
Abstract
Background:
Necrotizing soft tissue infections (NSTIs) are rapidly spreading, life-threatening infections that require emergent surgical intervention with immediate antibiotic initiation. However, there is no consensus regarding duration of antibiotic therapy after source control. We hypothesized that a short course of antibiotic therapy is as effective as a long course of antibiotic therapy after final debridement for NSTI.
Methods:
A systematic review of the literature was performed using PubMed, Embase, and Cochrane Library from inception to November 2022. Observational studies comparing short (≤7 days) versus long (>7 days) antibiotic duration for NSTI were included. Primary outcome was mortality and secondary outcomes included limb amputation and Clostridium difficile infection (CDI). Cumulative analysis was performed with Fisher exact test. Meta-analysis was performed using a fixed effects model and heterogeneity was assessed using Higgins I2.
Results:
A total of 622 titles were screened and four observational studies evaluating 532 patients met inclusion criteria. Mean age was 52 years, 67% were male, 61% had Fournier gangrene. There was no difference in mortality when comparing short to long duration antibiotic agents on both cumulative analysis (5.6% vs. 4.0%; p = 0.51) and meta-analysis (relative risk, 0.9; 95% confidence interval, 0.8–1.0; I2 0; p = 0.19). There was no significant difference in rates of limb amputation (11% vs. 8.5%; p = 0.50) or CDI (20.8% vs. 13.3%; p = 0.14).
Conclusions:
Short duration antibiotic therapy may be as effective as longer duration antibiotic therapy for NSTI after source control. Further high-quality data such as randomized clinical trials are required to create evidence-based guidelines.
Necrotizing soft tissue infections (NSTIs) are rare, rapidly spreading, life-threatening infections that require immediate initiation of broad-spectrum antibiotic agents and emergent surgical debridement. The term NSTI includes a spectrum of diseases such as Fournier gangrene, gas gangrene, and necrotizing fasciitis and myositis. 1 These infections can affect any part of the body, but the extremities are most frequently involved. Mortality ranges from 10% to 30% with a high risk of morbidity, including limb amputation.1–3
Although the basic tenets of management are clear (i.e., resuscitation, control of source contamination, removal of all infected and/or necrotic material, and administration of antibiotic agents), there are wide variations in clinical practice and no expert consensus exists on duration of antibiotic therapy after source control. 4 Several guidelines suggest continuing antibiotic therapy until source control is achieved, the patient has improved clinically, and fever has resolved for 48 to 72 hours. 5
With the increasing prevalence of multi-drug–resistant (MDR) organisms, an increasing emphasis on antibiotic stewardship, and especially the results of the Study to Optimize Peritoneal Infection Therapy (STOP-IT) trial, practitioners have started investigating whether shorter antibiotic duration would also be effective for other kinds of infections, including NSTI.6,7 In 2017, Lauerman et al. 8 published a retrospective study suggesting that shorter courses of antibiotics should be considered for the treatment of NSTIs. In 2020, the Surgical Infection Society (SIS) published updated guidelines with the same conclusion prompting several more studies on the topic. 9
The aim of this study is to perform a systematic review of prior data examining the optimal duration of antibiotic agents for treatment of NSTIs. We hypothesized that a short course of antibiotic agents (≤7 days) would be as effective as a longer course (>7 days) after source control for NSTI.
Methods
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. 10 The protocol was registered online with PROSPERO. 11
Search strategy and selection criteria
Pubmed, EMBASE, and Cochrane review were searched from database inception to November 2022. A search strategy for each database was constructed using a combination of medical subject headings and free-text terms including necrotizing soft tissue infection, NSTI, antibiotic, and antibiotic agents. The electronic database search was supplemented by a manual search of the reference lists of included articles.
