
Abstract
Background:
Surgical site infection (SSI) is an infrequent but costly complication after elective spine surgery. Identification of important temporal changes and predictive factors may inform targeted prevention efforts.
Patients and Methods:
A retrospective study of elective spine surgery patients was performed using the National Surgical Quality Improvement Programs (NSQIP) database from 2011 and 2019. Temporal changes in SSI and related factors were examined descriptively. Recursive partitioning and bootstrap forest techniques were used to inform the development of predictive models for SSI.
Results:
A total of 6,038 (1.66%) of 363,754 patients had an SSI recorded. Peri-operative transfusion and preoperative anemia decreased over the nine-year period, however, obesity and diabetes mellitus increased, whereas the SSI rate remained essentially unchanged. A full model including 15 variables had an area under the curve (AUC) of 0.693 (95% confidence interval [CI], 0.686–0.700) whereas a reduced model with just nine variables had an AUC of 0.690 (95% CI, 0.683–0.697). Adjusted odd ratios (aOR) greater than two were noted for only three variables; a posterior approach (aOR, 2.32; 95% CI, 2.14–2.50), body mass index (BMI) >40 kg/m2 (aOR, 2.63; 95% CI, 2.39–2.90), and surgical duration longer than 350 minutes (aOR, 2.39; 95% CI, 2.14–2.67). Remaining retained variables included albumin <3.5 g/dL, inpatient procedure, peri-operative transfusion, diabetes mellitus (both insulin/non-insulin), anemia, and smoking.
Conclusions:
Surgical site infection rate remained unchanged over a nine-year period despite the lower rates of allogeneic blood transfusion. Class 3 obesity, long operative times, and a posterior approach mainly for thoracic/lumbar spine procedures seemed more pragmatic, but their predictive performance was only modest in our prediction models for SSI.
Surgical site infection (SSI) is one of the most common infections representing 15.7% to 21.8% of all health-care–associated infection.1–3 Wound complications such as SSI increase unplanned re-admissions to hospital and intensive care unit as well as mortality after various types of surgery.4,5 The reported SSI rates vary in the types (deep vs. superficial) and periods of surveillance, but the estimated incidence is between 0.5% and 2% among elective spine procedures.6,7 Previously identified predictors of SSI in spinal surgery include high body mass index (BMI), poor glycemic control, high American Society of Anesthesiologists (ASA) physical status (>3), prolonged operative time, and operated vertebral levels.6,8–11 Allogeneic blood transfusion has been also associated with a risk of SSI after spine surgery,12,13 and transfusion-related immunomodulation is a presumed mechanistic link. 14
Concerted efforts among surgeons, anesthesiologists, and nursing staff in the surgical quality improvement15,16 and patient blood management 17 have succeeded in lowering SSI and transfusion rates in various surgical specialties.3,18,19 On the other hand, there are increases in obesity and diabetes mellitus on a global scale. 20 Adult obesity rates is 42% in the United States,21,22 and 89.0% of patients diagnosed with diabetes mellitus are overweight or obese. 23 Altered immune functions in obesity and diabetes mellitus are known to enhance bacterial infectivity in the bone with an implanted device. 24 Poor wound healing is expected after extensive adipose tissue injuries in obese patients because of relatively poor vascularization, underlying chronic inflammation, and altered humoral and cellular healing processes.25,26
Given the recent quality improvement efforts and rising rates of obesity and diabetes mellitus, it is imperative to review temporal trends and identify remaining predictors of SSI in contemporary spine surgery. The aims of the present study were to describe the nine-year trends of body mass index (BMI) and SSI in elective inpatient and outpatient spine surgery and to assess predictive values of both established risk factors and potential modifiers available in the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database.
Patients and Methods
The study was reviewed and approved by the University of Oklahoma Health Sciences Center Institutional Review Board. Retrospective data were obtained from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) Participant User Files (PUF) from the years 2011 to 2019. The files were queried for the Current Procedural Terminology (CPT) codes for spine arthrodesis (CPT 22532–22819), laminectomy (CPT 63001–63051), or both. Excluded were emergency procedures, patients who received pre-operative transfusion, and procedures lasting longer than 12 hours (Fig. 1).
