
Abstract
Background:
Pediatric acute appendicitis (PAA) involves a substantial consumption of health and economic resources. The identification of serum biomarkers that may help predict the post-surgical evolution of these patients is a field of great interest.
Patients and Methods:
This was a prospective, observational substudy within the Biomarkers for the Diagnosis of Appendicitis in Pediatrics (BIDIAP) cohort aimed at evaluating the association between post-surgical increase in serum IL-6 and different outcomes related to the clinical evolution of children operated on for PAA. Sixty-nine children with a confirmed diagnosis of acute appendicitis and both pre-operative and post-operative serum IL-6 were included in the study. Three multivariable-adjusted linear regression models were fitted to analyze the association between an increase of >10% in post-operative serum IL-6 level with the length of stay, the number of post-operative emetic episodes, and the onset of oral feeding. Two multivariable-adjusted logistic regression models were fitted to assess the association of the same exposure with the indication of antibiotherapy at discharge and with positivity in peritoneal fluid culture.
Results:
Thirteen children showed an increase of >10% in the post-operative serum IL-6 value (group 1) whereas 56 showed only a minor increase, or no change (group 2). After accounting for potential confounders, children in group 1 had a mean of three-day longer hospital stay (difference, 3.33; 95% confidence interval [CI], 0.57–6.09) and higher odds of a positive result in peritoneal fluid culture (odds ratio [OR], 37.43; 95% CI, 1.02–1361.28) than children in group 2.
Conclusions:
An increase of >10% in post-operative serum IL-6 value could predict longer hospital stay and higher odds of positive peritoneal fluid culture. Future prospective studies are needed to replicate these findings and to broaden the range of biomarkers that could predict the post-operative evolution of children operated on for PAA.
Pediatric acute appendicitis (PAA) is the most frequent urgent abdominal surgical pathology in the pediatric population, 1 and therefore, it is associated with significant social, economic, and healthcare costs. Although statistics vary according to countries and the structure of their healthcare systems, multicenter reports show an average cost per intervention ranging from $5,000 to $28,000, with the cost of operating being higher when patients are treated by pediatric surgeons than by general surgeons.2,3 This cost rises exponentially in the case of a complicated PAA. 4 Although recent studies have tried to find ways to optimize these numbers by promoting judicious use of surgical resources 5 or by trying to identify the most cost-efficient approach to complicated PAA (initial appendectomy on admission vs. interval appendectomy, for example), 6 the evidence on this subject is scarce. Given the prevalence of PAA, this is a field with a large potential impact on daily clinical care and, therefore, of great interest. In addition to costs, another relevant issue is the adequate planning of hospital resources. In this sense, the ability to predict the duration of a hospital admission could contribute to better management of available resources.
Novel biomarkers have demonstrated diagnostic validity in PAA. Illustrative examples are interleukin-6 (IL-6) or Pentraxin-3 (PTX-3),7–9 which have shown a moderate diagnostic performance to distinguish between PAA and non-surgical abdominal pain (NSAP). On the other hand, some of these biomarkers, specifically serum total bilirubin, and IL-6, have demonstrated a moderate ability to discriminate between complicated and uncomplicated PAA.7,8,10 Nevertheless, little is known about the potential usefulness of the postoperative value of certain biomarkers to predict clinical evolution of children operated on for PAA.
In 2004 Latifi et al. 11 found that persistent elevation of serum IL-6 in pediatric patients with intra-abdominal sepsis correlated with a longer length of stay. Bartin et al. 12 compared post-surgical serum IL-6 levels in two groups of patients according to the surgical techniques and found that laparoscopic appendectomy was associated with lower postsurgical serum IL-6 levels than open appendectomy. Nevertheless, that finding was not consistent with previous works. 13 This work aimed to assess the role of post-operative IL-6 in predicting the clinical evolution of children operated on for PAA
Patients and Methods
Study design
This was a sub-study within the Biomarkers for the Diagnosis of Appendicitis in Pediatrics (BIDIAP) cohort,7,8 an observational prospective study aimed to analyze the discriminatory capacity of several serum biomarkers in the context of PAA. This substudy focused on the changes in serum IL-6 as a potential predictor of clinical evolution of children operated on for PAA.
