
Abstract

To the Editor:
P
A 54-year-old female sought medical attention because she felt a painless lump on the left side of her face. Physical examination found a lump approximately 3 × 3 cm in size that was hard with poor mobility was palpable on the left side of her face. No obvious abnormal indicators were found in relevant laboratory tests. The patient denied a previous history of tuberculosis infection and contact.
After completing an enhanced computed tomography (CT) of the maxillofacial region, a quasi-circular mass approximately 3 × 3 cm in size was seen in the left parotid gland, with regular shape and clear boundary (Fig. 1). Based on the relevant patient data, it was considered to be a benign tumor of the parotid gland. After consultation, the patient and her family requested surgical treatment. The patient then underwent a parotid mass excision, where the mass was removed completely. Histopathology of the parotid gland mass after operation showed granulomatous inflammation with caseous necrosis (Fig. 2). The final diagnosis was primary tuberculosis of the parotid gland. After incision recovery, the patient was referred to the infectious ward for antituberculous therapy, and the prognosis was good.
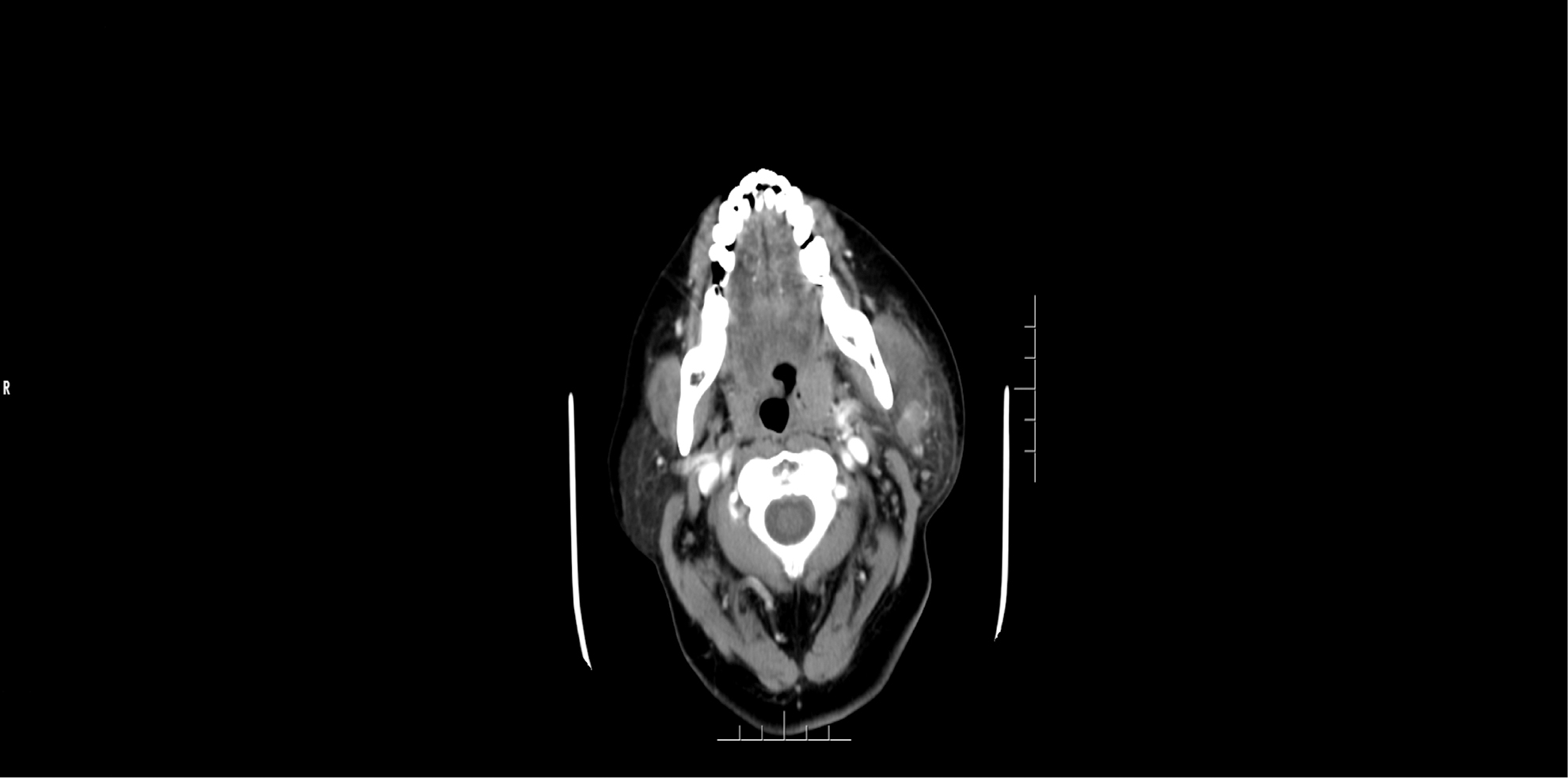
Maxillofacial enhanced computed tomography (CT) showed that there was a quasi-circular mass approximately 3 × 3 cm in size in the left parotid gland, with regular shape and clear boundary.
