
Abstract
Background:
The literature regarding alterations in the coagulation profile in pediatric acute appendicitis (PAA) is scarce and mainly limited to retrospective studies. Evidence on the diagnostic yield of coagulation parameters is limited to fibrinogen.
Patients and Methods:
This is a prospective study with 151 patients divided into two groups: patients with nonsurgical abdominal pain (NSAP) in whom the diagnosis of PAA was excluded (n = 53) and patients with a confirmed diagnosis of PAA (n = 98). In 93 patients (62%), a coagulation study was obtained at the time of diagnosis and international normalized ratio (INR), activated partial thromboplastin time (aPTT),
Results:
Patients with NSAP had lower median levels of INR, fibrinogen and
Conclusions:
This study found a moderate extrinsic pathway coagulopathy in patients with PAA, especially in complicated PAA. Fibrinogen is a parameter with moderate diagnostic yield for the diagnosis of PAA.
Pediatric acute appendicitis (PAA) is the most prevalent surgical abdominal pathology in the world, with a lifetime cumulative risk of approximately 6% to 8%. 1 Despite the large amount of literature on PAA, it continues to have a significant rate of diagnostic error,2,3 and many etiopathogenic and pathophysiologic aspects have not been clearly elucidated yet.
The diagnosis of PAA is based on anamnesis and physical examination, basic laboratory tests (leukocytes, neutrophils, C-reactive protein [CRP], and procalcitonin [PCT]) 4 and imaging tests such as abdominal ultrasound or abdominal CT scan.4–6 Sometimes, those elements have been combined to create indexes, such as the Pediatric Appendicitis Score (PAS). 7 In recent years, there has been a growing interest in finding biomarkers that may represent a novel and efficient diagnostic tool for diagnosing PAA. Illustrative examples are interleukin-6 (IL-6), calprotectin, neutrophil gelatinase-associated lipocalin (NGAL) and pentraxin-3.8–11 The distinction between complicated and uncomplicated PAA, a field of growing interest because of its prognostic and therapeutic implications, has also benefited from the emergence of specific biomarkers, such as hyponatremia or hyperbilirubinemia.12,13 These markers have demonstrated adequate diagnostic yields and are promising tools for the future.
The literature regarding alterations in the coagulation profile in the context of PAA is scarce. In a retrospective study, Morandi et al. 14 found that children with PAA were more likely to present altered extrinsic coagulation pathway, especially those with complicated PAA, and that fibrinogen was the parameter with the best diagnostic performance. Along with this, Prada Arias et al. 15 found that the diagnostic yield of fibrinogen was moderate in distinguishing PAA from non-surgical abdominal pain (NSAP) and good in distinguishing complicated PAA from non-complicated PAA. 16 Recent studies in adults showed similar results. 17
However, the study by Morandi et al. 14 is not exempt of limitations, such as the retrospective design and the absence of control group. In this context, we conducted the present study with two main objectives: to compare the coagulation profile of children with PAA and those with NSAP and describe the diagnostic performance of the different coagulation parameters to distinguish PAA from NSAP in a prospective cohort. As secondary objective, we aimed to repeat the analyses comparing complicated versus non-complicated PAA.
Patients and Methods
This study was approved by our center's clinical research ethics committee prior on December 18, 2020, under code PI_2020/112. The ethical principles of the Declaration of Helsinki were applied for the conduct of this research study. The parents or legal representatives of all participants signed an informed consent form prior to the inclusion in the study.
Study design
This is an observational prospective study to compare the coagulation profile between children with NASP and those with PAA and determine the diagnostic performance of different parameters of the coagulation profile. The patients included in this study were divided into two groups: patients who came to the emergency department for acute abdominal pain and in whom the diagnostic of acute appendicitis was finally excluded, also defined as NSAP (group 1), and patients with histologically confirmed diagnosis of acute appendicitis (PAA) (group 2). For further analysis, patients in group two were stratified in non-complicated PAA (congestive, phlegmonous, or suppurative appendicitis) and complicated PAA (gangrenous or perforated appendicitis) based on the histopathologic classification of the appendix.