Pediatric patients who underwent surgery and in whom the histopathologic diagnosis of acute appendicitis was confirmed were included in the study. Patients were classified according to the change between pre- and post-operative IL-6 levels into two groups: patients with IL-6 elevation of >10%, and patients with a minor elevation, no change, or decrease in IL-6 level. Group 2 was used as the reference category in the analyses.
Patients were also stratified based on their histopathologic analysis of the appendix. Congestive, phlegmonous, or suppurative appendicitis were considered uncomplicated appendicitis, and gangrenous or perforated appendicitis were considered complicated appendicitis. Sociodemographic, clinical, analytical, surgical, radiologic, and histologic variables of all patients were extracted from participants' clinical records.
Patients were recruited in the Emergency Department of our hospital when the personnel conducting the investigation were present. The recruitment period extended from February to December 2021. All patients were followed up on an outpatient basis for one month after the intervention.
Sample collection
Two venous peripheral blood samples were obtained from each patient in a vacutainer tube with separator gel (3.5 mL). In all patients, the first sample was obtained at the time of inclusion in the study, during their stay in the Emergency Department. Subsequently, 12 hours after surgery, the second sample was obtained following the same procedure. Serum samples were processed by laboratory personnel blinded to the patient's group. All the markers were measured in the same sample concurrently.
Measurement of serum IL-6 levels
Serum IL-6 determinations were made by a chemiluminescent assay on an Immulite 2000 XPi analyzer (Siemens Heathineers, Siemens Healthcare GmbH, Germany®).
Discharge criteria
This study was carried out in a Spanish tertiary center, with full public coverage and no fast-track protocol implemented for this pathology. The criteria used to indicate patient discharge were: adequate oral tolerance; pain controlled with oral analgesia; adequate mobilization; absence of post-operative complications; and complete intravenous antibiotherapy regimen proposed by the surgeon.
In the case of our center, intravenous antibiotherapy of patients is based on intra-operative findings, and is generally as follows: uncomplicated PAA (congestive, catarrhal, phlegmonous): 24 hours of intravenous antibiotherapy; complicated PAA (gangrenous, perforated): three to five days of intravenous antibiotherapy; and diffuse peritonitis: seven days of intravenous antibiotherapy.
Statistical analysis
Given the absence of specific precedents in scientific literature, it was not possible to calculate the sample size before carrying out the study.
For descriptive purposes, we used means and standard deviations or medians and interquartile ranges (IQR) for quantitative variables and proportions for categorical ones. The Kolmogórov-Smirnov test was used to assess the normality of quantitative variables. Sociodemographic and clinical variables were compared between groups using Fisher exact test, Mann-Whitney U test, and Kruskall Wallis test.
Regarding the choice of the cut-off point in the post-operative increase of serum IL-6 (>10%), we performed the initial approximation using univariable logistic regression models (receiver operating characteristic [ROC] analysis) for the different dependent variables (peritoneal fluid culture, hospitalization time) and subsequently we opted for the nearest whole number to simplify its implementation in clinical practice.
Three different multivariable-adjusted linear regression models were fitted to analyze the association between an increase of >10% in post-operative serum IL-6 level with the length of stay, the number of emetic episodes, and the onset of oral feeding. These models were adjusted for the patient's age (continous), gender (female vs. male), pre-operative IL-6 values (continuous), length of surgery (continuous), type of surgery (continuous), surgical technique (1. transumbilical laparoscopic-assisted appendectomy [TULA], 2. three port conventional laparoscopy, 3. TULA + conversion to laparotomy, 4. laparotomy, 5. TULA [using an HARMONIC FOCUS™ from Ethicon © and a Endo GIA™ Tri-Staple technology™ with a 45 mm purple charge from Medtronic ©] and type of appendicitis (complicated vs. uncomplicated). Additionally, 2 multivariable-adjusted logistic regression models were fitted to assess the association of the same exposure (an increase of >10% in post-operative serum IL-6 level) with the indication of antibiotherapy at discharge and positivity in the peritoneal fluid culture. These models were adjusted for the patient's age (continuous), gender (female vs. male), pre-operative IL-6 values (continuous), and type of appendicitis (complicated vs. uncomplicated). Statistical significance was settled in a p value <0.05. Statistical analysis was performed with STATA, version 17.0 (StataCorp LCC, College Station, TX).