Titles, abstracts, and full-text articles were screened by two independent reviewers (N.B.L. and B.L.C.) for relevance. The inclusion criteria were defined a priori and were as follows: randomized controlled trials or cohort studies (prospective and retrospective); articles that included adult patients (≥18 years) diagnosed with NSTI who received antibiotics after source control; and articles that reported outcomes after treatment. Case reports, non-clinical studies, pediatric studies, animal studies, editorials, commentaries, conference abstracts, and articles in a language other than English were excluded. Reviews were excluded but were evaluated to ensure that the selected articles were also included in our study.
Definition of short versus long-term antibiotic agents
We defined the length of antibiotic agents after final surgical debridement (i.e., source control) similar to the STOP-IT trial rather than total duration of antibiotic agents. 6 This avoids the confounder of a varied number of debridements, as those requiring more operations would likely require a longer total duration of antibiotic agents. Short course was defined as less than seven days in the SIS 2020 guidelines, so seven days was used as the cutoff for this study. 9
Data extraction and quality assessment
One reviewer compiled the data. For each article, data including the number of patients, country of origin, patient demographics, outcomes, and complications were extracted.
The Critical Appraisal Skills Program (CASP) checklist for cohort studies was used to assess the methodologic quality and risk of bias in the included studies (CASP). 12 The checklist for cohort studies includes 14 questions for a possible 28 points. Two reviewers (N.B.L. and B.L.C.) independently evaluated the quality of the included studies by use of the appraisal tools and a CASP score was calculated for each trial. The studies were categorized based on their score: high quality was a score ≥18, moderate was a score of 17 to 10, and low quality was a score nine or less. These categories were devised a priori by the authors. When there was disagreement in the scoring, this was discussed between the authors until resolution.
Outcomes
The primary outcome was mortality. Secondary outcomes included recurrence, limb amputation, Clostridium difficile infection (CDI), hospital and intensive care unit (ICU) length of stay (LOS), 30-day re-admission, and Necrotizing Infection Clinical Composite Endpoint (NICCE) success. Recurrence was defined as recurrent infection requiring further, unplanned debridement or restarting antibiotics. Treatment success for NSTIs is defined by NICCE and was defined as all of the following to be true: three or less surgical debridements by day 14, no amputation after the first debridement, modified Sequential Organ Failure Assessment (mSOFA) one day or less at day 14, and alive at 28 days. 13
Statistical analysis
Cumulative analysis was performed using Fisher exact test for dichotomous variables. Heterogeneity among studies was quantified using Higgins I2 statistics with I2 > 75%, >50%, and <25% considered high, moderate, and low heterogeneity, respectively. A random effects model was applied for analysis. Two-sided p values <0.05 were considered statistically significant. Statistical analysis was performed with SPSS Statistics, version 28.0 (IBM Corp, Armonk, NY).
Results
In total, 622 articles were identified from the initial Pubmed, EMBASE, and Cochrane Library search. After duplicates were removed, 461 articles remained. Of these, 413 were excluded based on review of their titles and 48 remained for abstract review. Nine articles were reviewed and four were included in the systematic review (Fig. 1). No additional studies were identified by review of reference lists and no other review articles were found.
