
Abstract
Background:
Prosthesis-related infections (PRIs) and surgical site infections (SSIs) remain one of the most devastating complications among patients undergoing clean orthopedic surgeries. Prevention strategies are critical to reduce infection rates in orthopedic surgeries. The current study aimed to determine the effectiveness of a set of evidence-based practices (bundled intervention) in reducing the incidence of PRIs and SSIs among patients undergoing clean orthopedic surgeries with hardware implants.
Patients and Methods:
A prospective, interventional randomized controlled trial was conducted for a period of three years. A total of 597 patients were enrolled, and depending on their Staphylococcus aureus carrier status were categorized into carrier group (n = 98) and non-carrier group (n = 499). Only carrier group patients were analyzed for effectiveness of bundled interventions, after being randomly assigned to two subgroups: interventional carrier group (ICG; n = 50) and non-interventional carrier group (NICG; n = 48).
Results:
Of the 597 patients, 98 (16.4%) were colonized with Staphylococcus aureus, among whom 9 (19.4%) had methicillin resistance. During follow-up, overall infection rate of 1.1% was observed (PRI, 0.3%; SSI, 0.8%). There was no case of PRI/SSI in the ICG. However, in the NICG, one patient developed SSI because of methicillin-resistant Staphylococcus aureus. An endogenous source of infection was demonstrated by pulsed field gel electrophoresis (PFGE). The SSI rate was higher in the NICG (p = 0.002). In the non-carrier group (n = 499), SSIs/PRIs occurred among 1.2% of the patients, because of organisms other than Staphylococcus aureus.
Conclusions:
Benefit of bundle intervention approach could be demonstrated. Further studies assessing the effectiveness of the individual components of the bundle can inform clinical practice greatly.
Prosthesis-related infections (PRIs) and surgical site infections (SSIs) remain one of the most devastating complications among patients undergoing clean orthopedic surgeries with hardware implants.1,2 Both PRIs and SSIs have dire implications for the surgeon, patient, and the hospital. In addition to accounting for nearly 20% of unplanned re-admissions, these infections could result in additional surgical procedures, prolonged hospitalization, increased hospital expenses, and may double the risk of patient mortality.3,4 Thus, a reduction in the rate of PRIs and SSIs can lead to both better clinical outcomes for patients and cost savings for hospitals.
Staphylococcus aureus accounts for most PRIs and SSIs in orthopedic patients with methicillin-resistant Staphylococcus aureus (MRSA) being of particular concern. The potential of this organism to form biofilms on orthopedic implants further compromises the efforts to eradicate such infections. 5 It is estimated that Staphylococcus aureus colonizes the anterior nares in approximately 31% (range 6-56%) of the general population at any given time. 6 Nasal carriage of Staphylococcus aureus has been epidemiologically linked to development of Staphylococcus aureus PRIs and SSIs in orthopedic surgery. In general, patients who are carriers of Staphylococcus aureus are two to nine times more likely to develop such infections. 7
Although Staphylococcus aureus remains the single most common organism, a large proportion of these infections are still caused by gram-negative bacteria (GNB) that have been described as the second most common cause of PRIs or SSIs in patients undergoing primary total joint arthroplasty. 8 Although most Staphylococcus aureus infections are caused by the patient's own endogenous flora, GNB infections are caused by contamination of the wound or skin by environmental microbes originating from non-disinfected skin or wound areas. 9
It has been estimated that approximately 40% to 60% of SSI cases are actually preventable and hence prevention strategies in reducing the infection rates in orthopedic surgeries are critical.10–13 However, prevention of PRIs and SSIs in orthopedic surgery has certain specificities unknown to general surgery: low inocula for implant-related foreign body infections; pathogenicity of skin commensals; a possible hematogenous origin for some infections; and the necessity for a prolonged, post-discharge surveillance period with a minimal follow-up of one year for implant-related surgeries.14,15 Previous studies conducted over the past decade sought to identify patients at risk for the development of PRIs or SSIs and determine methods to reduce the incidence of such infections by altering modifiable risk factors and minimizing pre-operative, intra-operative, and post-operative risk factors.12,16 However, evidence-based consensus guidelines on the prevention of PRIs and SSIs continue to be heterogeneous and there is little consensus on the optimal intervention implementations both within and across hospitals.8,17–19
Recently, bundled intervention comprising: pre-operative screening for nasal carriage of Staphylococcus aureus and decolonization with intra-nasal mupirocin in combination with chlorhexidine gluconate (CHG) bathing; targeted peri-operative antimicrobial prophylaxis (effective against gram-positive as well as gram-negative bacteria); and post-operative follow-up has gained much attention.20–22 A bundle is a set of evidence-based guidelines that, when implemented together, yield better patient outcome while minimizing the rate of infection and incurred cost. The current study was undertaken to determine the effectiveness of a set of evidence-based practices (bundled intervention) in reducing the incidence of PRIs and SSIs among the patients undergoing clean orthopedic surgeries with hardware implants.