Research ethics board committee
This study was approved by our center's clinical research ethics committee on December 18, 2020, under code PI_2020/112. The ethical principles of the Declaration of Helsinki were applied to the conduct of this research study. The parents or legal representatives of all participants signed an informed consent form before their inclusion in the study.
Result
Demographic, clinical, and analytical characteristics
The BIDIAP cohort included 99 patients with confirmed diagnosis of PAA. Among these, 30 were excluded because of missing data in either pre- or post-operative serum IL-6 values. The remaining 69 patients were classified into group 1) those with an increase of >10% in post-operative serum IL-6 level (n = 13) and group 2) those with a minor increase, no change, or a decrease in post-operative serum IL-6 level (n = 56). No differences were found between included (n = 69) and excluded (n = 30) participants in sociodemographic characteristics (data not shown).
Participants' sociodemographic, clinical, and analytical characteristics by group are shown in Table 1. Regarding sociodemographic variables, a significantly higher mean body mass index was found in children in group 1 than in their peers in group 2 (p = 0.04). Pre-operative serum IL-6 values (expressed as median [IQR]) were 33.5 (12.2–95.1) pg/mL in group 1 and 21.7 (12.9–48.15) pg/mL in group 2 (p = 0.59). Post-operative serum IL-6 values (expressed as median [IQR]) were 128 (31.3–321) pg/mL in group 1 and 6.25 (4.05–12.6) pg/mL in group 2 (p < 0.0001). We also found differences between groups in the length of hospitalization (p = 0.02) and in the number of emetic episodes on the second postoperative day (p = 0.003).
Sociodemographic and Clinical Characteristics of the Study Groups
Numbers are mean (standard deviation) or number (percentage).
PAA = pediatric acute appendicitis; CRP = C-reactive protein; PCT = procalcitonin; IL-6 interleukin-6.
Comparison between groups 1 and 2.
Median, interquartile range.
Multivariable-adjusted regression analysis
After adjusting for the patient's age, gender, surgical technique, pre-operative IL-6 value, and type of appendicitis, children who presented an increase of >10% in post-operative serum IL-6 value had a mean of three-day longer stay at the hospital (95% CI, 0.78–5.76). Additional adjustments for the duration of the surgery did not change the results (Table 2). Figure 1 shows the difference and 95% confidence interval in the length of hospital stay associated with each factor in the most adjusted model and shows that, after accounting for all the confounders, >10% increase in post-operative IL-6 is the only predictor associated with the outcome.