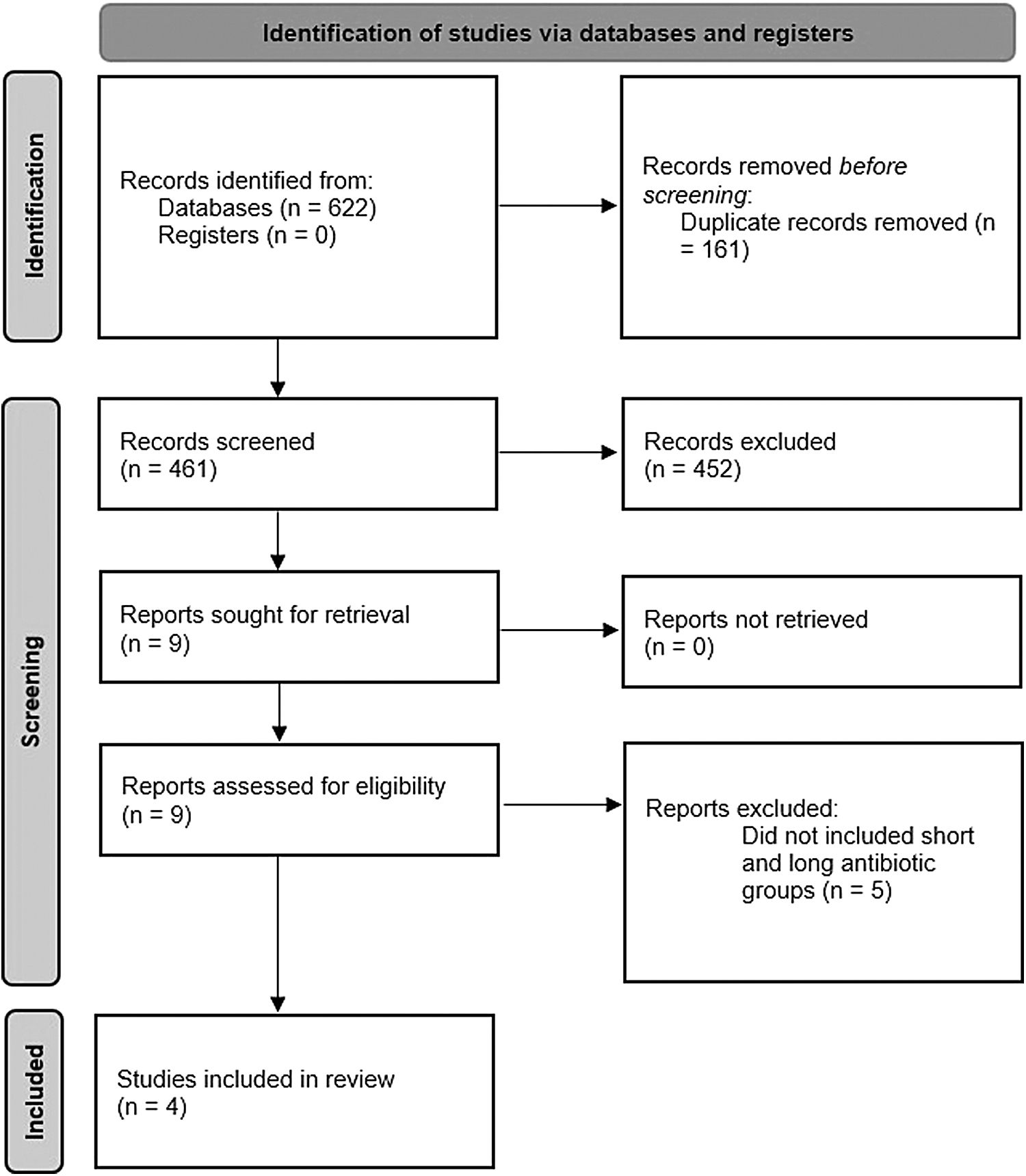
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 flow diagram.
Quality assessment and description of included studies
All four studies underwent a full-text review and assessment of risk of bias. Methodology of the studies is included in Table 1 along with study and background information. Of the four studies included, three were retrospective and one had an intervention group that was prospective and a control group that was retrospective. There were no randomized controlled trials published on this topic. All four studies were from the United States. Kenneally et al. 13 and Terzian et al. 14 included patients who received <48 hours of antibiotic agents in their intervention group, whereas Lauerman et al. 8 and Valadez et al. 15 included patients who received seven days or less of antibiotic agents. Kenneally et al. 13 defined long duration as >48 hours, so these patients were excluded from this study. Terzian et al. 14 had an average antibiotic duration of 7.5 days for the control group, thus these were included.