Congestive appendicitis was considered polymorphonuclear infiltration of the appendix without invasion of the lamina propria. Phlegmonous or suppurative appendicitis was considered polymorphonuclear infiltration of the appendix with invasion of the lamina propria. Gangrenous appendicitis was considered polymorphonuclear infiltration of the appendix with invasion of the lamina propria or mural necrosis. Perforated appendicitis was considered to be any of the previous alterations with the presence of micro- or macroscopic perforation of the appendix. This histologic evaluation was performed in all cases by the same pathologist and it was done in a blinded manner without knowing the results of the study.
The inclusion criteria for this study were patients aged 0 to 14 years inclusive who attended our pediatric emergency department with acute abdominal pain suggestive of acute appendicitis (initially mesogastric pain and later radiating to the right iliac fossa, onset pain in the right iliac fossa) of less than five days of evolution and associated with at least one of the following symptoms: hyporexia, nausea, vomiting, fever, or diarrhea.
Exclusion criteria for this study were as follows: Clear suspicion of acute appendicitis or with clinical instability not requiring complementary tests prior to surgery, previously known hematologic or coagulation profile alterations, previous history of vitamin K deficiency, liver or kidney disease, treatment with vitamin K antagonist or heparin in the month prior to surgery, metastatic malignancy, active autoimmune disorders, prior appendectomy, immunosuppressant treatment within 28 days prior to emergency evaluation, systemic steroid treatment within 14 days prior to emergency evaluation, and abdominal trauma prior to emergency evaluation.
All patients with NSAP were contacted two weeks after their inclusion in the study to confirm that they had not been diagnosed with PAA in that period.
Patients were recruited when the personnel conducting the investigation were available at the center. The recruitment period extended from February to December 2021.
Sociodemographic and clinical information was collected at recruitment, during patients' stay in the emergency department. Analytical, surgical, radiologic, and histologic information was extracted from participants' clinical records. In relation to sociodemographic variables, the following were collected: age, race, gender, height, weight, and body mass index. Regarding clinical variables, the following were collected: hours of pain, characteristics of pain, presence or absence of hyporexia, emesis, fever, diarrhea, urinary and rectal symptoms, temperature in the emergency department, physical examination, degree of hydration, duration of hospital stay, post-operative complications, and need for transfusion of blood products.
Regarding the analytical variables, the following were collected: blood count (leukocytes, neutrophils, red blood cells, platelets, mean platelet volume), biochemistry (CRP, PCT, bilirubin, glycemia), coagulation (
Regarding the radiologic variables, the following were determined: appendicular caliber, presence of appendicular inflammatory signs, and presence of peritoneal free liquid. Regarding the surgical variables, the following were collected: surgical approach, need for conversion, intra-operative findings, intra-operative bleeding volume, duration of the procedure, presence of intra-operative complications.
Sample collection and determination of the coagulation profile
Of the 151 patients enrolled, 93 agreed to have a venous blood sample taken in a 3.5 mL tube containing a 3.2% sodium citrate during their stay in the emergency department. Serum samples were processed following the standard procedure by laboratory staff blinded to the patient's group. All coagulation parameters were measured in the same sample concurrently. The platelet-to-lymphocyte ratio (PLR) was calculated as absolute platelet count/absolute lymphocyte count.
Statistical analysis
To calculate the sample size required for our analyses, we used the mean and standard deviation values of fibrinogen presented by Prada-Arias et al.15,16 as reference. Assuming an alpha of 0.05 (two-sided) and a power of 85%, 32 patients were required in each group to observe significant differences.
For descriptive purposes, the median and interquartile ranges or mean and standard deviation were used for quantitative variables and proportions for categorical ones. Kolmogorov-Smirnov test was used to assess the normality of quantitative variables. Sociodemographic and clinical variables were compared between groups using the Mann-Whitney U test and the Fisher exact test.