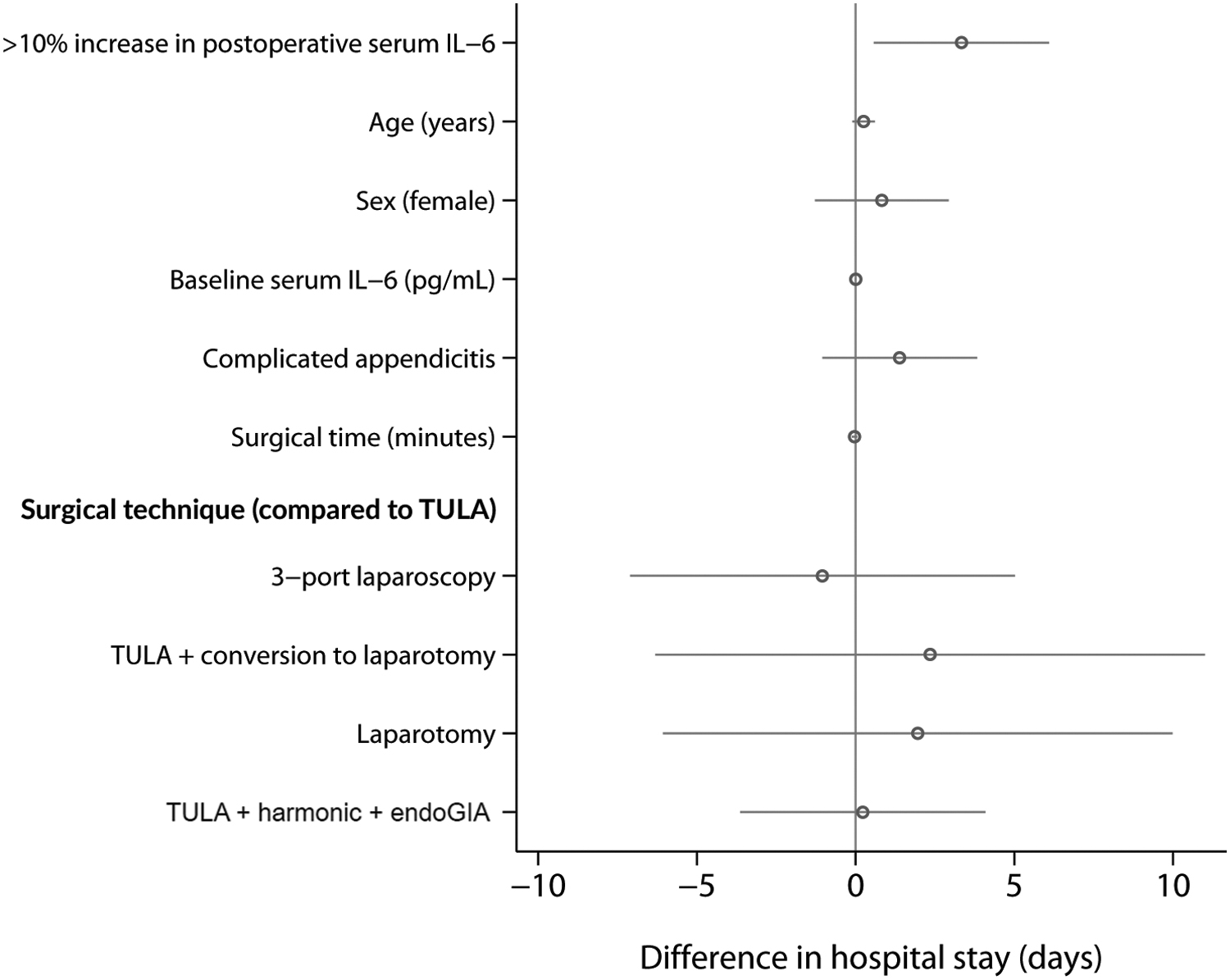
Linear regression model for the association between the increase of post-operative serum IL-6 value and the length of stay at hospital adjusted for patient's age (continuous), gender (female vs. male), pre-operative serum IL-6 value (continuous), surgical technique (TULA vs. three-port laparoscopy, TULA + conversion to laparotomy, laparotomy and TULA + harmonic + EndoGIA), surgical time (continuous) and type of PAA (complicated vs. uncomplicated). TULA = transumbilical laparoscopic-assisted appendectomy; PAA = pediatric acute appendicitis; IL-6 = interleukin-6.
Multivariable Adjusted Linear Regression Analysis for the Length of Admission, the Number of Emetic Episodes in the Second Twenty-Four Post-Operative Hours and the Onset of Oral Feeding Associated With an Increase of >10% in Post-Operative Serum Il-6 (group 1 vs. 2)
All analysis were adjusted for age, gender, pre-operative serum IL-6, surgical time, surgical technique, and type of PAA (complicated vs. non-complicated).
CI = confidence interval; IL-6 = interleukin-6; PAA = pediatric acute appendicitis.
Children who presented an increase of >10% in post-operative serum IL-6 value had a higher number of emetic episodes on the second post-operative day (difference, 0.87; 95% CI, 0.21–1.53) after accounting for patient's age, gender, surgical technique, pre-operative IL-6 value, and type of appendicitis. Nevertheless, this association became not significant after further adjustment for the duration of the surgery (Table 2). No association was found between post-operative serum IL-6 increase and the onset of oral feeding in any of the fitting models (Table 2).