Study Background and Demographic Information a
AA = African American; BMI = body mass index; CASP = Critical Appraisal Skills Programme; CKD = chronic kidney disease; d = days; ESRD = end stage renal disease; h = hours; HIV = human immunodeficiency virus; NSTI = necrotizing soft tissue infection; WBC = white blood cell count.
Values reported as mean or n (%) unless otherwise stated; some studies did not report several of the variables, so the percentage for the totals column was calculated only including the studies that reported each outcome
A total of 532 patients (180 short duration and 351 long duration) were included in the analysis. These patients were enrolled from 2010 to 2018. Lauerman et al. 8 did not include the average age of the patients, however, for the remaining three studies, the average age of the patients was 52 years. In total, 67% of patients were male and 67% had diabetes mellitus. In the two studies that reported race, 70% of patients were white and 26% were African American. Lauerman et al. 8 only included patients with Fournier gangrene, and in total 61% of patients had an NSTI of their perineum. The average white blood cell count on presentation was 18,000, they underwent an average of 2.2 surgical debridements, and 53% of patients were septic on admission. Lauerman et al. 8 and Valadez et al. 15 defined sepsis according to Sepsis-3 guidelines. 16
All four studies reported NSTI type. Type 1 is polymicrobial, type 2 is monomicrobial, type 3 is gram negative, and type 4 is fungal. 17 Most patients had a type 1 or 2 NSTI (60.9% and 26.5%, respectively) and none reported type 4 infections. Two studies reported the bacterial species. Only Kenneally et al. 13 reported the antibiotic agents each patient received, however, broad-spectrum antibiotic agents were used in all four studies (Table 2).
Necrotizing Soft Tissue Infection Type and Antibiotic Therapy
GAS = group A Streptococcus; GBS = group B Streptococcus; GPS = gram-positive cocci; MRSA = methicillin resistant Staphylococcus aureus; MSSA = methicillin sensitive Staphylococcus aureus.
Outcomes
There was no difference in the primary outcome of mortality for short versus long antibiotic duration (5.6% vs. 4.8%; p = 0.683). Three studies reported recurrence and there was no difference between antibiotic duration groups (2.3% vs. 2.7%; p = 1.000). Limb amputation and CDI were reported by two studies each and there was no difference based on antibiotic duration (Table 3). The outcomes for NICCE success rates were only reported in two studies, but one study only includes patients from the short antibiotic duration group, so composite analysis is biased.
Outcomes
CDI = Clostridium difficile infection; LOS = length of stay; NICCE = Necrotizing Infection Clinical Composite Endpoint.
Meta-analysis
A meta-analysis was performed for the primary outcome of mortality, which was the only outcome reported in all four studies. There was no difference in mortality comparing short to long duration antibiotic agents on both cumulative analysis (5.6% vs. 4.0%; p = 0.683) and meta-analysis (relative risk, 0.9; 95% confidence interval, 0.8–1.0; I2, 0; p = 0.19; Fig. 2).

Meta-analysis of mortality.
Discussion
The major new findings from this systematic review are that there was no difference in mortality when comparing short- to long-duration antibiotic agents on both cumulative analysis (5.6% vs. 4.0%; p = 0.683) and meta-analysis (relative risk, 0.9; 95% confidence interval, 0.8–1.0; I2, 0; p = 0.19). Within the context of the limitations discussed in detail below, these observations support the conclusion that a shorter duration of antibiotic agents after final surgical debridement for NSTIs may be appropriate.
A potential risk of a shorter course of antibiotic agents for NSTI is recurrence of the infection if it is undertreated. However, the recurrence rates for the two groups were nearly the same with a low rate of recurrence, suggesting adequate surgical debridement is more important than the duration of antibiotic agents for eliminating the infection. Although the included studies reported the type of NSTI, they did not report on the antibiotic resistance of the cultures. If patients were initially on antibiotic agents that had inadequate coverage for the organisms present in the wound, this could have affected the recurrence rate.