Patients and Methods
Study design and study setting
This prospective study, an interventional randomized controlled trial, was conducted at a 2,500-bed tertiary care hospital and national referral center of India. Patients were enrolled for the study after registration of the study protocol in Clinical Trial Registery of India (CTRI/2016/03/006767, dated 30.03.2016 ) and approval was obtained from Institutional Ethics Committee (IEC-147/04.03.2016, RP-1/2016, dated March 18, 2016).
Study population
A brief study protocol was explained to the study participants and their written informed consent was sought. All consenting adult patients (≥18 years) undergoing clean orthopedic surgery with hardware implants from October 10, 2019 to October 9, 2022 were enrolled. Patients younger than 8 years of age, patients with revision or dirty surgeries, or with pre-existing infections at the surgical site were excluded.
Depending on their Staphylococcus aureus (methicillin-susceptible Staphylococcus aureus [MSSA] or MRSA) carrier status, patients were categorized into carrier group (n = 98) and non-carrier group (n = 499). According to an assignment sequence prepared in advance on an online randomization tool, carrier group patients were randomly assigned to interventional carrier group (ICG; n = 50) and non-interventional carrier group (NICG; n = 48). Only those patients colonized with Staphylococcus aureus (carrier group), were analyzed to determine the effectiveness of bundled interventions, after being randomly assigned to ICG and NICG (Fig. 1). The demographic details, relevant clinical history, associated risk factors and co-morbidities of the study participants were noted prospectively.
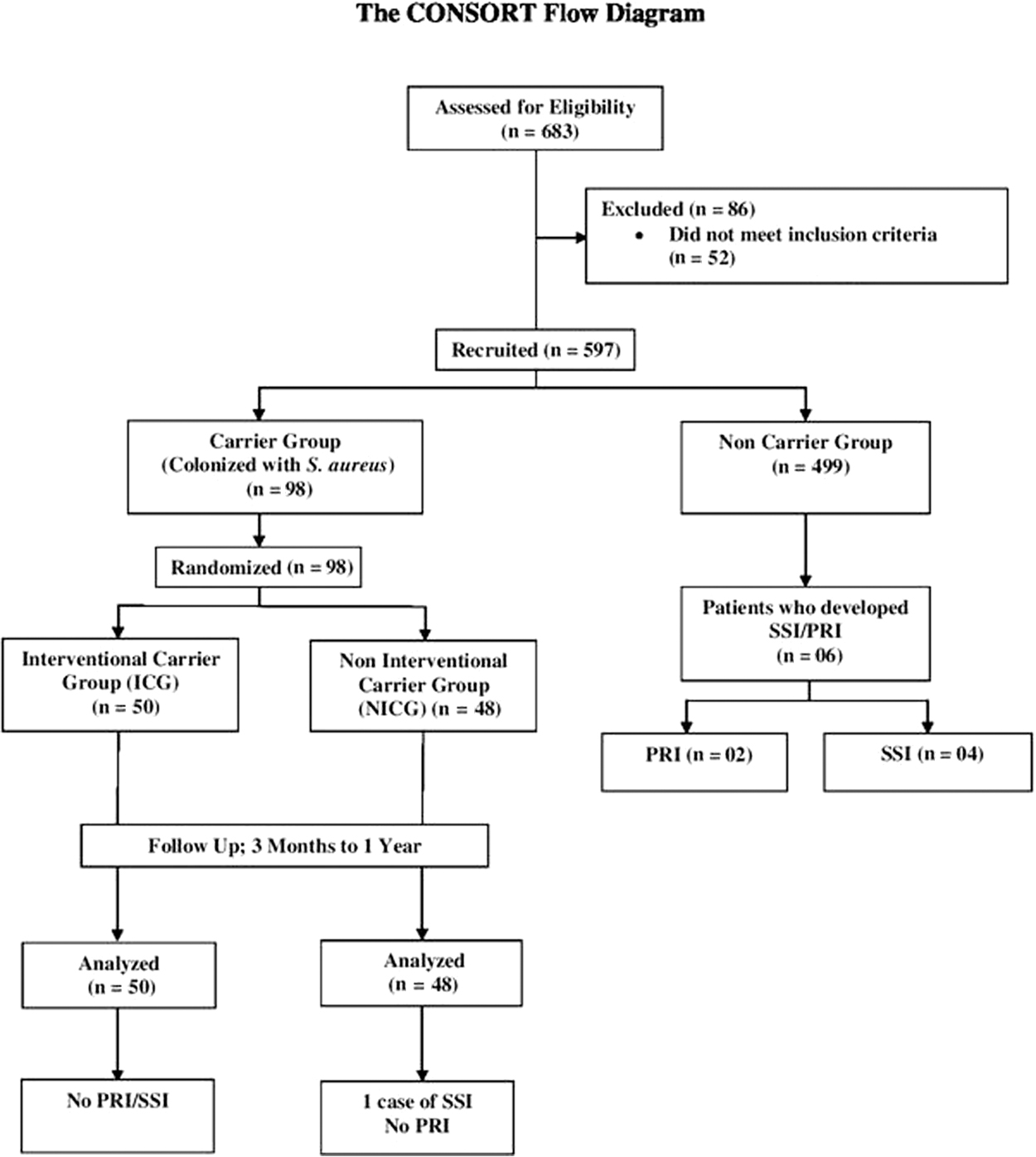
Consolidated Standards of Reporting Trials (CONSORT) flow diagram of patient categorization. PRI = Prosthesis-related infections; SSI = surgical site infection; S. aureus = Staphylococcus aureus.