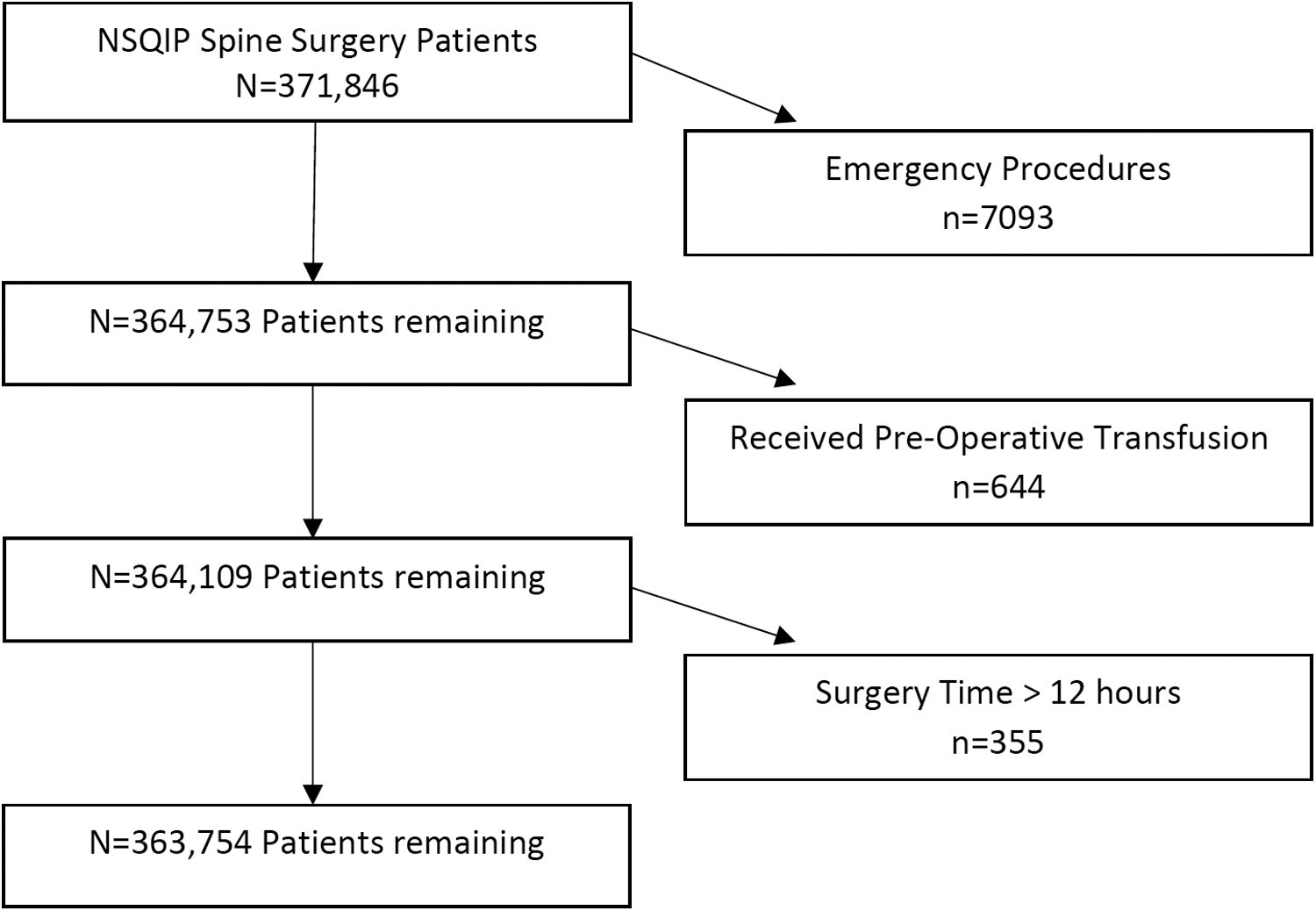
Study population. NSQIP = National Surgical Quality Improvement Program.
