
Abstract
Background:
Surgical site infections (SSIs) have been associated with increases in terms of costs, hospital stay, morbidity, and mortality. We aimed to assess trends in SSIs monitored through 10 years of surveillance activities in our region, and to describe mortality attributable to SSIs in the two most frequently monitored surgical procedures: colorectal surgery and hip arthroplasty.
Methods:
A retrospective cohort study was conducted among the 42 hospitals participating in the surveillance network of our region in northern Italy. All colorectal and hip arthroplasty procedures performed between January 1st, 2010, and December 31st, 2019, and monitored through the surveillance system were included in the study. Surgical site infection rates, overall mortality, case fatality rates (CFR), and mortality attributable to SSIs were evaluated overall and by year of participation in the surveillance program.
Results:
In total, 11,417 colon surgery and 20,804 hip arthroplasty procedures were included. Among colon surgery procedures, SSI rates decreased from 9.21% in 2010 to 5.7% in 2019. A significant decreasing trend was found for overall mortality (p = 0.008), which progressively decreased from 4.96% in 2010 to 2.96% in 2019. Among hip arthroplasty procedures, no significant trend emerged for SSI and mortality rates. Considering the 10-year period, the CFR was 6.62% and 3.7% for SSIs after colon surgery and hip arthroplasty procedures, respectively.
Conclusions:
The impact of SSIs on the clinical outcomes of patients undergoing surgery highlights the importance of SSI surveillance.
Health-care–associated infections (HAIs) are known to be associated with a substantial burden for healthcare systems worldwide.1–4 In particular, surgical site infections (SSIs) are a frequent type of HAIs, and have been linked to increases in terms of costs, hospital stay, morbidity, and mortality.5,6 The economic burden is linked to the direct costs of hospitalization, such as the ones for diagnostic tests and treatment, but also to the prolonged hospital stay and eventually to a reoperation, if required. 7 Moreover, Astagneau et al. 8 previously described the associated burden in terms of mortality in patients with SSIs from 1997 to 1999, finding that 38% of deaths occurring among patients with SSIs were attributable to the infection itself, and identified SSIs as a predictor of mortality. A more recent study showed that crude mortality rates were higher in patients with SSIs for all the categories of surgery considered. 9
Surgical site infections are also considered to be among the most preventable HAIs.10–12 An effective measure to reduce the incidence of SSIs are surveillance programs, as demonstrated by several previous reports.5,13–18 In this regard a robust methodology must be applied, standardizing definitions and data collection, and implementing a rigorous follow-up. 10
In Italy, SSIs have been monitored through a national surveillance system for SSIs (Sistema Nazionale Sorveglianza Infezioni del Sito Chirurgico [SNICh]) 19 following the European Center for Disease Prevention and Control (ECDC) HAI-SSI protocol for definitions, data collection, and reporting methodology. 20 In the Piedmont region, in northwestern Italy, surveillance through the national network began in 2008 and is ongoing, involving all public and some private hospitals in the region.5,21
Considering the burden associated with SSIs in terms of mortality, it is worth exploring the issue. Therefore, the objective of this study was to update the findings of Astagneau et al. 8 and provide further insights into Italian epidemiology, assessing the trends through 10 years of surveillance activities, from 2010 to 2019, and describing mortality attributable to SSIs in the two most frequently monitored surgical procedures: colorectal surgery and hip arthroplasty. In addition, this study aimed at identifying areas where quality improvement efforts should be focused.
Methods
Study design
A retrospective cohort study was conducted among the 42 hospitals participating in SNICh in Piedmont. All colorectal and hip arthroplasty procedures performed between January 1, 2010, and December 31, 2019, and monitored through the surveillance system were included in the study.
Data collection
Data on included procedures were collected through SNICh, as previously reported in detail.5,22 Briefly, the surveillance system applies a national protocol based on the ECDC HAI-SSI network protocol.19,20 The participation in the network is voluntary and the surveillance is conducted for a minimum of six months each year, encouraging continuity. Demographic and clinical data are collected, including the occurrence of infection (within 30 days after the procedure for colorectal surgery and 90 days for hip arthroplasty), and the state at discharge (alive or deceased in hospital). Post-discharge surveillance is performed through post-operative visits in the same hospital or through a standardized telephone interview.
