
Abstract

To the Editor:
H
A 66-year-old male presented to our department with a 30-minute history of severe abdominal pain. He reported subarachnoid hemorrhage and epidural hematoma 19 days prior. At that time, no abdominal distension and hematochezia was noted. On physical examination, peritonitis in the right abdomen, weakened peristaltic sound, and negative shifting dullness were observed. The abdominal computed tomography (CT) showed multiple branching gas density shadows in the liver and mesentery of the upper abdomen (Fig. 1A). Moreover, the superior mesenteric vein, caecum and ascending colon were marked dilated with a large amount of gas (Fig. 1B). Hence, ANE complicated with HPVG was considered. The patient underwent emergency open right hemicolectomy, during which the intestinal wall of the terminal ileum and cecum were found to have full-thickness necrosis, the inner wall of the ascending colon and partial transverse colon were necrotic, with 100 mL purulent secretion (Fig. 1C). A diagnosis of ANE was considered based on pathologic characteristics, which revealed extensive inflammation, with large-scale local neutrophil infiltration, and the mucosa and partial intestinal wall necrosis (Fig. 1D). There were no complications during nine-month follow-up after surgery.
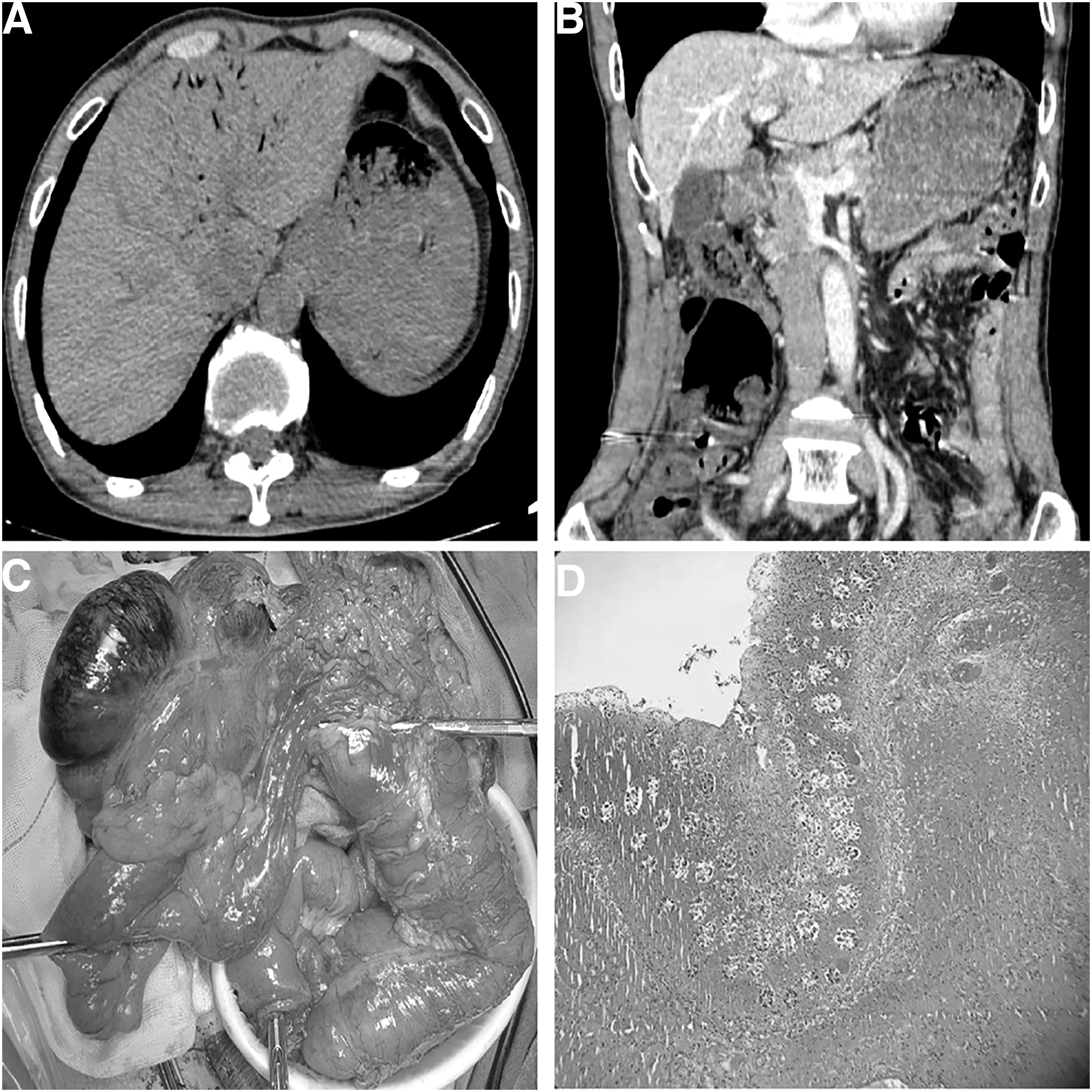
Clinicopathologic features of the patient.
As a rare acute inflammatory disease, ANE is characterized by intestinal hemorrhage and necrosis. The pathogenesis of ANE plus HPVG, nevertheless, lacks empirical support. Researchers have reported the nosogenesis was associated with Clostridium perfringens infection. 3 Scholars have speculated that intestinal necrosis caused by various reasons and the infection of gas-producing bacteria in the abdominal cavity spread to the portal vein. 4 Other risk factors included diabetes mellitus, protein deficiency, abundant trypsin inhibitors, and affluent protein or moldy food. 1 The most typical abdominal CT characteristic of ANE plus HPVG is hepatic portal vein gas, and dilated bowel loops, pneumatosis, localized or diffuse peritonitis could be seen. Thus, abdominal CT is egarded as the most accurate and effective auxiliary examination. Culture of Clostridium perfringens type C may contribute to ANE diagnosis. Acute necrotizing enteritis complicated by HPVG often has a poor prognosis, which results in the worse survival rate. Meanwhile, we believe that surgery is the only effective method to save the patient.
Based on our extensive literature search, this case is the fifth patient in the world and the first successful life-saving case of ANE plus HPVG. In our case, typical abdominal CT features were identified by surgeons. It only took approximately 30 minutes from the admission to diagnosis, which was considered the primary requirement for patient survival. Additionally, prompt surgical treatment is another successful element. We believe that surgical intervention can prevent the progression of shock and disease efficiently. Of course, early fluid resuscitation and empiric broad-spectrum antibiotic agents are also essential therapies.