Surgical site infection was the primary outcome of interest. The list of potential predictors included: age, gender, diabetes mellitus, long-term steroid use, anemia, peri-operative transfusion, surgeon specialty (neurosurgery or orthopedics), BMI, year of surgery, pre-operative laboratory tests (hematocrit, hemoglobin, albumin, creatinine), current smoker, hypertension, operative time in minutes, vertebral region, number of vertebral levels, and surgical approach dichotomized as anterior/posterior. Multiple imputation was used to complete missing laboratory values. Hemoglobin was calculated as the pre-operative hematocrit divided by three, and anemia was defined by hemoglobin <13 or <12 g/dL for males and females, respectively. Diabetes mellitus was further categorized as insulin-dependent and non-insulin types. Body mass index (kg/m2) was grouped into commonly used categories: <18.5, 18.5–24.9, 25–29.9, 30–39.9, and >40 kg/m2. Vertebral levels were grouped as 1–3, 4–6, and 7+ levels. Recursive partitioning identified potential cut-points for operative time and age with regard to predicting SSI. The cut-points were less than 96, 96–177, 178–350, and longer than 350 minutes for operative time, and 63 years for age.
Descriptive statistics and graphical methods were used to summarize the trends in SSI and other potential risk factors over time. Mean and standard deviation (SD) or median and interquartile range (IQR) were used to summarize continuous variables. Differences in continuous variables were tested using t-tests or Wilcoxon rank sum tests. Frequencies and proportions were used to summarize categorical variables and χ 2 tests were used to test bivariable associations. Because of potential relations among candidate predictors, pairwise correlation was assessed. Using number of patients available with/without SSI and assuming a null AUC of 0.50 estimated power was greater than 99% to detect an AUC as small as 0.55.
Recursive partitioning with cross-validation as well as bootstrap forest techniques were used to screen the list of predictors and gain insight to their relative contribution in predicting SSI. Multivariable logistic regression was used to develop and evaluate the predictive models. Both a full model and reduced model using variables suggested by recursive partitioning and bootstrap forest results were developed. Model discrimination and fit were determined using area under the curve (AUC) and Hosmer-Lemeshow good-of-fit statistics, respectively. Adjusted odds ratios with 95% confidence intervals were calculated. Area under the curve contrasts using the method of DeLong et al. 27 were used to compare models and assess the added predictive value of individual variables. Effect plots for selected variables were produced to show the relation of these predictors across operation time while holding other covariables fixed.
Results
The final study population contained 363,754 patients (Fig. 1). Using the year 2011 as a baseline, the proportion of spine patients developing SSI has remained steady over time. Among commonly implicated risk factors of SSI, the proportion of class 1–2 and class 3 obesities increased, whereas both peri-operative transfusion and pre-operative anemia declined (Fig. 2).

Percent changes in surgical site infection (SSI) and implicated risk factors. The trends in SSI and commonly implicated SSI risk factors were shown as a percent change from the year 2011 as a baseline. The percent change in SSI rates was minimal over time. Between 2011 and 2019, anemia and transfusion rates were 2.5% and 4.76% lower, whereas the proportions of body mass index (BMI) ≥30 and ≥40 kg/m2, (BMI >30 kg/m2 and >40 kg/m2), and non-insulin-dependent diabetes mellitus (NIDDM) were 6.53%, 1.67% and 3.39% greater.
With the exception of surgical specialty all predictors showed statistical significance in bivariable testing although many of the actual differences were small (Table 1). Notable differences between the non-SSI and SSI groups were seen with respect to approach, outpatient/inpatient, BMI group, anemia, peri-operative transfusion, diabetes mellitus, and low pre-operative albumin. A posterior surgical approach was more commonly associated with SSI (87.5% vs. 74.7% for non-SSI). Importantly, there was a strong correlation of approach and operated vertebral region with 89.2% of posterior approaches occurring in the thoracic or lumbar region, and 79.6% of anterior approaches occurring in the cervical region. Median operative time was 34 minutes longer in the SSI group. Obesity (BMI >30 kg/m2) was more common in SSI group (60%) than non-SSI group (47.6%).
Comparison of Variables by SSI
SSI = surgical site infection; BMI = body mass index; IQR = interquartile range; min = minutes; SD = standard deviation.
Recursive partitioning results suggested just nine variables were needed to maximize the AUC for predicting SSI, which included, in order of contribution to the model, operative time, surgical approach, BMI categories, inpatient/outpatient, albumin <3.5 g/dL, peri-operative transfusion, gender, current smoker, and diabetes mellitus. Results from several bootstrap forests suggested the same top six variables, however, variables beyond that point varied from forest to forest, suggesting weaker predictive value for those variables.