Ethics
As stated in the SNICh protocol, 19 the purposes of the program are surveillance of diseases and quality of care improvement, thus the written consent of patients involved or any other authorization from the ethics committee and/or the protection commissioner are not required. Additionally, the program is coordinated by public entities (National Centre for Disease Prevention and Control, Ministry of Health, Emilia-Romagna and Piedmont Regions). Patients are provided with an information sheet at admission to inform them about the hospital's participation in the surveillance program. All collected data are transferred anonymously to the regional coordinating center.
Statistical analysis
Patient demographics were summarized using descriptive statistics. Surgical site infection rates, overall mortality, case fatality rates (CFR; i.e., number of deaths occurring among infected patients), and mortality attributable to SSIs (difference between mortality in patients with and without an SSI), were evaluated overall and by year of participation in the surveillance program. Pearson χ 2 or Fisher exact tests were used to evaluate differences of distributions for the following categorical variables: gender, American Society of Anesthesiology (ASA) physical status score, infection risk index, elective or urgent/emergent procedure, and surgical technique (minimally invasive vs. open). Due to non-normal distribution at Shapiro-Wilk test, continuous variables were assessed using non-parametric Mann-Whitney U tests. Trends in SSI rates and overall mortality rates were calculated using χ 2 tests for trends. Analyses were performed using IBM SPSS Statistics, version 28.0.1 (IBM Corp, Armonk, NY) and setting two-tailed statistical significance at 0.05.
Results
During the study period, a total of 11,417 colon surgery and 20,804 hip arthroplasty procedures were monitored in 27 and 35 hospitals, respectively. Descriptive characteristics of included patients, overall and comparing the first and final included years, are summarized in Table 1. Further detail on performed operations is provided in Figures 1 and 2. As shown in Figure 1, the proportion of partial colectomy procedures among all colon surgery procedures was approximately 80% throughout the study period. The proportion of revisional hip arthroplasty procedures progressively decreased from 2010 to 2019 (Fig. 2).

Distribution of colon surgery operation types per year.
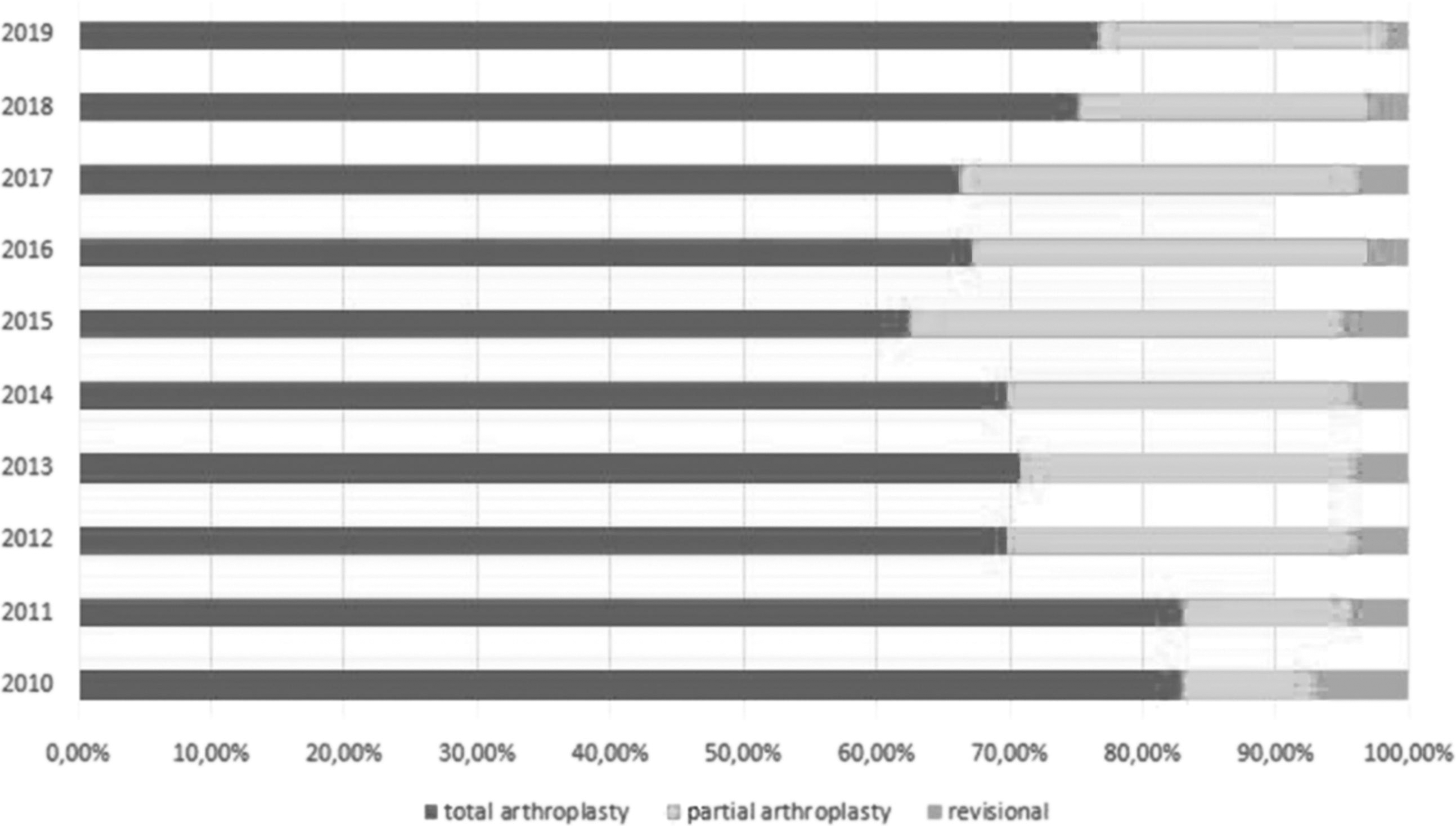
Distribution of hip arthroplasty operation types per year.
Demographic and Clinical Characteristics of Included Patients, 2010–2019
