et al. 103 in 2012. Adult patients were enrolled with abdominal pain and tenderness, an elevated white blood cell count or C-reactive protein, and diagnosis of diverticulitis based on CT. Complicated diverticulitis, including an abscess or pneumoperitoneum, was excluded. Six hundred twenty-three subjects were randomized to no antibiotic agents or intravenous antibiotic agents (with potential switch to oral agents) for at least seven days. Major outcomes included pain, fever, and tenderness score over time. There was no difference in outcomes between patients who received antibiotic agents or not. In addition, complications (including subsequent sigmoid perforation or abscess formation) were similar between groups, as was the necessity for sigmoid resection. Hospital length of stay was 2.9 days in each arm and the rate of recurrent diverticulitis was 16% in each group.
Daniels et al. 104 published the DIABOLO (DIverticulitis: AntiBiotic agents Or cLose Observation?) trial in 2017. Only stages 1a and 1b (allowing small, peri-colic abscesses) disease was included; 528 patients were randomly assigned to receive antibiotic agents (generally amoxicillin-clavulanic acid with potential for oral switch, 10-day minimum) or observation alone. Time to recovery was tracked; at six months there was no difference. Neither perforation, obstruction, bleeding, abscess formation, nor the incidences of any intervention differed between groups. In addition, the rates of ongoing diverticulitis were similar and the rate of recurrent diverticulitis within six months was 3% in each group.
Most recently, in 2021, the STAND (Selective Treatment with Antibiotic agents for Non-complicated Diverticulitis) study was reported from New Zealand and Australia. 105 Among 178 patients with Hinchey Ia disease randomized to placebo or antibiotic agents (intravenous/oral) for seven days, the hospital length of stay was similar at approximately four days each. Time to reduction in white blood cell count and pain score were also similar. Two patients in the antibiotic group and none in the placebo group required a procedural intervention, and the rates of seven- and 30-day reeadmission were similar: at seven days, placebo 1% and antibiotic agents 6%; at 30 days, placebo 11% and antibiotic agents 6%.
The question of whether patients with Hinchey Ib diverticulitis who have demonstrable extraluminal air (denoting true colonic perforation) behave differently has also been addressed. A subgroup analysis of the DIABOLO study 104 focused specifically on Hinchey Ib patients showed no difference in meaningful outcomes between those patients receiving antibiotic agents or not. 106 In fact, few patients ultimately required either emergency surgery or percutaneous drainage; those who did were in the original DIABOLO antibiotic treatment arm.
Long-term results have also been reported for patients in the aforementioned RCTs of antibiotic avoidance for diverticulitis. Two-year follow-up of the DIABOLO study 104 was published in 2018 by van Dijk et al. 107 ; no differences were found in the rates of recurrent diverticulitis or elective or emergency colectomy between patients who received antibiotic agents or observation alone during DIABOLO. Ten-year follow-up was published for the AVOD study 103 in 2019 by Isacson et al. 108 Even over 10 years, there was no difference in diverticulitis recurrence or complications, or a requirement for either emergency or planned surgery for diverticulitis. These findings strongly suggest that for umAD, antibiotic agents are unnecessary and do not change either short- or long-term outcomes.
Multiple meta-analyses of studies comparing use of antibiotic agents to no antibiotic agents in the management of mild diverticulitis have been published, including by Au et al. (2019), 109 Desai et al. (2019), 110 Mege et al. (2019), 111 and Van Dijk et al. (2020). 112 In each analysis, no differences in outcomes were found with the use of antimicrobial agents versus placebo for either umAD (Hinchey Ia) or mild complicated (Hinchey Ib) diverticulitis. Consensus guidelines have adopted these findings as recommendations. Hall et al., 113 writing for the American Society of Colon and Rectal Surgeons (ASCRS) in 2020, summarized guidelines for the management of diverticulitis. The authors, using Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology, concluded, “Selected patients with uncomplicated diverticulitis can be treated without antibiotic agents. Grade of Recommendation: Strong recommendation based on high-quality evidence, 1A.” Also focusing on diverticulitis, Peery et al. 114 published the American Gastroenterological Association (AGA) Clinical Practice Updates 2021. These expert opinion-based updates noted, “Antibiotic treatment can be used selectively, rather than routinely, in immunocompetent patients with mild uncomplicated diverticulitis.” Furthermore, the authors commented on patients who should receive antimicrobial agents in the setting of uncomplicated diverticulitis, stating “Antibiotic treatment is advised in patients with uncomplicated diverticulitis who have comorbidities or are frail, who present with refractory symptoms or vomiting, or who have a C-reactive protein >140 mg/L or baseline white blood cell count >15 × 109 cells/L. Antibiotic treatment is advised in patients with complicated diverticulitis or uncomplicated diverticulitis with a fluid collection or longer segment of inflammation on CT scan.” Although not defined precisely, it is plausible that the perception of frailty in an individual patient is the most common reason for starting antimicrobials for truly mild disease, but elderly, frail patients may be at high risk for complications therefrom. 115
Although the data regarding the non-antibiotic management of umAD are solid, there are still some limitations. Given the natural propensity to not enroll patients with more severe disease in clinical trials, it is possible that the above studies excluded patients with limited disease by CT, but a more worrisome clinical picture based on examination. Second, prior studies did not require follow-up imaging, so some number of subjects may have had abdominal pain from a non-diverticular cause superimposed on stable, uninflamed diverticulosis coli. Finally, to identify patients accurately who will fail treatment with or without antimicrobial agents for umAD may require advancements in imaging technology, alternative biomarkers, and genomics/personalized medicine.
