
Abstract
Background:
Longitudinal rates, risk factors, and costs of superficial and deep incisional surgical site infection (SSI) were evaluated six months after primary total hip arthroplasty (pTHA) and revision total hip replacement (rTHA).
Patients and Methods:
Patients who had pTHA or rTHA between January 1, 2016 and March 31, 2018 were identified using the IBM® MarketScan® administrative claims databases. Kaplan-Meier survival curves evaluated time to SSI over six months. Cox proportional hazard models evaluated SSI risk factors. Generalized linear models estimated SSI costs up to 12 months.
Results:
The total cohort included 17,514 pTHA patients (mean [standard deviation] age 59.6 [10.1] years, 50.2% female; 66.4% commercial insurance), and 2,954 rTHA patients (61.2 [12.0] years, 52.0% female; 48.6% commercial insurance). Deep and superficial post-operative SSI at six months affected 0.30% (95% confidence interval [CI], 0.22%–0.39%) and 0.67% (95% CI, 0.55%–0.79% of patients in the pTHA, and 8.9% (95%CI: 7.8%–10.0%) and 4.8% (95% CI, 4.0%–5.6%) of patients in the rTHA cohorts. Hazards for SSI were related to patient comorbidities that included diabetes mellitus, obesity, renal failure, pulmonary or circulatory disorders, and depression. The adjusted average all-cause incremental commercial costs associated with post-operative infection ranged from $21,434 to $42,879 for superficial incisional SSI and $53,884 to $76,472 for deep incisional SSI, over a 12-month post-operative assessment period.
Conclusions:
The SSI rate after revision total hip arthroplasty (rTHA) was nearly 9% compared with 1.0% after pTHA. The risk of infection was influenced by several comorbid risk factors. The incremental cost associated with SSIs was substantial.
More than 300,000 hip replacement procedures are undertaken annually in the United States1–3 and this number is expected to increase by 2030 with an ageing population and an increasing prevalence of arthritis.4–6 Although total hip arthroplasty (THA) is effective in improving quality of life, with low morbidity and mortality, post-operative infection poses a substantial, and expensive, complication. Peri-prosthetic joint infections (PJI) have four inter-related risk factors including bacterial virulence and antimicrobial resistance; multiple patient comorbidities; intra-operative factors that include the peri-operative surgical team, operative technique, and the operating room environment; and post-operative care and wound management. Although superficial incisional surgical site infections (SSIs) may be amenable to local wound treatment with debridement, antiseptic dressings, and antibiotic therapy, infection may extend beyond the subcutaneous layer to involve deeper tissue layers and leading to a PJI. Management of a PJI necessitates the interdisciplinary coordination of surgical and often prolonged antimicrobial therapy, and in the case of treatment failure, device removal.6,7
The incidence of SSI after primary and revision (pTHA and rTHA) total hip arthroplasty ranges from 0.4% to 8.6%, depending upon the patient population, type of surgical procedure, and the definition of SSI.8–10 In an earlier analysis of 163,547 THAs we reported that SSI rates were 8.6% for rTHA compared with 2.1% for pTHA. Comorbidities that had the greatest impact on SSI after rTHA were metastatic cancer, congestive heart failure, blood loss anemia, coagulopathy, weight loss, alcohol abuse, deficiency anemia, obesity, uncontrolled hypertension, diabetes mellitus, and fluid electrolyte disorder. 11 The purpose of the current study was to build upon these findings by conducting a longer duration (180 days) longitudinal analysis, using the same database, to determine more accurately the time of SSI presentation after rTHA, if associated risk factors differed in relation to the time of SSI presentation, and the all-cause incremental costs from the perspective of commercial payers for pTHA and rTHA associated with superficial and deep incisional SSI.