ASA = American Society of Anesthesiologists physical status score; IQR = interquartile range; LOS = length of stay.
Indicates statistical significance (p < 0.05). Differences between 2010 and 2019 values investigated using Pearson χ 2 and Mann-Whitney U tests.
Considering colon surgery procedures, an increase in the proportion of patients with an ASA score ≥3 was found comparing 2010 and 2019, however, the proportion of minimally invasive procedures also increased, reaching almost 50% in 2019. Pre-intervention and overall hospital length of stay (LOS) decreased from 2010 to 2019.
Considering hip arthroplasty procedures, more older patients underwent surgery in 2019 compared to 2010. Comparing the same two years, there was an increase in the proportion of patients with ASA score ≥3 and urgent/emergent procedures. The distribution of infection risk index scores was also different comparing 2019 to 2010, with a shift towards higher scores.
Tables 2 and 3 summarize considered outcomes: SSI rates, mortality rates, and CFR, per year. Overall, 936 and 297 SSIs occurred among patients undergoing colon surgery and hip arthroplasty procedures, respectively, and a total number of 373 and 209 deaths were recorded. In total, 63.1% of SSIs occurred during the index hospital stay, whereas the rest occurred post-discharge. Median time to infection was nine days (interquartile range [IQR], 5–14) for SSIs after colon surgery procedures, and 20 (IQR, 10–30.5) for SSIs after hip arthroplasty procedures.
Outcomes for Patients Undergoing Colon Surgery Procedures, Stratified by Year
CFR = case fatality rate; OR = odds ratio; CI = confidence interval; SSI = : surgical site infection.
Not considering 252 procedures with missing status at discharge.
Outcomes for Patients Undergoing Hip Arthroplasty Procedures, Stratified by Year
CFR = case fatality rate; OR = odds ratio; CI = confidence interval; SSI = surgical site infection.
Not considering 282 procedures with missing status at discharge.
Among colon surgery procedures, SSI rates decreased from 9.21% in 2010 to 5.7% in 2019; however, no trend emerged (p = 0.268). A decreasing trend was found for overall mortality (p = 0.008), which decreased progressively from 4.96% in 2010 to 2.96% in 2019. Considering the 10-year period, the SSI rate was 8.2%, the overall mortality rate was 3.34%, and the CFR was 6.62%.
Among hip arthroplasty procedures, no trend emerged for SSI and mortality rates (p = 0.578 and p = 0.253, respectively). Considering the ten-year period, the SSI rate was 1.43%, the overall mortality rate was 1% and the CFR was 3.7%.