In summary, mild diverticulitis, generally Hinchey Ia or Ib in current nomenclature, does not appear to benefit from antimicrobial agents based on clinical studies. The implication is that this disease is not an infection but localized inflammation. Non-antimicrobial management is reasonable. More severe disease does require antibiotic agents and potentially surgical or other forms of intervention.
Discussion
Among the considered disease entities, the evidence is arguably strongest that umAD is not an infectious disease and can be treated without antibiotic agents, strong but indirect regarding uACC, and lacking for uAA. There is evidence that the gut microbiome is altered in sepsis. 116 Whether such alterations are causal or consequential is debatable; the interactions between the microbiome and the inflammasome have been referred to as a vicious cycle. 117 Although uACC is associated with ischemia 118 and prostanoid-mediated inflammation, 119 and bacterial invasion is believed to be a secondary phenomenon, 81 recent metagenomic studies indicate the presence of a lush biliary microbiome120,121; indeed, bacteria have been implicated in the pathogenesis of gallstones. 122 Alterations of the gut microbiome have been described in both uAA and umAD.68,123
Considering umAD, for which the evidence is most robust, if one accepts results that that antibiotic therapy does not alter the outcomes of umAD, one must consider alternative pathophysiologic hypotheses. Diverticulitis, for which the evidence is strongest, is clearly an inflammatory disease that occurs in the setting of diverticulosis coli. Given the immediate presence of the dense, diverse colonic microbiome, bacteria and other micro-organisms are certainly involved, but most likely not always in the standard sense of disease pathogenesis (infection). Considering that umAD generally resolves on its own without antimicrobial therapy, a plausible hypothesis is that the inflammation that causes symptomatic umAD is related to a disturbance of the normal colonic microbiome, resulting in dysbiosis, which is defined as an imbalance of micro-organisms present in a person's natural microflora, especially that of the gut, believed to contribute to a range of conditions of ill health.
Indeed, O'Grady et al. 123 demonstrated a loss of diversity and other evidence of dysbiosis in patients with diverticulitis compared with healthy controls. Although unproved, restoration of a normal non-pathogenic microbiome could explain resolution of umAD without antibiotic therapy.124,125 If dysbiosis is at the core of the pathogenesis of umAD, one could posit that prebiotics, probiotics, or synbiotics would be effective, either as prophylaxis or for the treatment of umAD. In 2016, Lahner et al. 126 performed a systematic review of extant data regarding the use of probiotics in the management of diverticular disease, and found the results inconclusive. More recently, Ojetti et al. 127 published an RCT of the efficacy of the probiotic Limosilactobacillus reuteri ATCC PTA 4659 in the treatment of umAD. Patients were randomly assigned to probiotic therapy or placebo. Resolution of pain occurred within seven days in both groups, but the group receiving the probiotic had a greater decrease in C-reactive protein than did the placebo group.
In terms of prevention, evidence is lacking for the use of prebiotics, probiotics, or synbiotics. However, from an epidemiologic standpoint, consumption of a high-fiber diet, likely producing a prebiotic effect, 128 is associated with lower rates of diverticulosis, and by association diverticulitis. Further studies are necessary to determine if increased consumption of fiber or probiotics is associated with a lower incidence of diverticulitis.
Diverticulitis coli results in an estimated 300,000 hospital admissions per year in the United States and the incidence is increasing. 129 Are there valid reasons to continue to use antibiotic agents in umAD? Conceivably, progression of Hinchey Ia or Ib diverticulitis to more extensive disease could be prevented with antimicrobial agents. Frailty and medical comorbidities are also common among patients presenting with diverticulitis, and, at least according to the AGA, should receive antibiotic agents, as should patients with immunocompromise or signs of sepsis. 114 Finally, public perception continues to expect antimicrobial treatment for all forms of diverticulitis, an attitude that will not change rapidly. 130 As a result, it may be impossible to reassure patients sufficiently that antimicrobial agents are not necessary for umAD. As for prebiotic or probiotic therapy, no current recommendation can be made in terms of treatment, but it is not recommended for prevention of recurrent disease. 114
Footnotes
Funding Information
No funding was received for this project.
Author Disclosure Statement
The authors have nothing to disclose.