Patients and Methods
Data sources
The current analysis represents a retrospective cohort study using the IBM® MarketScan® (Ann Arbor, MI, USA) Commercial Claims and Encounters (CCAE), Medicare Supplemental and Coordination of Benefits (MDCR), and Multi-State Medicaid (MDCD) databases. The CCAE contains information on individuals who are under the age of 65 and are the primary insured, spouse, or dependent. The Medicare database includes information for individuals who are 65 years or older and are Medicare eligible with supplemental insurance being paid for by their current or former employer. Data for the CCAE and Medicare databases are collected from more than 300 large, self-insured U.S. employers and more than 25 U.S. health plans. The Medicaid database contains data from more than 48 million Medicaid enrollees from multiple states. The databases comprise enrollment information, demographics, and adjudicated health insurance claims (e.g., inpatient, outpatient, and outpatient pharmacy).
The use of IBM databases has been reviewed by the New England Institutional Review Board (IRB) and determined to be exempt from broad IRB approval. All data within these databases are de-identified and comply with Health Insurance Portability and Accountability Act (HIPAA) regulations (45 CFR 160, 162, and 164).
These databases consist of three files: an enrollment file, which includes patient sociodemographic and health insurance payer type information; a medical file, which includes detailed records for hospital inpatient and outpatient admissions and services across different facilities of care captured with an international classification of disease (International Classification of Diseases [ICD]-9 and ICD-10 diagnosis), involving clinical modification (CM) and procedure coding system (PCS) codes and Common Procedural Terminology (CPT) codes; and a drug file, which includes pharmacy claims. The files are linkable, based on encrypted patient identification numbers.
Patient population
Patients in the database who underwent pTHA or rTHA (identified using ICD-10-PCS codes or CPT-4 codes) between January 1, 2016, and March 31, 2018, in either outpatient or inpatient settings of care were considered for inclusion. The date of hospitalization for THA was defined as the index date. Patients were included if they were 18 or older and continuously enrolled for at least 12 months before and 180 days after index THA. Patients were excluded if a knee procedure had been performed 12 months pre-index THA to two years post-index THA, a contralateral hip procedure had been performed within six months of index, or a femoral fracture was present at time of index surgery. These exclusions were designed to avoid including other potential sources of SSI in the analyses.
Outcomes evaluated
The occurrence of SSI within 180 days after pTHA or rTHA was evaluated using ICD-10-CM and CPT codes (Supplementary Table S1). An inclusive list of identified comorbid risk factors (Elixhauser Comorbidity Index [ECI]) in the pTHA and rTHA patient populations is documented in Supplementary Table S2. The ECI estimates an aggregate measure of comorbidity using 31 dimensions and has been shown to be associated with risk of mortality and health care utilization.12,13 The primary outcome was the occurrence of deep incisional SSI from two to 180 days post-operatively. Secondary outcomes included the occurrence of superficial incisional SSI, and incremental, all-cause healthcare costs associated with SSIs, evaluated from the perspective of the insurer at six and 12 months post-index procedure. For the evaluation of deep incisional SSI after rTHA, a subgroup analysis was conducted to analyze the occurrence of deep infection from two to 180 days post-operatively, excluding patients with a diagnosis of deep incisional infection up to one year prior to the rTHA. This subgroup analysis was designed to evaluate the risk of deep incisional infection in patients having their hip replacement revised for non-infection–related causes.
Statistical analyses
Descriptive statistics including means and standard deviations for all continuous variables and proportions for categorical variables were performed to describe all variables in the dataset. Analyses were performed separately for pTHA and rTHA patients. Time to superficial and deep incisional SSI over six months was represented with Kaplan-Meier survival curves. Cox proportional hazard models examined the effects of pre-operative patient characteristics (demographics and pre-existing comorbid factors) and surgical characteristics (year of surgery) on the hazard of superficial or deep incisional SSI. Hazard ratios, 95% confidence intervals, and p values were computed. Generalized linear models with gamma distribution and log links estimated the adjusted all-cause incremental cost of superficial and deep incisional SSI. All costs were adjusted to 2021 U.S. dollars using the Bureau of Labor Statistics (BLS) consumer price index. 14
Results
Patient baseline demographic and overall risk index
A total of 17,514 pTHA patients and 2,954 rTHA patients were included in the analyses. The baseline demographic characteristics included age, gender, risk index, and health insurance type (i.e., commercial, Medicare, or Medicaid) is presented in Table 1. Females accounted for 50.2% and 52.0% of patients in the primary and revision arthroplasty cohort groups, respectively. Two-thirds of pTHA patients had commercial insurance (66.4%), the remainder had Medicare (18.8%) or Medicaid (14.9%) insurance, whereas 48.6% of rTHA patients had commercial insurance; Medicare or Medicaid coverage was approximately 25% each. Overall, the mean (standard deviation [SD]) ECI scores were higher among patients with rTHA (3.6 [2.7]) compared with patients in the pTHA cohort (2.1 [1.9]). Compared with pTHA, patients in the rTHA cohort were also more likely to have an ECI of five or greater (pTHA: 10.2 vs. rTHA: 29.9).