Bundled interventions
The intervention consisted of 11 processes throughout the surgical encounter, including pre-operative, peri-operative, and post-operative elements (Table 1). Briefly, the eligible patients were screened for Staphylococcus aureus during their scheduled pre-operative clinic visits (10–14 days prior to surgery, but no more than 30 days). Patients with positive screening tests for either MSSA or MRSA followed a decolonization protocol, wherein they applied 2% mupirocin intranasally twice daily for five days prior to surgery and wiped the body (especially the area to be operated) with a set of 2% CHG wipes once daily for four days prior to and the day of surgery.
Bundled Interventions to Reduce the Rate of Prosthesis-Related Infections/Surgical Site Infections Among the Patients Undergoing Clean Orthopedic Surgeries with Hardware Implants
CHG = chlorhexidine gluconate; OR = operating room.
Targeted peri-operative antimicrobial prophylaxis was administered as per the 2013 American Society of Health System Pharmacists (ASHP) guidelines. 23 The antimicrobial agents to be used varied by the patient's Staphylococcus aureus carrier status; MSSA carriers received cefuroxime, whereas MRSA carriers received cefuroxime and vancomycin. In case of confirmed allergy, β-lactam antimicrobial was replaced by gentamicin and vancomycin was replaced by daptomycin.
All patients received standard follow-up care and were monitored for subsequent development of PRIs/SSIs up to minimum of three months and maximum of one year. Joint radiographs were taken and the surgical site was evaluated for any PRIs/SSIs at each follow-up appointment at one week, six weeks, three months and later if required, depending on the patient's clinical condition. The attending clinician obtained clinical samples if any infection was suspected during the follow-up period and the culture results were also documented.