Among colon surgery procedures, 62 of 373 deaths (16.62%) occurred among patients with an SSI. Mortality among patients with and without infection was 6.62% and 2.97%, respectively, with an estimated attributable mortality of 3.65% for SSIs occurring after colon surgery procedures. Among hip arthroplasty procedures, 11 of 209 deaths (5.26%) occurred among patients with an SSI. Mortality among patients with and without infection was 3.7% and 0.97%, respectively, with an estimated attributable mortality of 2.73% for SSIs occurring after hip arthroplasty procedures. Characteristics of deceased patients with versus without SSI are reported in Table 4. As shown in the table, the only significant differences emerged for overall LOS, which was higher among patients developing SSI for both procedure categories.
Characteristics of Deceased Patients With Versus Without Surgical Site Infection After Colon Surgery and Hip Arthroplasty Procedures, 2010–2019
SSI = surgical site infection; ASA = American Society of Anesthesiologists physical status score; IQR = interquartile range; LOS = length of stay.
Indicates statistical significance (p < 0.05). Differences among patients deceased with versus without SSI investigated using Fisher exact test and Mann-Whitney U test.
Discussion
This study reports surveillance data collected over a 10-year period, including more than 30,000 procedures. The progressive increase in the number of both colon surgery and hip arthroplasty procedures monitored is a first important result, which has led to an increased representativeness of the surveillance system.
Considering colon surgery, this study found a decreasing trend in overall mortality during the 10-year period, even though the proportion of patients with ASA score ≥3 increased in 2019 compared with 2010. Furthermore, a not significant but progressive reduction in SSI rates of approximately 3.5% was observed, in line with previously described findings. 5 Surgical site infection and mortality rates after hip arthroplasty procedures also decreased non-significantly, probably due to having reached a plateau in terms of preventable negative outcomes. This result is even more relevant when considering that the continued widening of surveillance has resulted in the inclusion of older patients as well as patients with greater clinical complexity, reflecting the demographic situation in Italy.
Comparing the procedure categories included in the study, the rate of SSIs after hip arthroplasty was four times less frequent than after colon surgery procedures, and mortality following hip arthroplasty was 50% lower than following colon surgery procedures. This result is consistent with studies describing variable mortality rates and incidence of SSI depending on the type of surgery considered.8,23
Previous studies have described an increase in mortality of patients with SSI.8,24 Based on the results of this study, we estimated an attributable mortality of approximately 4% for SSIs after colon surgery procedures and 3% for SSIs after hip arthroplasty procedures. Furthermore, this study found a considerable increase in overall LOS in patients deceased with SSI in both types of surgery considered (median of 27.5 days for colon surgery and median of 41 days for hip arthroplasty), in accordance with previous findings of prolonged hospital LOS by approximately seven to 11 days in patients with SSI, compared with patients without infection. 25 Therefore, our results support previous findings of increased economic burden associated with severe SSIs, in addition to the clinical burden in terms of increased morbidity and mortality. 7
Surgical site infections are related to higher all-cause mortality rates, prolonged hospitalization, higher re-admission rates, and increased costs for healthcare systems.7,23-24 On the other hand, standardized and continuous SSI surveillance has proven effective in reducing SSI rates, LOS, re-admissions and the negative impact on patients' quality of life,7,26-28 reducing related costs and improving the management of elective surgery waiting lists.29,30 According to our results, a reduction in both pre-operative and overall LOS for colon surgery procedures and a reduction in overall LOS for hip arthroplasty procedures was found considering the 10-year period. Regarding colon surgery, these results are most likely due to the increase in the proportion of minimally invasive approach, however, the reduction in SSI rates could also have contributed.
The effectiveness of participation in surveillance networks in reducing SSI rates has been described in the literature previously.26–28 Moreover, the number of consecutive years of participation in surveillance networks has been associated with an increased impact in reducing SSI rates. 5 Other factors such as improvements in infection prevention and control activities could have contributed to decreasing SSI rates, in particular the adoption of a surgical bundle in our region has been associated with a positive impact of infection risk for both procedure categories.21,31 The four-element bundle was introduced in 2012, and included the following evidence-based practices: pre-operative showering, appropriate hair removal, antimicrobial prophylaxis (in terms of appropriate agent, timing, dose, and duration), and maintenance of intra-operative normothermia. The four elements of the bundle are established SSI prevention practices, however introducing the bundled intervention allowed to increase standardization and consistency of their implementation throughout our region.