Overall Baseline Demographics, Insurance Coverage, ECI, and Age Category for Patient Population Undergoing Primary and Revision THA
ECI = Elixhauser Comorbidity Index; SD = standard deviation; pTHA = primary total hip arthroplasty; rTHA = revision total hip arthroplasty.
Superficial and deep incisional SSI rates and timing
Subgroup analyses of primary and revision THAs for deep, superficial and no infection cohorts is reported in Table 2. No difference in patient age was observed in the superficial, deep, or no infection categories in both pTHA and and rTHA. The mean ECI score for deep pTHA/rTHA infections was greater than the value reported for superfical pTHA/rTHA infections. All key comorbid risk factors were more prevalent in the rTHA patient population compared with the pTHA cohort. For example, in those pTHA patients presenting with deep infection, complicated hypertension, obesity, cardiac arrhythmia, chronic pulmonary disease including asthma and fluid and electrolyte disorders were documented in 7.5%, 34.0%, 26.4%, 24.5%, and 11.3% of patients compared with the respective findings in the rTHA patient cohort: 18.3%, 38.6%, 34.7%,37.8%, and 36.3% (Table 3). As expected, chronic comordid conditions were far more prevalent in the superficial and deep incisional SSI cohort groups compared with the no-infection patient population.
Baseline Demographics of Patients, ECI Category of pTHA and rTHA in Deep, Superficial, and No Infection Cohort Groups
ECI = Elixhauser Comorbidity Index; SD = standard deviation; SSI = surgical site infection; pTHA = primary total hip arthroplasty; rTHA = revision total hip arthroplasty.
Key Comorbidities of Patients with pTHA or rTHA Based on Post-Operative Infection Status
ECI (Elix) = Elixhauser Comorbidity Index; SSI = surgical site infection; pTHA = primary total hip arthroplasty; rTHA = revision total hip arthroplasty.
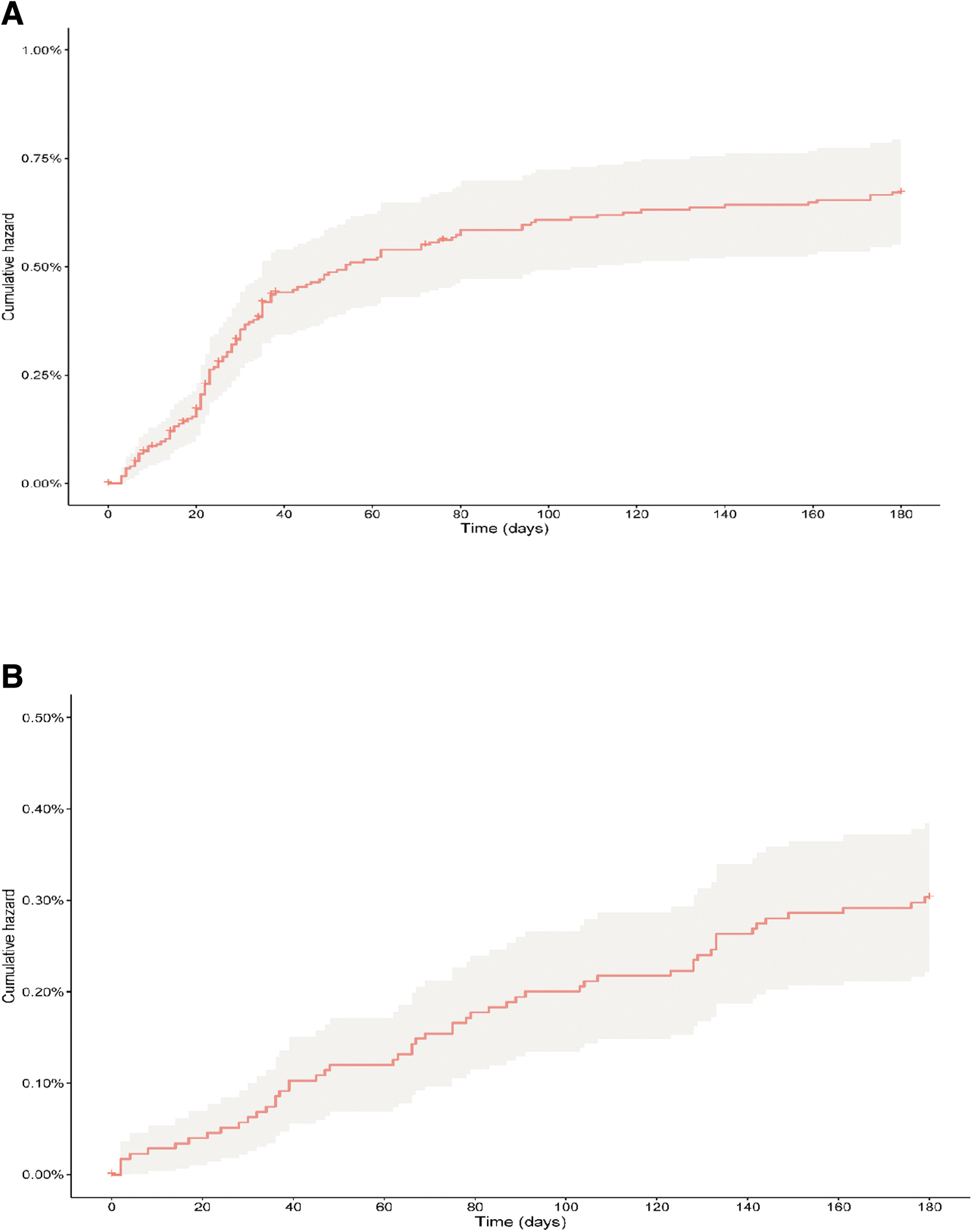
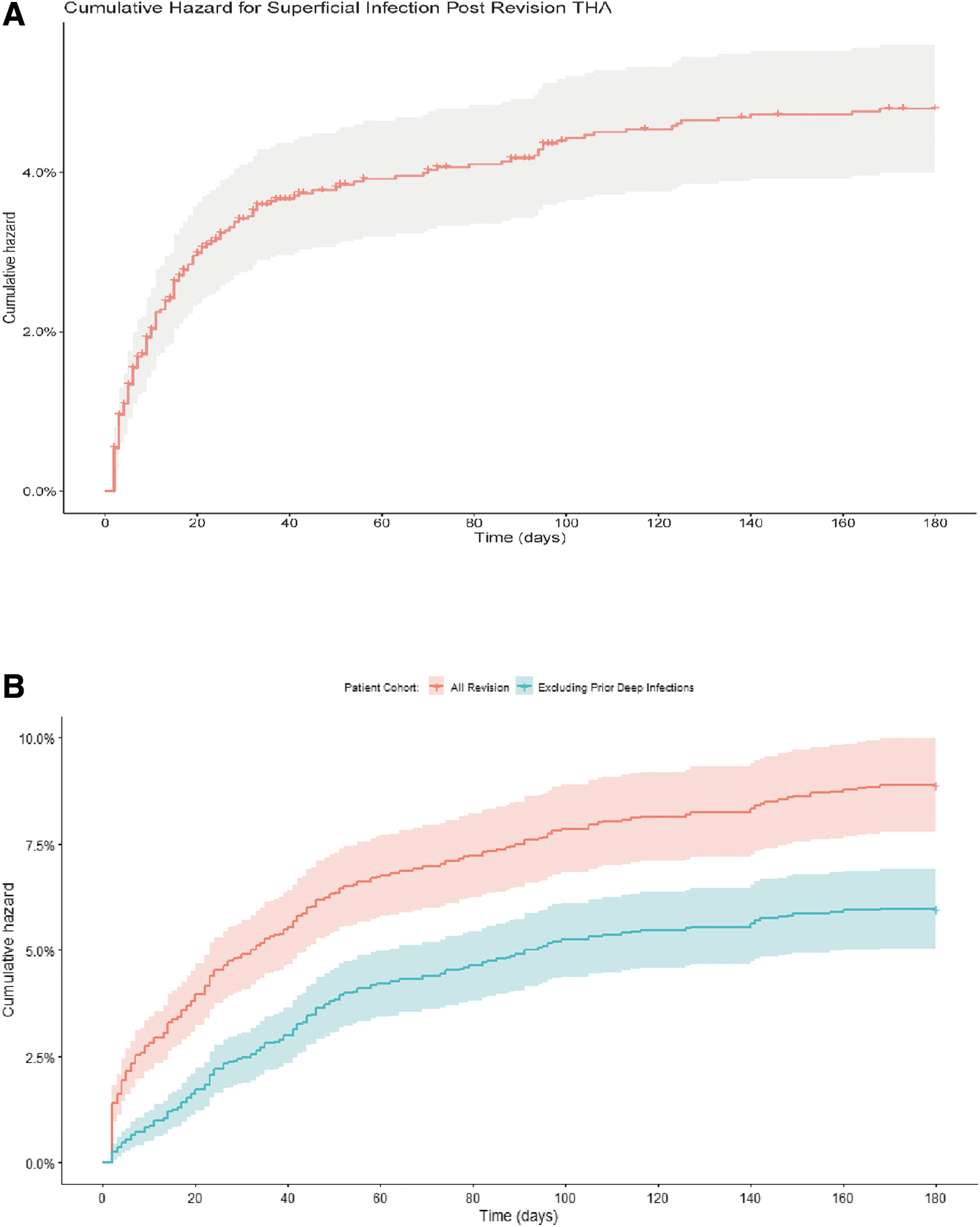