Bundled interventions were implemented on the patients recruited in ICG whereas the NICG patients served as the prospective controls and followed the usual practice of our hospital, i.e., pre-operative bathing with plain soap on the day of surgery and peri-operative antimicrobial prophylaxis (cefuroxime only). Patients assigned to the non-carrier group (n = 499) also followed the usual practice of our hospital.
Surgical site infections and PRIs were defined and classified as per the definitions established by the U.S. Centers for Disease Control and Prevention (CDC) and Musculoskeletal Infection Society (MSIS) criteria, respectively.24,25
Details of the optimization, evaluation, preparation, and use of 2% CHG wipes is described in the Supplementary Appendix.
Laboratory methods
Nasal screening for Staphylococcus aureus carriage was implemented as standard of care and samples for the same were collected from anterior nares of all the patients. Swabs were plated onto blood agar (BA) and mannitol salt agar (MSA) and incubated aerobically for 24 to 48 hours. Colonies demonstrating β-hemolysis on BA and growth on MSA were identified preliminarily as Staphylococcus aureus and confirmed by MALDI-TOF MS (BioMerieux, Manchester, United Kingdom). All the Staphylococcus aureus strains were stocked in 30% glycerol and stored at −70°C until further molecular confirmation and characterization by multiplex polymerase chain reaction (M-PCR) and pulsed field gel electrophoresis (PFGE), respectively.
Clinical samples from suspected cases of PRIs/SSIs included, blood, pus, synovial fluid, peri-prosthetic tissue, and explanted prostheses and were further processed and identified using standard procedures.26,27 Antimicrobial susceptibility testing (AST) was done by Kirby-Bauer disk diffusion method on Muller-Hinton agar and the results were interpreted in accordance with Clinical Laboratory Standard Institute (CLSI) guidelines. 28 Cefoxitin (30 mcg) disk was used as a surrogate marker to determine methicillin resistance. Mupirocin (200 mcg) disk (Oxoid, Basingstoke, England) was used to determine mupirocin resistance. Inducible resistance to clindamycin in macrolide-resistant strains of Staphylococcus aureus was detected by a standardized disk approximation test. 28 Vancomycin susceptibility was determined by broth microdilution method.
Molecular confirmation of the Staphylococcus aureus isolates with simultaneous detection of methicillin and mupirocin resistance was done by performing a M-PCR targeting femB, mecA, and iles2 genes, respectively, as described elsewhere. 29 Clonal relation between pre-decolonization Staphylococcus aureus isolates and the Staphylococcus aureus isolates from PRIs/SSIs was determined by PFGE as described previously.29,30 Genotypic characterization of the isolates was done by macrorestriction analysis using the restriction endonuclease Sma1 (New England Biolabs).
Statistical analysis
The study was reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) Statement and ICH guidelines for Good Clinical Practice (GCP). All study data was managed by STATA, version 14 data analysis statistical software (StataCorp LP, College Station, TX). Confidentiality of participant data was assured according to GCP.
Results
A total of 597 patients were included in the study. Of these, 226 (37.8%) underwent total knee replacement, 158 (26.5%) underwent total hip replacement, 108 (18.1%) underwent spine surgeries, and the remaining 105 (17.6%) underwent other clean orthopedic surgeries. Of the total 597 patients, 298 (49.9%) were male. The mean age of the patients was 45.1 ± 3.0 years.
Of the 597 patients, 98 (16.4%) were colonized with Staphylococcus aureus (carrier group) and were included for analyzing the effectiveness of bundled intervention by randomly assigning them to two subgroups ICG (n = 50; 51%) and NICG (n = 48; 49%). Among the patients colonized with Staphylococcus aureus, 19 (19.4%) had MRSA carriage. No discrepancy was observed between the detection of methicillin and mupirocin resistance by disk diffusion method and multiplex PCR.