For comparison, a model was fit containing 15 variables that remained statistically significant (p < 0.05) after adjustment (Table 2). This full model had an AUC of 0.693 (95% CI, 0.686–0.700). Continuous age was also considered in the model; however, the model performance based on AUC statistics was nearly identical to the model using the age cut-point of 63 years. A model with nine variables suggested by the screening process was then fit yielding an AUC of 0.690 (95% CI, 0.683–0.697). Odds of SSI showed incremental changes with a high of 2.39 (95% CI, 2.14–2.67) for operations lasting longer than 350 minutes. The obese and morbidly obese groups also had increased odds of SSI with aORs of 1.36 (95% CI, 1.25–1.47) and 2.47 (95% CI, 2.25–2.72), respectively. A posterior approach was the only other factor with a higher aOR (aOR, 2.32; 95% CI 2.14–2.50). The remaining factors retained in the reduced model included albumin <3.5 g/dL, inpatient procedure, peri-operative transfusion, diabetes mellitus, anemia, and smoking.
Multivariable Models Predicting SSI
SSI = surgical site infection; BMI = body mass index.
AUC 0.693 (95% CI, 0.686–0.700) H-L χ 2 11.08, p = 0.197.
AUC 0.690 (95% CI, 0.683–0.697) H-L χ 2 8.97, p = 0.345.
Holding other covariables constant, the predicted probabilities for SSI among patients with a BMI ≥40 kg/m2 with or without diabetes mellitus or peri-operative transfusion were all higher than patients with a normal BMI (Fig. 3A). Moreover, the probabilities increased more rapidly with longer operative times than patients with a normal BMI. Also notable is insulin-dependent diabetes mellitus was just as influential on SSI probabilities as transfusion, especially among the BMI >40 kg/m2 group. Both anterior and posterior approaches among BMI >40 kg/m2 had higher predicted probabilities of SSI than either approach in normal BMI group (Fig. 3B). Also apparent, was the probability of SSI increased more rapidly for posterior approaches in the BMI >40 kg/m2 group.

Predicted probabilities of surgical site infection (SSI) for selected factors across pperative time.
Discussion
The present analysis of the NSQIP data (2011–2019) included 363,754 inpatient and outpatient patients who underwent elective spine surgery. The overall rate of 1.66% for any SSI agrees with a recent meta-analysis of 22,475 cases with the pooled incidence of SSIs within 30 days of surgery: 1.4% for superficial SSI and 1.7% for deep SSI. 28 Temporal changes over nine years showed steady increases in the prevalence of class 1–2 obesity and diabetes mellitus whereas transfusion rates declined (Fig. 2). Annual raw SSI rates did not change numerically, but odds of SSI for 2017–2019 compared with 2011–2012 suggested a slight increase in the trend (aOR, 1.17; 95% CI, 1.07–1.28). The prevalence of obesity (classes 1–3) and any diabetes mellitus increased by 8.2% and 4.7%, respectively, between 2011 and 2019. The multivariable adjustments demonstrated the strongest associations with SSI for BMI >40 kg/m2 (aOR, 2.63; 95% CI, 2.39–2.90), posterior approach (aOR, 2.32; 95% CI, 2.14–2.50), and operative time longer than 350 minutes (aOR, 2.39; 95% CI, 2.14–2.67) using normal BMI and operative time less than 96 minutes, respectively, as a referent. Both the full and reduced model using nine variables were shown to have a suboptimal predictive value (AUC <0.7; Table 2). This suggests there are other predictive factors of SSI that are unmeasured or unrecorded in the NSQIP. Moreover, commonly implicated etiologic factors appear only weakly predictive of SSI, in part because of the relative rarity of the complication overall, and a combination of factors (Fig. 3A and 3B) is more important than any one factor in isolation.