This study had several limitations. The most important limit was the lack of information on post-discharge deaths, due to surveillance design. As other studies have also pointed out, it would be appropriate to monitor mortality longer after patient discharge, 23 or to be able to detect any SSI-related hospitalizations or deaths that have occurred post-discharge in other hospitals that are not part of the surveillance network. Based on the results shown in Table 2, we might assume worse clinical conditions of patients with SSI than those without, therefore further analysis with multistate models could be useful to avoid competing risk bias. Finally, we did not account for changing infection prevention and control activities over time or different implementation in participating hospitals.
Conclusions
Standardized data collection and participation in surveillance networks such as SNICh provide useful data for benchmarking purposes and allow to identify trends over time. The impact of SSIs on the clinical outcomes of patients undergoing surgery highlights the importance of SSI surveillance.
Footnotes
Acknowledgments
The authors thank the members of the regional working group Infezioni Correlate all'Assistenza and gratefully acknowledge the infection control staff involved in the SNICh program: Dr. A.Macor, C. Fanton, P. Berto, P. Bianco, R.G. Vecchietti, S. Fantino, A. Riccio (ASL Città di Torino); Dr. M. Giacometti, A. Trombotto, N. Gentile, B. Viviani, P. Desantis, M. Campobasso (ASL TO3); Dr. A. Scarcello, M. Bello, M. Boux, A. Buono, S. Greco, R. Musca, S. Naretto, M. Obert (ASL TO4); Dr. D. Morabito, F. Riccardi (ASL TO5); Dr. P Toscano, E. Ferrando, A. Pernecco, P. Ferrero (ASL AL); Dr. F. Di Nardo, B. Bacchetta, G. Beltrame, G. Zanetti (ASL NO); Dr. R. Broda, G. Marchese (ASL AT); Dr. F. D'Aloia, C. Frassati, M. Sicari (ASL BI); Dr. M. Salvatico, S. Gerbaudo, M. Giordana, L. Ghiglia, M.C. Operti (ASL CN1); Dr. V. Venturino, S. Cabutti, M. Rabino (ASL CN2); Dr. S. Gatti, M. Franchino, M. Staiano (ASL VC); Dr. V. Destefano, R. Pesce, L. De Giorgis, M. Bignamini (ASL VCO); Dr. C. Bolla, B. Montanari, M. Ricci, E. Marino (AO AL); Dr. C. Silvestre, Dr. F. Gremo, Dr. G. Guareschi, S. Zozzoli, E. Frasinelli, D. Filippi, G. Finotto, M. Gambino, L. Ferrero, E. Scalenghe, E. Spina, V. Procacci, E. Migliore, P. Dalmaso (AOU Città della Salute e della Scienza); Dr. P. Pellegrino, P. Occelli, A. Re (AO CN); Dr. I. Vigna, S. Bagnato, I. Casonato, A. Do Nascimento, A. Mercugliano (AO Mauriziano); Dr. P. Silvaplana, P. Lovera, S. Pelassa (AOU S. Luigi); Dr. M. Tacchini, R. Negri, C. Guenzi, P. Lino, L. Codari (AO NO); Dr. D. Tangolo, M. Carlevato, M. Valle (Osp. Humanitas Gradenigo); Prof. R. Russo, L. Turinetto, A. Muca, G. Dacci (Osp. Cottolengo); T. Romani (COQ Omegna), F. Baiardi, K. Enluida (Casa di Cura S. Anna); C. Bosio (Clinica Villa Igea); Dr. L. Savoia (Clinica San Gaudenzio), R. Terranova, E. Milan (Policlinico di Monza); Dr. P. Malvasio, M. Cossu (Osp. Koelliker).
Authors' Contributions
Conception and design: Vicentini, Zotti. Data collection: Elhadidy, Paladini, Cornio, Marengo. Formal analysis: Vicentini. Writing—original manuscript: Vicentini, Elhadidy, Marengo. Writing—review and editing: Zotti. Project coordination: Zotti.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Sisclosure Statement
Declarations of interest: none.