The demographic characteristics of the patients assigned to ICG and NICG are summarized in Table 2. Staphylococcus aureus nasal carriage was significantly observed in patients with underlying osteoarthritis/rheumatoid arthritis. Demographic details of the non-carrier group are available in Supplementary Table S1.
Demographic Characteristics of the Patients Assigned to Interventional Carrier Group and Non-Interventional Carrier Group (n = 98)
BMI = body mass index; CVD = cardiovascular disease; ICG = interventional carrier group; NICG = non-interventional carrier group; OSAS = obstructive sleep apnea syndrome.
During follow-up, a total of seven patients developed PRIs/SSIs with an overall infection rate of 1.1% (PRI, 2; 0.3%; SSI, 5; 0.8%). Among the carrier group patients, no case of SSI or PRI was observed in the ICG subgroup, however, in the NICG subgroup, one patient developed SSI due to MRSA within three months of surgery. On comparing the rate of SSI between ICG and NICG, it was found substantially higher in the NICG (0.0% [0/50] vs. 2.1% [1/48]; p = 0.002) subgroup. No case of PRI was found in the carrier group.
Among the patients in the non-carrier group, PRIs/SSIs occurred in six of 499 patients (1.2%). Two patients developed PRI and four SSI. All the infections were mono-microbial and occurred within three months of the index surgery. None of these infections were due to Staphylococcus aureus thereby suggesting causal relation between Staphylococcus aureus nasal carriage and PRI/SSI. Both cases of PRI were due to GNB. Of the four SSI cases, three were due to GNB and one was due to Enterococcus faecalis. Out of the five GNB isolates, four were multi-drug–resistant. Details of the isolated organisms and their antimicrobial susceptibility profile are available in Supplementary Tables S2 to S7).
Table 3 depicts the comparison of the incidence of PRI/SSI between different subgroups. The rate of SSI among the carrier group was statistically higher than among non-carriers (1.02% [1/98] vs. 0.8% [4/499]; p = 0.012). Off note, there were two cases of PRI in the non-carrier group compared to none in the carrier group (0.4% [2/499] vs. 0/98 [0.0%]; p = 0.00), however, both were due to GNB.
Comparison of the Incidence of Prosthesis-Related Infections/Surgical Site Infections Between Different Subgroups Undergoing Surgery
ICG = interventional carrier group; NICG = non-interventional carrier group; PRI = prosthesis-related infections; SSI = surgical site infection.