Logistic regression models showed (Table 3) that children who presented an increase of >10% in post-operative serum IL-6 value had 37 times higher odds of showing a positive result in peritoneal fluid culture (OR, 37.43; 95% CI, 1.02–1361.28) than children with minor or no increase in postoperative IL-6 value after accounting for all potential confounders. On the other hand, no associations were found between the post-operative increase in serum IL-6 and the odds of needing oral antibiotherapy at discharge (Table 3).
Multivariable Adjusted Logistic Regression Analysis for the Indication of Oral Antibiotherapy at Discharge and Positivity of Peritoneal Culture Associated With an Increase of >10% in Post-Operative Serum IL-6 (group 1 vs. 2)
All analysis were adjusted for age, gender, pre-operative serum IL-6, and type of PAA (complicated vs non-complicated).
OR = odds ratio; CI = confidence interval; IL-6 = interleukin-6; PAA = pediatric acute appendicitis.
Additional adjustments in all models for weight did not modify the results obtained.
Discussion
Interleukin-6 is a proinflammatory cytokine secreted by multiple human cell lines in relation to pathogen-associated molecular patterns. IL-6 is involved in multiple defense functions: it acts as an endogenous pyrogen, promotes the release and synthesis of liver acute phase reactants and increases vascular permeability. Pediatric acute appendicitis is a focal inflammatory/bacterial infectious process that can present with bacterial translocation, hematogenous dissemination, and sepsis (especially in complicated PAA). Interleukin-6, extensively related to bacteremia and sepsis, is elevated in PAA because of this pathophysiologic phenomenon. Regarding its diagnostic performance in this pathology, it is considered good, with recent studies reporting an area under the curve (AUC) of 0.83 for the diagnosis of PAA and 0.77 for the distinction between complicated and uncomplicated PAA. 8
In this study, we analyzed the possible role of increased serum IL-6 values (value at 12 hours after surgery compared with the pre-operative value) as a predictor of clinical outcome in children operated on for PAA and found that, after accounting for all potential confounders, children that presented >10% increase in post-operative IL-6 value had a mean 3-day longer stay at the hospital and higher odds of obtaining a positive peritoneal fluid culture than those with minor or no increase.
Regarding the length of stay, we believe this finding could be because children who showed >10% increase in serum IL-6 values probably had a higher degree of systemic inflammation, which might prolong their post-surgical recovery. It is noteworthy that the association observed between IL-6 increase and a longer hospital stay was independent of the surgical technique and the duration of the surgery, which are sources of metabolic aggression. Although we cannot reliably prove the presence of bacterial translocation in our patients because of the absence of targeted microbiologic studies, it must be another potential hypothesis to consider in this scenario.
The increased odds for a positive result in peritoneal fluid culture is biologically plausible given that IL-6, apart from an acute phase reactant, is a marker of sepsis. However, we acknowledge that the estimate found in this study could just represent the upper limit of the true association, which might lay within the presented confidence interval. Antibiotic resistance, nonetheless, was not associated with the increase in IL-6 level.
After accounting for the duration of the surgery, the association between IL-6 increase and the number of emetic episodes became not significant. Although the duration of surgery did not result in an independent predictor of post-operative emesis in our analyses, we still believe that, based on biological arguments, the previously described association between the postoperative increase in serum IL-6 and the number of emetic episodes could be confounded by the duration of the surgery.
There are other variables of potential interest in this study such as the presence of surgical site infection or the need for re-intervention. Although we believe there could be a potential association between pre- and post-operative IL-6 levels and these variables, in our cohort, we did not encounter any of the aforementioned events and therefore could not assess this relation.
A relevant aspect when introducing a new biomarker into clinical practice is its cost and processing time. In our case, the processing cost of IL-6 is 8.9 euros (URV, 2020) and the processing time is approximately 60 minutes, which makes it easily implementable in clinical practice if proven useful.