We evaluated the results of the coagulation parameters separately and, for each of them, considered that the patient had an alteration if he/she presented a value outside the normal range proposed by our laboratory.
To calculate the parameters' capacity to distinguish between NASP and PAA, and between complicated and non-complicated PAA, we calculated the area under the receiver operating characteristic curves (ROC) of
To compare the discriminatory capacity of each coagulation parameter with that of other routine serum markers, we performed a ROC comparison analysis. Statistical significance was settled in a p value <0.05. All statistical analyses were performed with STATA, version 17.0 (StataCorp LCC, College Station, TX).
Results
Sociodemographic and clinical characteristics
This study included 151 patients divided into two groups: patients with NSAP in whom the diagnosis of PAA was excluded (NSAP group; n = 53) and patients with a confirmed diagnosis of PAA (PAA group; n = 98). In 93 (62%) of the 151 enrolled patients (NSAP = 34 patients, PAA = 59 patients) a coagulation study was performed at the time of diagnosis. To rule out the possibility of selection bias, the included sample (n = 93) was compared with the excluded sample (n = 58) due to missing data on coagulation parameters. No differences in sociodemographic or clinical variables were found between the two groups (data not shown). Finally, 59 PAA patients in whom histopathologic information on the appendix was available were further classified into complicated PAA (n = 19) and non-complicated PAA (n = 40).
Sociodemographic characteristics of patients by group are shown in Table 1. On average, patients with NSAP were older, taller, and heavier than those with PAA. No differences were observed between patients with complicated and non-complicated PAA. Clinical characteristics of the patients by group are shown in Table 2. Patients with NSAP had more diarrheal stools and emetic episodes than those with PAA. Also, the hours of pain evolution and the proportion of patients with fever was higher in the group of complicated PAA than in that with non-complicated PAA.
Sociodemographic Characteristics of the Patients Included in the Study
Numbers are mean (standard deviation) or number (percentage).
NSAP = non-surgical abdominal pain; PAA = pediatric acute appendicitis.
Clinical Characteristics and Analytical Values of the Patients Included in the Study
Numbers are mean (standard deviation) or numbers (percentage).
NSAP = non-surgical abdominal pain; PAA = pediatric acute appendicitis; CRP = C-reactive protein; PCT = procalcitonin; FEU = fibrinogen equivalent units; aPTT = activated partial thromboplastin time; INR = international normalized ratio.
Median, interquartile range
Regarding the surgical procedure, among the 59 patients who underwent surgery, 57 were operated on by single-port transumbilical laparoscopy (TULA), one of whom required conversion to a Rocky-Davis type laparotomy. One patient underwent a conventional three-port laparoscopy and one patient underwent a direct Rocky-Davis laparotomy. Acute appendicitis was identified in all patients, and no patient in the series presented additional abdominal pathology. The mean operative time was 42 ± 16 minutes, and there were no intra-operative complications in any of the patients. The intra-operative bleeding volume, quantified by aspiration, was less than 10 mL in all cases.