At six-months post-pTHA deep and superficial incisional SSI affected 0.30% (95% CI, 0.22%–0.39%) and 0.67% (95% CI, 0.55%–0.79%) of patients (Fig. 1A and 1B). The cumulative hazard for superficial pTHA appears to plateau around day 40. However, in the deep infection pTHA cohort the findings suggest that the increase in risk extends beyond 180 days post-operatively. In the rTHA cohort population, deep and incisional SSI affected 8.9% (95% CI, 7.8%–10.0%) and 4.8% (95% CI, 4.0%–5.6%) of patients (Fig. 2A and 2B). In a subgroup analysis, patients having rTHA who did not have an infection at time of revision, the rate of deep incisional SSI reached 6.0% (95% CI, 5.1%–6.9; Fig. 2B).
Patient characteristics associated with SSIs
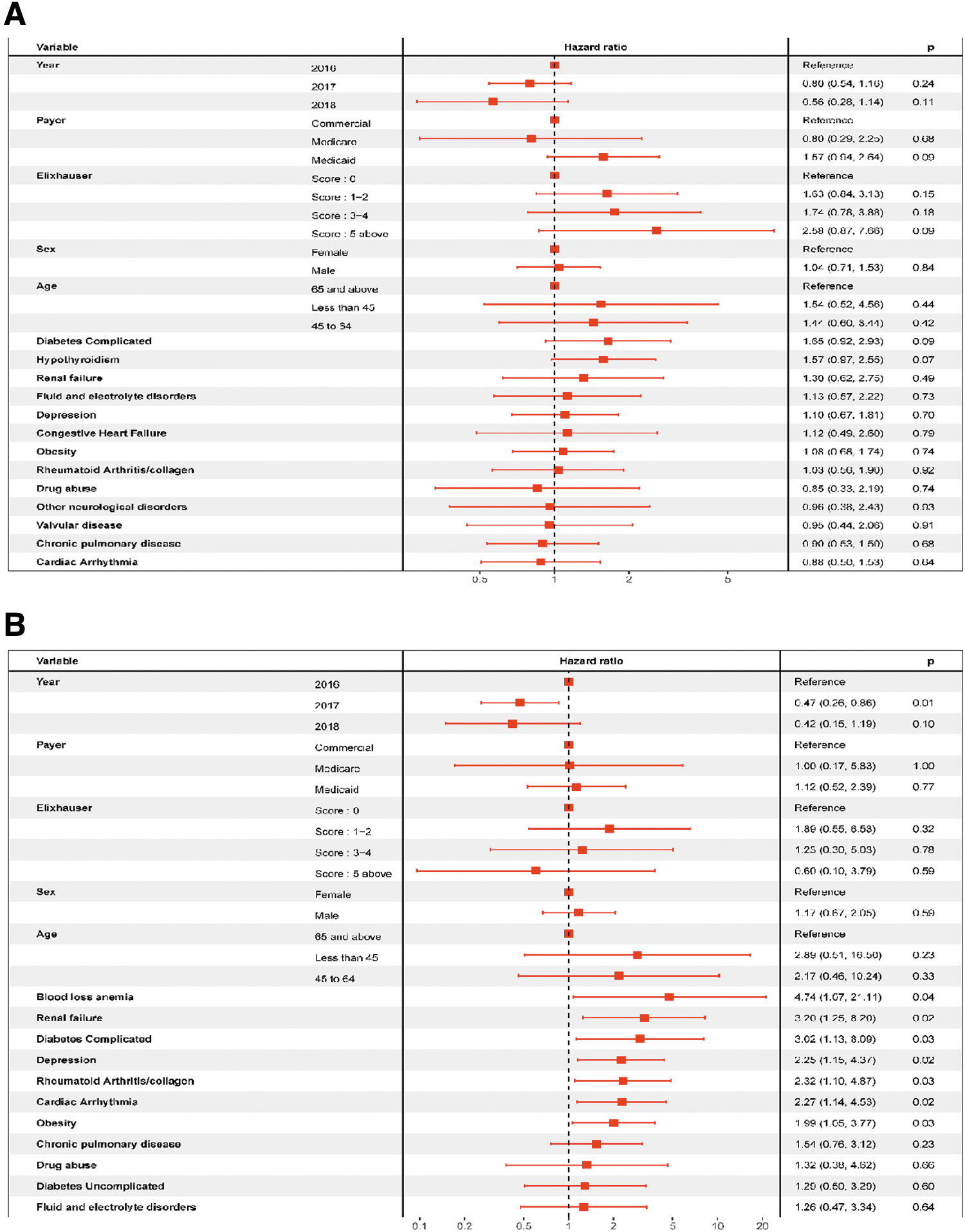
Forest plots of hazard ratios for deep and superficial incisional SSI after primary and revision THA are shown in Figure 3A and 3B and Figure 4A and 4B. None of the patient demographic or comorbidities at time of pTHA was strongly associated with an increased hazard for superficial SSI (Fig. 3A). Patients on Medicaid had a slightly increased, but non-significant hazard for