Clonal diversity among Staphylococcus aureus isolates
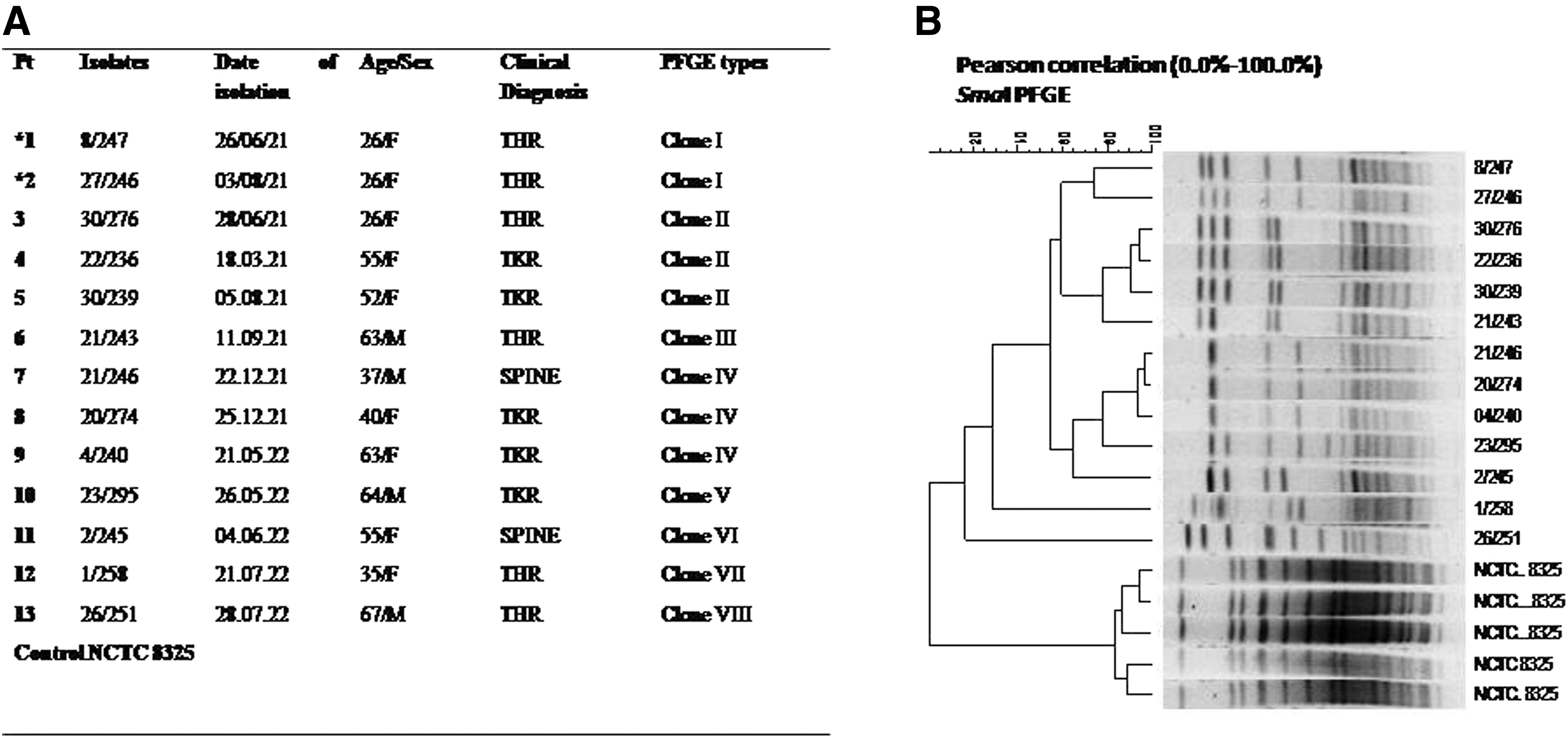
The SmaI macrorestriction fragment profiles of 48 randomly selected Staphylococcus aureus isolates (MRSA, 17; MSSA, 31) were determined by PFGE. In addition, the profile of the two strains of MRSA isolated from the nasal cavity and infection at the surgical site of a patient recruited to the NICG subgroup were also determined. A total of eight clones (I–VIII) were identified. Clone I, III, and VI consisted of only MRSA strains whereas clone IV, V, VII, and VIII consisted of only MSSA strains. Clone II consisted of both MSSA and MRSA strains (Fig. 2 and Fig. 3). The two MRSA strains isolated from the nasal cavity and infection at the surgical site of the same patient were indistinguishable from each other, suggesting that they were derived from a similar clone (clone I).

Pulsed field gel electrophoresis pattern of SmaI macrorestriction fragments of control strain NCTC 8325 (lane 1, 6, 11, 15, and 18) and 13 clinical samples.
Adverse events
Three patients reported mild skin irritation associated with pre-operative use of CHG wipes, however, the symptoms subsided quickly once the usage was discontinued. None of the patients reported any adverse reactions to mupirocin or other antimicrobials used in peri-operative prophylaxis.
Discussion
To the best of our knowledge this is the first randomized control trial from an Indian hospital aimed to determine the impact of bundled care intervention on the outcome of patients undergoing clean orthopedic surgeries with hardware implants.
Both PRIs and SSIs are pharmacotherapeutically and pharmacoeconomically detrimental for the patient. Nasal carriage of Staphylococcus aureus has been identified as a substantial risk factor for infection in general orthopedic surgical services. The combination of pre-operative identification of Staphylococcus aureus colonization followed by active decolonization has been viewed as a pre-emptive strategy for reducing the risk of PRI/SSI. We used a M-PCR assay for the simultaneous identification of Staphylococcus aureus and detection of methicillin and mupirocin resistance. Molecular screening methods have the advantage of high sensitivity, specificity and rapid turnaround time. We observed a 16.4% Staphylococcus aureus colonization rate (MSSA, 13.2%; MRSA, 3.2%).