Serum inflammatory biomarkers
The analytical values of serum biomarkers by group are shown in Table 2. On average, patients with PAA had higher levels of total leukocytes, total neutrophils, CRP and PCT (p < 0.01) than those with NSAP. In additon, compared with patients with NSAP, those with PAA had higher mean values of
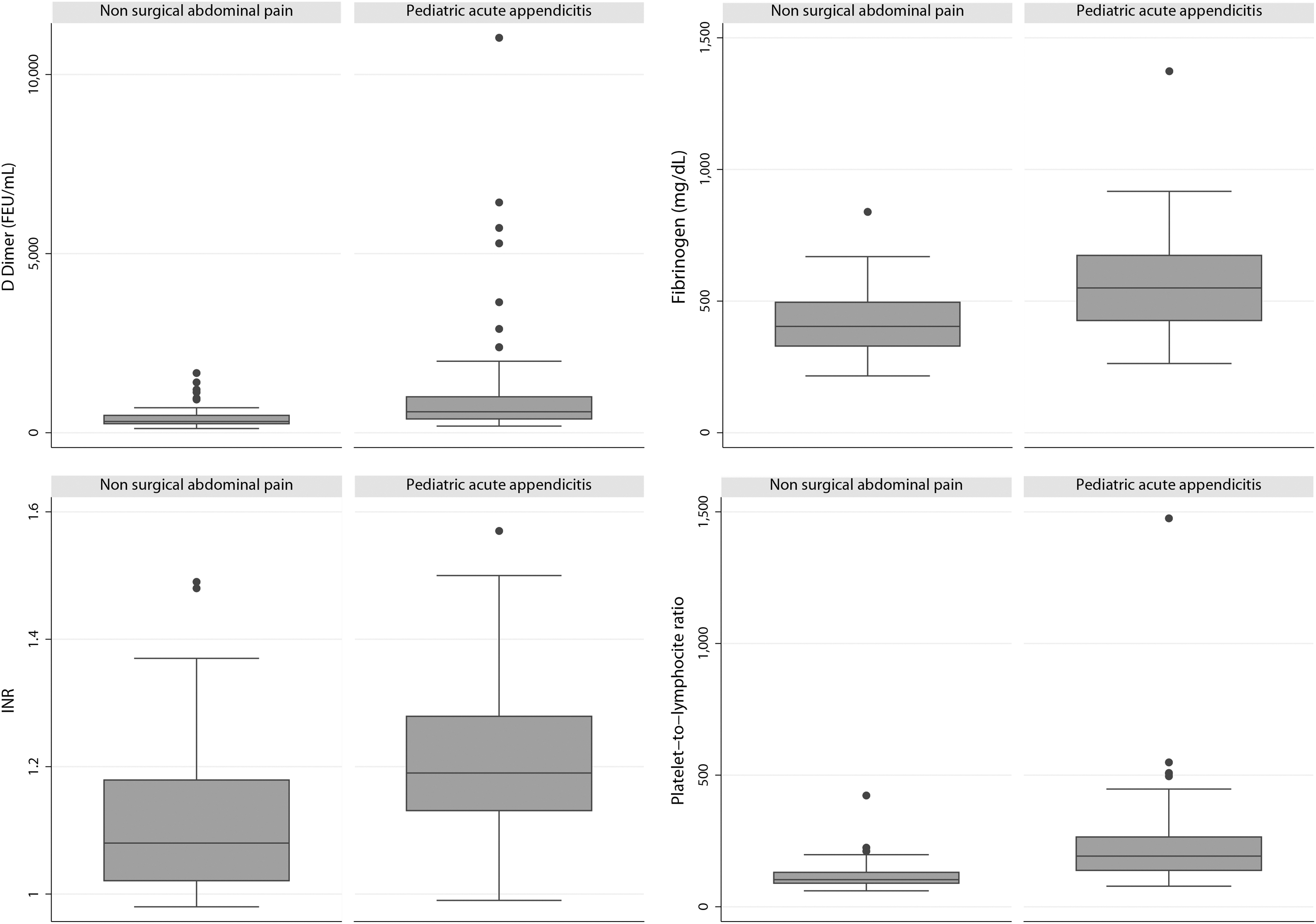
Box-plot representation of
Along with this, children with complicated PAA had higher mean levels of total leukocytes, total neutrophils, CRP, and PCT (p < 0.01) than their peers with non-complicated PAA. On average, patients with complicated PAA had higher levels of INR (p = 0.04) and fibrinogen (p < 0.01) than those with non-complicated PAA. No differences were observed for mean
Prevalence of altered coagulation profile
The prevalence of alterations in the coagulation parameters is shown in Table 3. We found a high proportion of children with altered coagulation profile in both the NSAP and the PAA groups, but none of the patients needed specific treatment for the correction of coagulopathy. Differences between groups were observed for
Prevalence of Alterations in the Different Coagulation Markers Evaluated
NSAP = non-surgical abdominal pain; PAA = pediatric acute appendicitis; aPTT = activated partial thromboplastin time; FEU = fibrinogen equivalent units; INR = international normalized ratio.