superficial SSIs. The hazard ratios for Medicaid versus commercially-insured patients was 1.57 (95% CI, 0.94–2.64). The hazard ratios for superficial infections also increased with increasing ECI, but even for patients with an ECI score of five or above, the hazard ratio was not significant (hazard ratio [HR], 2.58; 95% CI, 0.87–7.66). Complicated diabetes mellitus and hypothyroidism had non-significant, but elevated hazard ratios (complicated diabetes: HR, 1.65; 95% CI, 0.92–2.93; hypothyroidism: HR, 1.57; 95% CI, 0.97–2.55). The hazard ratio for deep SSI after pTHA are shown in Figure 3B. Unlike superficial SSI, many comorbidities were associated with increased risk of deep incisional SSI: blood loss anemia (HR, 4.74; 95% CI, 1.07–21.11), renal failure (HR, 3.20; 95% CI, 1.25–8.20), complicated diabetes mellitus (HR, 3.02; 95% CI, 1.13–8.09), depression (HR, 2.25; 95% CI, 1.15–4.37), rheumatoid arthritis (HR, 2.32; 95% CI, 1.10–4.87), cardiac arrythmia (HR, 2.27; 95% CI, 1.14–4.53), and obesity (HR, 1.99; 95% CI, 1.05–3.77).