A recent work by Edmiston et al. 29 utilized a commercial insurance database to document the impact of post-spinal surgical SSI on incremental healthcare costs. The authors used a longer surveillance period up to 180 days, reporting the overall incidence of 6.6% (1.7% superficial and 4.9% deep SSI). The higher incidence of SSI could be partly attributed to the inclusion of emergencies (2.9% of all cases) that was associated with a high rate of SSI (13.8%). In contrast, our analysis excluded emergent cases because predicting infection risks becomes extremely difficult because of multiple unmeasured and unpredictable factors (e.g., major bleeding). The data of Edmiston et al. 29 data showed that superficial and deep SSI occurred on median post-operative days 44 and 28, respectively. The number of reported superficial infections could have been accrued over time in at-risk patients with uncontrolled diabetes mellitus and peripheral vascular disease because of poor wound healing. Although 30-day SSI rates are tracked for benchmarking, 28 a longer surveillance period and more patient-level data may be needed to fully elucidate the risk of SSI and to control incremental costs to treat infections. 29
Previous NSQIP studies have assessed SSIs after spine surgery, but most of them were largely etiologic in nature, and as such they seldom reported any measures of the predictive value of their models or specific factors studied. For example, extreme obesity is considered as an etiologic factor because adipose tissues are poorly vascularized and prone to soft tissue infection and necrosis after prolonged retraction during multilevel spine surgery.25,26 An NSQIP study by Schoenfeld et al. 30 included 5,887 arthrodesis cases of any spine level, and reported an increased odds of wound complication per each unit (kg/m2) of BMI (aOR, 1.04; 95% CI, 1.02–1.06). This aOR translates into a 2.19-fold increase in the odds of SSI when BMI increases from 20 to 40 kg/m2. Another NSQIP study by Marquez-Lara et al. 31 included 24,106 lumbar fusion and decompression surgeries, and reported increased associations between superficial wound infection and BMI. The highest unadjusted relative risk (RR, 3.8; 95% CI, 2.5–5.9) was reported for BMI >40 kg/m2 relative to normal BMI, however, there was no adjusted analysis presented despite a number of differences noted between normal and obese BMI groups. Finally, the NSQIP study by Sebastian et al. 10 reported an SSI rate of 2.9% in 5,441 cervical spine cases, and an aOR of 1.60 (95% CI, 1.10–2.34) for BMI >35 kg/m2.
Our present findings were in line with these previous studies as we reported an aOR of SSI was 2.63 (95% CI, 2.39–2.90) for BMI >40 kg/m2 relative to normal BMI, and a higher aOR of SSI for a posterior approach, the majority of which involve the thoracic/lumbar region (aOR, 2.32; 95% CI 2, 14–2.50; Table 2). It is known that a posterior approach increase the risk of infection by approximately 2-fold. 28 Compared with an anterior approach, posterior wounds are more prone to skin flora as well as contaminations from bowel or bladder incontinence.32,33 Patients with extreme obesity may be prone to antibiotic dosing errors due to altered pharmacokinetics and pharmacodynamics. 34 Taken together, peri-operative antibiotic coverage, post-operative wound cleaning, and early detection of SSI should be optimized in patients with BMI >40 kg/m2 undergoing spine surgery with a posterior approach.
Another notable finding in our study was an incremental change in the odds of SSI according to the operative time. Using the operative time under 96 minutes as a referent, aORs were 1.52 (95% CI, 1.41–1.65) and 2.39 (95% CI, 2.14–2.67) for operative times 177–350 minutes and longer than 350 minutes, respectively (Table 2). Similarly, Schoenfeld et al. 30 previously reported the operative time exceeding 309 minutes was associated with SSI (aOR, 2.0; 95% CI, 1.3–3.0). 30 Sebastian et al. 10 also reported a higher aOR (aOR, 1.41; 95% CI, 1.08–1.84) for operative time longer than 197 minutes versus less than 93 minutes in cervical spine cases. 10
Several mechanistic links can be postulated for the association between operative time and SSI. Longer operative time is likely to expose patients to fluctuations in body temperature. 35 Intra-operative temperature monitoring by non-contact infrared thermography reported the surgical field temperature of 24.3°C to 29.8°C with a surrounding temperature of 27.7°C despite active body warming to maintain the core temperature in an observational orthopedic study. 36 Cold-induced vasoconstriction and reduced oxygen tension in adipose tissues presumably suppress functions of leukocytes and other immune cells against bacterial infection. 37
Lengthy surgery is often complicated by bleeding, coagulopathy, and allogeneic blood transfusion,38,39 and thus its association with SSI may be explained by transfusion-related immunomodulation. 14 Allogeneic blood transfusion has been considered as an etiologic factor for SSI in spine surgery.12,13 In our study, patients who developed any SSI received more blood transfusions than those without SSI (12.0% vs. 4.7%; Table 1). In addition, pre-operative anemia was more frequent in patients with any SSI (22.0% vs. 13.3%). However, aORs of SSI were only modestly increased with transfusion (aOR, 1.46; 95% CI, 1.33–1.59) or anemia (aOR, 1.37; 95% CI, 1.28–1.47) after multiple adjustments. The lack of strong associations of transfusion and anemia with SSI are also supported by the yearly trends (Fig. 2). The prevalence of transfusion and anemia decreased between 2011 and 2019 by 4.76% and 3.18 %, respectively. The transfusion rate in orthopedics used to be higher in 2011 (13.2% vs. 6.0% in neurosurgery), but it decreased to 5.4% by 2019. Despite the reduced transfusion rates, SSI rates did not change over 9 years. In addition, there were no differences between the two specialties in the SSI rate. After considering yearly trends and odds of SSI, prolonged operative times and obesity seemed more pragmatic predictors compared to transfusion or anemia.