Proposed Cutoffs for Each Coagulation Parameter (NSAP vs. PAA)
NSAP = non-surgical abdominal pain; PAA = pediatric acute appendicitis; AUC = area under the curve; INR = international normalized ratio; FEU = fibrinogen equivalent units.
Diagnostic performance of the coagulation profile
The AUC and the selected cut-off point for each coagulation biomarker with its associated sensitivity and specificity are shown in Table 4. The PLR was found to be the biomarker with the highest AUC (AUC, 0.82; 95% confidence interval [CI], 0.72–0.92), followed by the fibrinogen, with an AUC of 0.74 (95% CI, 0.65–0.85).
Nevertheless, the comparation of the AUC of the different parameters showed that the diagnostic yield of fibrinogen was not significantly better than that of the
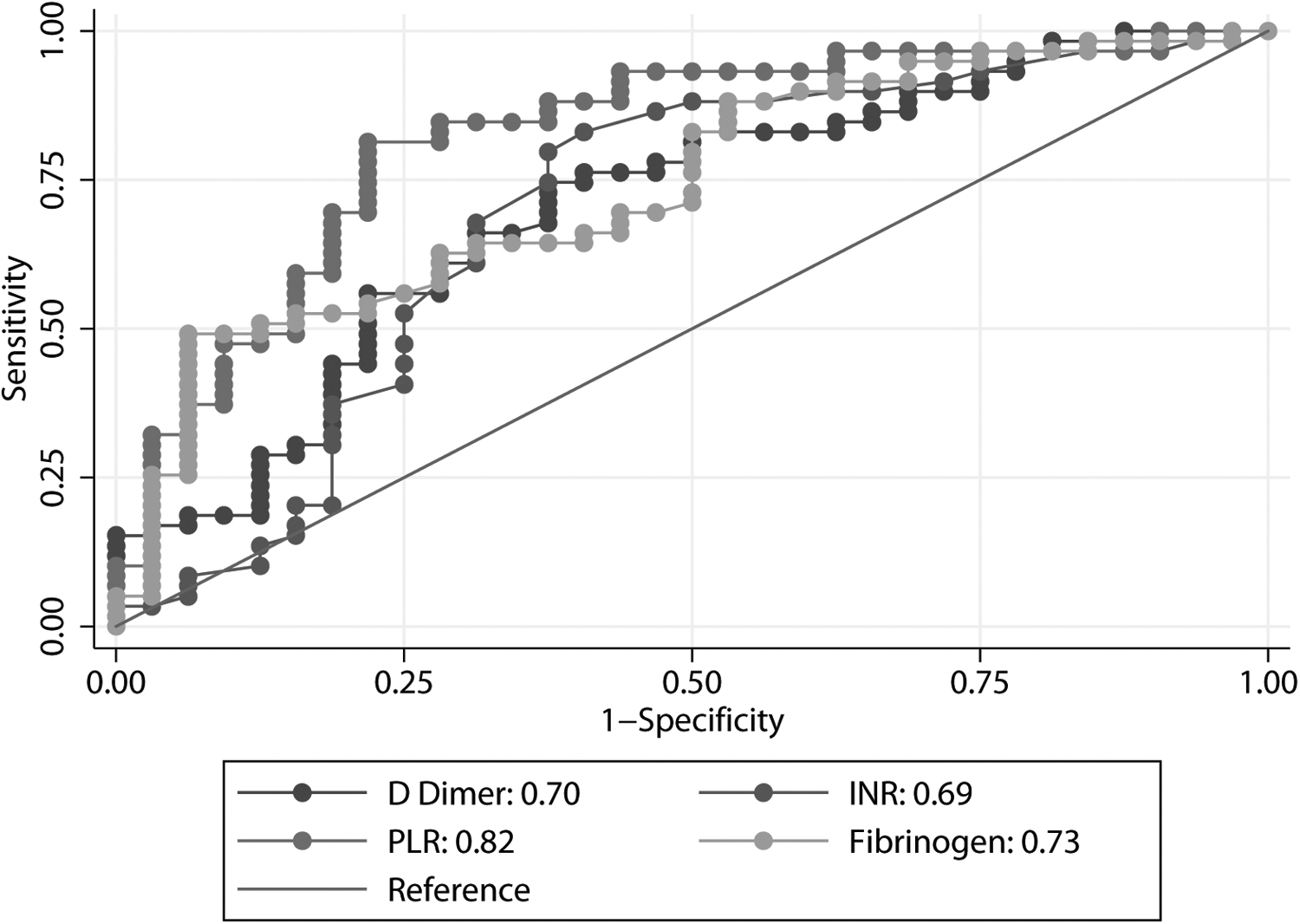
Graphical representation of the receiver operating characteristic (ROC) curve of fibrinogen,
Classically used biomarkers for the diagnosis of PAA are leukocyte count, neutrophil count, CRP, and PCT, which showed an AUC of 0.88 (95% CI, 0.81–0.95), 0.90 (95% CI, 0.84–0.96), 0.76 (95% CI, 0.65–0.86) and 0.75 (95% CI, 0.64–0.85), respectively. The comparison of the AUC of these biomarkers with that of the fibrinogen showed that leukocyte count and neutrophil count outperformed fibrinogen in terms of diagnostic performance (p < 0.05), but that was not the case for CRP and PCT (p > 0.05)
Complicated and non-complicated PAA
The analysis of the discriminatory capacity of the parameters of the coagulation profile to distinguish between non-complicated and complicated PAA (Table 5) showed that fibrinogen had the highest AUC (AUC, 0.71; 95% CI, 0.57–0.86) and its diagnostic yield was better than that of