For patients undergoing rTHA few variables demonstrated an association for superficial SSI, However, coagulopathy (HR, 1.86; 95% CI, 1.05–3.27) and obesity (HR, 1.47; 95% CI, 1.01–2.16) did document an association for development of a superficial SSI. All other comorbidities or demographic factors were not associated with increased hazards for superficial infection (Fig. 4A). Comorbidities were linked with deep incisional SSI after rTHA (Fig. 4B). Patients with an ECI of five or above had an HR of 3.76 (95% CI, 1.47–9.62). Individual comorbidities, associated with increased hazard for deep incisional SSI after rTHA included fluid and electrolyte disorders (HR, 1.84; 95% CI, 1.37–2.49), complicated diabetes (HR, 1.48; 95% CI, 1.07–2.03), pulmonary circulation disorders (HR, 1.67; 95% CI, 1.08–2.58), and obesity (HR,1.34; (95% CI, 1.01–1.77).
Costs associated with SSIs
Adjusted all-cause incremental cost (payments) associated with management of superficial and deep incisional SSIs, compared with patients not having an SSI, were available for patients with commercial insurance over six and 12 months post-pTHA/rTHA. For patients having pTHA, the following average incremental cost of care were incurred when infection was reported: superficial incisional SSI, six-month costs $21,434 (95% CI, $8,615–$34,252) and 12-month costs $34,958 (95% CI, $11,163–$58,753); deep incisional SSI: six-month costs $54,521 (95% CI, $7,093–$101,949) and 12-month costs $76,472 (95% CI, $4,927–$148,017). For patients with rTHA, the costs were as follows: superficial SSI six-month costs $38,519 (95% CI, $13,845–$63,192) and 12-month costs $42,879 (95% CI, $15,575–$70,184); deep incisional SSI: six-month costs $53,884 (95% CI, $29,636–$78,131) and 12-month costs $55,605 (95% CI, $21,516–$89,695).
Discussion
The current analysis found that incisional SSI, both deep and superficial, occurred more commonly after rTHA compared with pTHA. Although patients with pTHA had a low risk of deep (0.3%) and superficial incisional SSI (0.6%), patients with rTHA had a higher risk of deep (8.9%) and superfical (4.8%) SSIs. The rates of SSI after rTHA observed in this study were higher than those of our previously published analysis, which found that SSI rates were 8.6% after rTHA and 2.1% after pTHA. 11 The differences in rates of SSI may be due to the inclusion of Medicaid patients in this study, the differences in timing of data collection, and the differences in duration of follow-up for the studies. Pre-operative patient optimization is recommended prior to total joint replacement for high-risk patients because it can decrease SSI risk as well as improving surgical outcomes and patient care.15–17
This analysis demonstrates that risk factors for SSI were related to patient comorbidities, including diabetes mellitus, obesity, renal failure, and pulmonary circulatory disorders. Although these results suggest a relatively small number of factors related to adverse patient outcomes, they are consistent with our previous analyses of the comorbidities associated with THA SSI. 11
The current study also found that a pTHA conducted in 2017 (compared with 2016) was associated with a lower risk of deep incisional SSI. There was also a trend for lower risk of deep SSI in 2018, but the difference was not statistically significant, presumably due to the smaller sample size studied in 2018 because only patients after THA within the first three months of the year were included to enable adequate follow-up data post-THA. The findings of a decreasing trend of SSIs in more recent years are consistent with a recent study evaluating SSI with rTHA using the National Surgical Quality Improvement Program (NSQIP) database. 18 There was a trend toward decreasing SSIs nationwide between 2011 and 2016, again emphasizing the benefits from pre- and post-operative infection prophylactic strategies. 18 Deep incisional SSI rates also reflected a marked improvement, specifically between 2014 and 2016. 18 However, these findings may also be due to changes in coding practices or documentation of infection as hospital infection rates are more closely scrutinized. 19 Furthermore, Medicare non-payment penalties have been instituted in an effort to reduce the incidence of hospital-acquired infections, including selective SSI. 20
Finally, the current study suggested that male gender was associated with an increased risk of deep SSI after rTHA. The reason for this finding is unclear but aligns with findings from other studies, including our prior investigation.10,11,21,22 It is also possible that male gender is linked to other unmeasured variables and that these results are confounded.