On the other hand, there are several risks of prolonged antibiotic duration, including an increased risk of acquiring a MDR organism, leading to more complications, longer hospital stay, and increased risk of mortality. Increasing antimicrobial resistance is accelerated by overuse of antibiotic agents. This overuse of antibiotic agents leads to an increase in more severe diseases, length of disease, risk of complications, mortality rate, and healthcare costs. 7 There is strong evidence that antimicrobial stewardship is prudent thus if a longer duration of antibiotic agents is of no benefit, a shorter course should be used. Moreover, antibiotic agents themselves also pose risks to individual patients, and side effects can range from mild to severe and include nephrotoxicity or neutropenia. For these reasons, antibiotics should be de-escalated based on sensitivities and stopped when they no longer provide a benefit to the patient. The studies did not report side effects from the antibiotics received by the two groups, however, this outcome could be included in future studies.
Additionally, antibiotic exposure is the most common factor predisposing patients to CDIs and increased doses, number of antibiotic agents, and total antibiotic days increase the rate of CDI.18,19 Thus, reducing the total dose as well as the number and days of antibiotic agents should reduce the incidence of CDI. In the present study, there was no statistically significant difference in the rate of CDI between short- and long-duration groups.
This review, and the included studies, have other limitations. First and foremost, failure to find a difference does not prove no difference exists. All the studies were at least partially retrospective and were conducted at a single institution or affiliated institutions, limiting their generalizability. In addition to only being non-randomized trials, the included studies reported different outcomes, most of which are relatively rare as is the diagnosis of NSTI, which limited our ability to group patients and analyze them. It is also possible that patients presented to other hospitals with a recurrence, which could affect this outcome. Lauerman et al. 8 defined short course of seven days or less of total antibiotic agents rather than antibiotic agents received after final debridement that could affect outcomes as well. Lauerman et al. 8 also included outside hospital transfers, so the number of surgical debridements and length of antibiotic agents could be inaccurate. Transfer is associated with a higher mortality rate in NSTIs, thus including these patients could have influenced the outcomes in this study. 20 Mortality was the only outcome reported by all four studies; therefore, we could not perform a meta-analysis for the secondary outcomes.
Factors associated with mortality in NSTI include age >75, multifocal NSTI, severe peripheral vascular disease, nosocomial infection, severe sepsis, and septic shock on hospital admission. 1 It would be important to factor in these predictors, however most of these were not reported by every study. Early debridement (i.e., within 12 hours of admission) also improves mortality, however, only one study reported time to first operative debridement. 21 These limitations underscore the need for well-designed randomized controlled trials and should be the focus of future studies. Although we defined short duration as seven days or less, even shorter antibiotic durations such as three or four days may also be effective and can be explored in future studies.
Conclusions
Short-duration antibiotic agents may be as effective as longer duration antibiotic agents for NSTI after source control. As the only available evidence on this topic is from retrospective studies, high-quality data such as randomized clinical trials and multicenter studies are required to create evidence-based guidelines.
Footnotes
Authors' Contributions
Conceptualization (supporting): Lyons. Conceptualization (lead): Meizoso. Methodology (lead): Lyons. Formal analysis (lead): Lyons. Formal analysis (supporting): O'Neil, Ramsey: Meizoso. Investigation (lead): Lyons. Data curation (lead): Lyons. Writing—original draft (lead): Lyons. Writing—review and editing (equal): Cohen, O'Neil, Ramsey, Proctor, Namias, Meizoso. Visualization (lead): Lyons. Visualization (supporting): Meizoso. Investigation (supporting): Cohen. Data curation (supporting): Cohen. Resources (equal): Proctor: Namias. Project administration (equal): Proctor: Namias, Meizoso. Supervision (equal): Proctor: Namias, Meizoso. Validation (lead): Meizoso.
Funding Information
There was no external grant support. This work was supported by the Daughtry Family Department of Surgery.
Author Disclosure Statement
For all authors, no competing financial interests exist.