Graphical representation of the receiver operating characteristic (ROC) curve of fibrinogen,
Proposed Cutoffs for Each Coagulation Parameter (Complicated vs. Non-Complicated PAA)
PAA = pediatric acute appendicitis; AUC = area under the curve; CI = confidence interval; INR: International normalized ratio; FEU = fibrinogen equivalent units.
Discussion
The present prospective validation study found that patients with PAA had higher levels of
The literature describing the prevalence of altered coagulation profile in PAA is scarce. A recent large series in adults reported the prevalence of coagulopathy in acute appendicitis to be up to 5%, without differences in the adjusted risk of post-surgical transfusion, re-admission, or re-operation between patients with coagulopathies and those without.
18
In our study, we found that the prevalence of alterations of the coagulation profile in patients with PAA could be as high as 62.71% considering
The etiopathogenic and pathophysiologic mechanisms underlying these alteration have not been clearly elucidated yet. It is known that PAA is associated with a systemic inflammatory response, 8 which is related to the production of procoagulant factors. Recent studies found patients with acute appendicitis had altered levels of factor VII but normal levels of factor IX, 19 which together with the work of Morandi et al. 14 confirmed that patients with acute appendicitis tend to present alterations in the extrinsic coagulation pathway. We hypothesize that the alteration of the extrinsic coagulation pathway could be consequence of the systemic inflammatory response triggered by the bacterial translocation from the appendix to the blood stream.