Regarding the optimal time for post-operative determination of IL-6, in our case, it was established by consensus at 12 hours post-operatively. Although, indeed, IL-6 usually shows peak elevation at 24 to 72 hours after inflammatory/infectious insult, in this scenario our patients already had baseline inflammatory/infectious insult since PAA. On the other hand, the existing literature in this specific context is very limited. Future studies with serial determinations at different post-operative points may contribute to defining the best time for this determination in terms of diagnostic and prognostic performance.
Despite our findings, we must acknowledge some limitations.
First, post-operative control of the IL-6 value was conducted 12 hours after surgery. Therefore, changes in serum IL-6 values that may have occurred before that time and their association with oral tolerance could not be assessed. Second, the exclusion of patients because of missing data in serum IL-6 value could have resulted in a selection bias and resulted in a limited sample size. Specifically, the fact that the group with increased IL-6 had only 13 observations constitutes a major limitation when extrapolating these results. Furthermore, this may explain the wide confidence intervals we obtained in some analyses. However, we believe that a thorough sociodemographic and clinical comparison between included and excluded patients demonstrates that selection bias is unlikely.
Third, this is a substudy of BIDIAP, 14 whose primary objective was the evaluation of diagnostic performance tools in PAA. For this reason, variables of potential relevance for this analysis such as the presence of postoperative leukocytosis, tachycardia, or fever were not collected, which limits the analyses of this work. Last, because of the observational design of this study, we cannot rule out the possibility of residual confounding by variables that we did not account for, such as surgical debridement or digitoclasia.
On the other hand, this study has several strengths. First, we followed a rigorous methodology, including laboratory staff blinded to the participant's group. Second, we performed several multivariable-adjusted regression models that account for the most common confounding factors.
Conclusions
In conclusion, this study showed that a >10% increase in post-operative serum IL-6 value could predict longer hospital stays and higher odds of a positive peritoneal fluid culture. This opens the door to the creation of specific algorithms with pre- and post-operative IL-6 determination as a predictive tool for the duration of hospitalization and as a potential tool for guiding the timing and spectrum of post-operative intravenous antibiotherapy. Future prospective studies with large sample sizes and thorough control of confounding (i.e., digital debriding, the use of irrigation-aspiration) are needed to replicate these findings and to broaden the range of biomarkers that could predict post-operative evolution of children operated on for PAA.
Footnotes
Acknowledgments
We would like to highlight the excellent work developed by the nursing team of our Pediatric Hospitalization Area during the recruitment of patients for this study. Their dedication, care, and patience have been essential. We would also like to thank Helen Williams, for her excellent work in the English revision of this work.
Authors' Contributions
Conceptualization and study design: Arredondo Montero, Martín-Calvo. Literature search and selection: Arredondo Montero, Martín-Calvo. Recruitment: Arredondo Montero, Antona. Data curation and extraction: Arredondo Montero, Martín-Calvo, Antona. Formal analysis: Arredondo Montero, Martín-Calvo. Investigation: Arredondo Montero, Martín-Calvo. Methodology: Arredondo Montero, Martín-Calvo. Project administration: Arredondo Montero, Martín-Calvo. Resources: Arredondo Montero, Martín-Calvo. Validation: Arredondo Montero, Martín-Calvo.
Laboratory determinations: Rivero Marcotegui. Visualization: Arredondo Montero, Martín-Calvo. Writing—original draft: Arredondo Montero, Martín-Calvo, Fernández-Celis, López-Andrés.
Writing—review and editing: Arredondo Montero, Martín-Calvo, Antona, Rivero Marcotegui, Bardají Pascual, Fernández-Celis, López-Andrés.
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
Data Availability
All data of this study are available upon justified request through the author in correspondence.
Funding Information
This study has not received external funding. None of the authors have financial disclosures to declare.
Author Disclosure Statement
No financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article.
The Research Ethics Board committee of our center (Hospital Universitario de Navarra) assessed this project under registration code PI_2020/112 and approved it on December 18, 2020.
Before inclusion in this study, all the legal guardians of the patients involved in the study gave their verbal and written consent through an informed consent form.