The choice between using logistic regression models or Cox proportional hazards models for epidemiologic association studies is primarily based on the design of the study. Cox proportional hazards models are the recommended models if follow-up data are available because they have more statistical power than logistic regression models and take account of the time until events occur. 23 To our knowledge, no other study has compared these models in determing the factors associated with incisional SSI after THA.
The analysis also found that the adjusted average all-cause incremental cost associated with SSI is substantial. The adjusted average all-cause incremental commercial costs ranged from $21,434 to $42,879 for superficial incisional SSI and $53,884 to $76,472 for deep incisional SSI, varying with the time horizon. A substantial proportion of the costs were incurred by six months but costs did increase from six to 12 months. We focused our cost analysis on the commercial cohort for multiple reasons; the Medicare database does not include all Medicare-eligible patients, only those with supplemental insurance provided by the workers' employers. Medicaid data are provided by a small proportion of U.S. states varying from year to year, and may be subject to delayed reimbursement.
The present analysis evaluated, within a real-world setting, the risk of SSI after pTHA and rTHA. The study used an administrative claims database, enabling a robust analysis of large numbers of patients. However, the results of the study must also be seen in light of its limitations, including that the observational design makes it difficult to draw causal inferences. Potential coding errors and misclassifications within the databases could not be identified and results may therefore lead to under-reported or missing diagnoses based on patients' choice (not to seek care) or access challenges that could not be captured. The findings from this database study are generalizable to similar populations with pTHA and rTHA and evaluated the risk of all-cause revisions only and did not analyze the specific cause for the revision.
Although this real-world data study found that SSI occurred most commonly after rTHA compared with pTHA and among patients with comorbid risks including diabetes mellitus, obesity, renal failure, and pulmonary circulatory disorders. The present analyses also suggests that our traditional healthcare surveillance strategies (i.e., CDC-NHSN or ACS-NSQIP) that collected data within a 30-day time period would likely miss a number of these post-operative infections that occur (detected) beyond this period of time. Therefore, underestimating the personal and fiscal impact to both the patient and the healthcare system in general.
Conclusions
Although orthopedic (device-related) infections represent a substantial cost to patients and healthcare systems, the implementation of evidence-based interventional care bundles have been shown to mitigate THA infections. An effective orthopedic surgical SSI care bundle must be scientifically sound (representing level 1A evidence base), supported by peer review and appropriate governmental bodies and associations, and free of dogmatic surgical practice. One systematic review has shown that introduction of a surgical care bundle was effective in reducing Staphylococcus aureus infections after major cardiac and orthopedic procedures. 24 A recent large cohort analysis has documented the clinical efficacy of a four-component surgical care bundle in improving the clinical outcome of THA. 25 An enhanced recovery after surgery (ERAS) protocol has been documented in a systematic review and meta-analysis to reduce the length of stay and incidence of complications in patients undergoing THA. 26 Therefore, in light of the increase in the projected number of hip arthroplasty procedures over the next 10 years, experience has shown that a prioritized institutional and staff commitment is required to implement a focused evidence-based strategies, improving the clinical outcome of selective surgical (orthopedic) patient populations. 27
Footnotes
Authors' Contributions
Conceptualization: Edmiston, Holy. Writing: Edmiston, Spencer, Leaper, Holy. Review: Edmiston, Spencer, Leaper, Gunja, Holy, Ruppenkamp. Editing: Edmiston, Spencer, Leaper, Gunja, Holy, Ruppenkamp. Statistical analysis: Holy. Statistics: Ruppenkamp. Final draft approval: Edmiston, Spencer, Leaper, Gunja, Holy, Ruppenkamp.
Funding Information
No funding was received.
Author Disclosure Statement
Dr. Edmiston, Ms. Spencer, and Dr. Leaper are members of the Ethicon Speakers Bureau; Dr. Gunja, Dr. Holy, and Ms. Ruppenkamp are employed by Johnson and Johnson, Inc. Dr. Edmiston, Ms. Spencer, and Dr. Leaper received no funding for this project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.