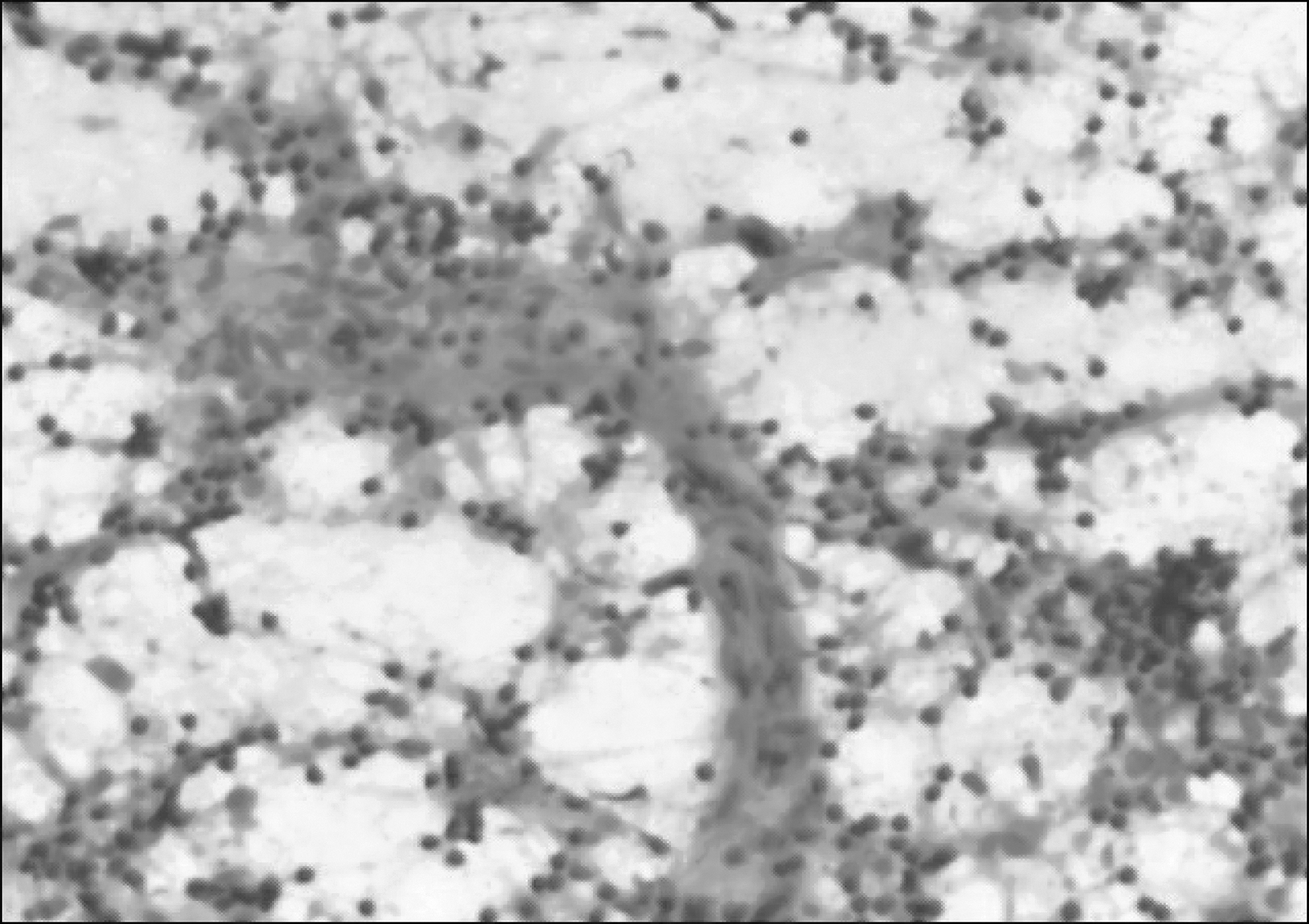
Histopathology of parotid gland mass after operation showed granulomatous inflammation with caseous necrosis.
The parotid gland is the most commonly affected site of salivary gland tuberculosis. It is a slow growing painless mass and is easily confused with benign parotid tumors. Parotid tuberculosis can occur in the early stage of the disease, causing confusion.2,3 The initial manifestations of primary parotid tuberculosis are mostly painless masses. Compared with parotid tumors, primary parotid tuberculosis has no special clinical and imaging manifestations, which leads to frequent misdiagnosis. Diagnosis is often dependent on histopathologic examination. Fine-needle puncture is also useful in detecting the disease but depends on the accuracy of the material collected. Because this disease can lead to serious complications such as facial ulceration and disfigurement, early diagnosis and treatment are particularly important. The prognosis of this disease is good, and once diagnosed, regular antituberculosis therapy should be carried out. For painless masses of the parotid gland, the possibility of tuberculosis should be considered when considering diagnosis to avoid misdiagnosis.