A number of publications suggested that the fibrinogen had an acceptable diagnostic performance in PAA.14–17
Our results agree with those studies and add to the previous evidence because we found no difference between the diagnostic yield of fibrinogen and that of
Although PLR is not a coagulation parameter per se, its potential diagnostic performance—especially to discern between complicated and non-complicated PAA—has been suggested in previous works. 20 In our series, we found that PLR was higher in the PAA group than in the NSAP group (p = 0.02), but no differences were found between patients with complicated and non-complicated PAA (p = 0.68). Regarding its diagnostic yield, PLR proved to be a useful marker to distinguish between PAA and NSAP (AUC, 0.82; 95% CI, 0.72–0.92), but a poor marker to distinguish between complicated and non-complicated PAA (AUC, 0.56; 95% CI, 0.39–0.73). These results contradict previous evidence, which suggested that PLR could be a useful diagnostic tool to discriminate between complicated and non-complicated PAA. 20
Alterations in the coagulation profile of children with PAA is frequent in clinical practice, but largely underreported in the scientific literature. In additional analyses, we compared clinical characteristics of patients who underwent surgery according to whether or not they had a coagulation disorder. We found no differences between groups regarding surgical time, intra-operative bleeding, intra-operative complications, days of hospitalization, and post-operative complications. In this scenario, we concluded that the alteration in the extrinsic coagulation pathway in patients with PAA may constitute a subclinical situation that we hypothesized could be explained because children are generally healthy patients without comorbidities (groups 1 and 2 of the ASA classification) and appendectomy is a short surgery, often performed by minimally invasive approaches, and well tolerated by patients.
Our study has several strengths including the prospective design, the large sample size, and the thorough statistical analyses. Despite our findings, we must acknowledge some limitations. First, we used a convenience sampling, which is susceptible of a selection bias. Additionally, 58 patients were excluded because of missing data on their coagulation profile. Nevertheless, inclusion and exclusion criteria were strictly applied, and we did not observe differences between included and excluded patients in sociodemographic and clinical characteristics. Second, we believe that although our sample size calculation was performed correctly, some of our results may not have reached statistical significance because of the sample size, especially those related to comparisons of non-complicated versus complicated PAA.
Conclusions
In conclusion, our results showed the presence of an alteration in the extrinsic coagulation pathway in patients with PAA that is more pronounced in patients with complicated PAA. New prospective studies with a larger sample size should confirm these findings and further investigate the underlying etiopathogenic and pathophysiologic mechanisms of this alterations.
Footnotes
Acknowledgments
We would like to thank the team of nurses of the Pediatric Emergency Department of Hospital Universitario de Navarra for their excellent work in the recruitment of patients for this study. Their dedication, care and patience have been essential. We would like to give special thanks to Jon Ariceta, Ainhoa Iceta, Nuria Clerigué, Fidel Gallinas, Marga Aranda, and Sonia Iso for their involvement during the design and development of this study, which would not have been possible without their constant and selfless support.
The ethics committee for clinical research of the Complejo Hospitalario de Navarra (CHN, Pamplona, Spain) assessed this project under registration code PI_2020/112 and approved it on December 18, 2020. The legal guardians of all patients involved in the study signed an informed consent before entering the study.
Authors' Contributions
Conceptualization and study design: Arredondo Montero. Literature search and selection: Arredondo Montero. Recruitment: Arredondo Montero, Antona. Data curation and extraction: Arredondo Montero, Martin-Calvo, Antona. Formal analysis: Arredondo Montero, Martin-Calvo. Investigation: Arredondo Montero, Martin-Calvo. Methodology: Arredondo Montero, Martin-Calvo. Project administration: Arredondo Montero, Martin-Calvo, Resources: Arredondo Montero, Martin-Calvo. Validation: Arredondo Montero, Martin-Calvo. Visualization: Arredondo Montero, Martin-Calvo. Writing—original draft: Arredondo Montero, Martin-Calvo. Writing—review and editing: Arredondo Montero, Martin-Calvo, Antona, Bardají Pascual, Bronte Anaut, López-Andrés. Laboratory determinations: López-Andrés.
All authors listed made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
Data Availability
All data pertaining to this study are available upon justified request through the author in correspondence.
Funding Information
This study did not receive external funding. None of the authors have financial disclosures to declare.
Author Disclosure Statement
The authors declare that they have no conflict of interest.