Residual confounding is possible in our non-etiologic study, but Falsetto et al. 13 also reported a similar aOR (aOR, 1.48; 95% CI, 1.01–2.16) of SSI associated with transfusion in lumbar spine surgery using NSQIP data (2012–2016) and propensity matching (transfused vs. non-transfused; n = 1,992 each). The use of propensity matching might have reduced confounding by indication, however, the authors lost large samples (original, n = 174,891) because of an inability to match. As shown in our data, most of the cases (71.7%) had an operative time less than 177 minutes (Table 1), but SSI was more common in longer cases (Table 2). Therefore, the study by Falsetto et al. 13 study might have underestimated the contribution of operative time to SSI. On the other hand, they included pre-operative transfusion (within 72 hours), which might have augmented the association between SSI and transfusion regardless of operative time. Our study excluded preoperative transfusion as these patients tend to be severely anemic and ill. However, pre-operative albumin below 3.5 g/dL was shown to be an independent predictor of SSI (1.94; 95% CI, 1.76–2.14). This is in agreement with others who have reported the associations of comorbidities (e.g., Charlson comorbidity index) with SSI.10,30
Surprisingly, diabetes mellitgus was only weakly predictive of SSI in these data and showed only modest aORs of 1.14 and 1.51 for non-insulin and insulin types, respectively. These are lower than an odds ratio from a meta-analysis done by Meng et al. 28 where they found higher odds of SSI among patients with diabetes mellitus after spine surgery (OR, 2.04; 95% CI, 1.69–2.46), however, important details regarding the procedures and type of diabetes mellitus were not reported. 40 Similarly, it is possible additional details lacking in NSQIP regarding the duration of diabetes mellitus or a measure of control such as HgbA1c could improve the predictive value of this commonly implicated SSI risk factor.
There are other important limitations in our study. Given the modest discrimination seen with our models, it is likely other unmeasured factors influence the likelihood of SSI. One example is compliance with post-discharge wound care, an aspect of SSI difficult to measure in any design. Another would be the lack of information regarding antibiotic prophylaxis use and dosage variation. Only pre-operative laboratory values are available in NSQIP so it is possible further or new important derangements may occur post-operatively. Additional development of a prognostic model for SSI will also need to include a process for external validation to confirm performance.
Conclusions
Despite changes in commonly implicated risk factors, rates of SSI remained unchanged over a nine-year period. Anemia, transfusion, and diabetes mellitus showed little predictive value for SSI, although perceived as key prognostic factors in etiologic studies. Considering these findings, class 3 obesity, a posterior approach mainly for thoracic/lumbar spine procedures, and operative times seem to be more pragmatic predictors compared with transfusion or anemia. Our data reiterate the importance of countering adult obesity to reduce the risk of SSI after major spine surgery. Limited predictive performance of the NSQIP database is likely caused by unmeasured or unrecorded factors, and targeted collection of additional patient-level data should be explored in spine surgery.
Acknowledgments
The authors would like to thank the American College of Surgeons and participating NSQIP centers for the data collection that allowed us to perform this study. The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the American College of Surgeons NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Footnotes
Authors' Contributions
Conceptualization: Stewart, Butt, Tanaka. Methodology: Stewart, Butt, Tanaka. Project administration: Stewart, Butt, Tanaka. Supervision: Stewart, Butt, Tanaka. Date curation: Stewart, Ma. Software: Stewart, Butt, Tanaka. Formal analysis and interpretation: all authors. Writing—original draft: Stewarrt, Terada, Tanaka. Writing—review and editing: all authors.
Funding Information
The authors received no funding for this research.
Author Disclosure Statement
The authors have nothing to disclose.