Topical mupirocin, with or without pre-operative CHG showers and skin wipes, is the current gold standard for nasal decolonization. 31 Nasal mupirocin has been used widely for the suppression of nasal carried Staphylococcus aureus in surgical patients because it is safe, inexpensive, and effective in decolonization. However, a cautionary comment on mupirocin is warranted. Despite all isolates being susceptible to mupirocin both by phenotypic and genotypic methods in this study, mupirocin resistance appears to be increasing worldwide. A previous study from our center reported 5% emergence of high-level mupirocin-resistant isolates from patients with skin and soft tissue infections. 29 Given that at present, mupirocin is the only topical agent documented to eliminate MRSA carriage, its judicial use under antibiotic stewardship guidelines should be ensured. 31 Notably, although mupirocin has been viewed as gold standard for short-term suppression of MRSA, it is less effective as a long-term agent. 31 A study suggests that in hospitalized patients, MRSA can be suppressed successfully (long-term) using a combination therapy of 2% CHG wipes and topical mupirocin, a decolonization protocol followed in our study. 32
Post-operatively, seven cases of PRI/SSI (2 PRI; 5 SSI) were identified in the study group with an overall infection rate of 1.1%. Furthermore, most of the infections occurred in the first three months and were early onset. The proportion is lower in our study compared with the rest of the literature but is comparable with reports from other centers with high operative volume. Various studies have shown that increase in the hospital operative volume results in fewer post-operative complications. 33 The results are reassuring when considering the current standards of care for infection prevention, in addition, ultra-clean operating rooms, dedicated personnel, and improved surgical techniques contribute to the low incidence of post-operative infections observed at our hospital.
A single case of SSI was found in the NICG group compared with none in the ICG subgroup. However, no case of PRI was found in the ICG/NICG after one year of follow-up. The SSI rate was higher in the NICG than among intervention carrier group (p = 0.002). The influence of pre-operative decolonization on PRI/SSI was assessed in a recent meta-analysis by Zhu et al. 19 and the results suggested that Staphylococcus aureus screening reduced both SSI and prosthetic joint infection (PJI) in the decolonization group as was observed in our study.
Genotyping of randomly selected 48 Staphylococcus aureus isolates revealed eight different clones thereby, depicting diversity among the isolates. There is often an erroneous view that Staphylococcus aureus represents a uniform sub population of Staphylococcus aureus. In fact, Staphylococcus aureus comprise a multitude of more or less epidemiologically successful clonal lineages with huge differences and resistance patterns and virulence factors as was also observed in our study. Different clonal lineages may present typical resistance pattern or may be equipped with certain virulence factors. Thus, screening of patients for Staphylococcus aureus and molecular characterization of the isolates is vital for understanding the transmission dynamics of prevalent or emerging genotypes and optimizing the therapeutic measures.
In a major multicenter study by Berthelot et al. 34 focusing on arthoplasties, it was observed that in most cases of Staphylococcus aureus SSI, either an endogenous origin could not be demonstrated or preoperative nasal decolonoization retrieved a strain that was different from the infecting pathogen. Contrary to this study, we demonstrated a causal relation between nasal carriage of Staphylococcus aureus (MRSA) with subsequent SSIs by PFGE. The SmaI macrorestriction fragment profiles of the two MRSA isolates from the nasal cavity and from the infection at the surgical site of our patient recruited in the NICG belonged to the same clone, suggesting an endogenous source of infection. Off note, two cases of PRI and four cases of SSI were found in the non-carrier group due to micro-organisms other than Staphylococcus aureus. Contrary to previous reports2,35 of the predominance of gram positive organisms in PRIs/SSIs, we found predominance of GNB. These findings are important because PRIs/SSIs due to GNB are difficult to treat and clinical outcomes are less favorable. The differences in the study settings and socioeconomic status of the study population from those in other studies could be a plausible reason for these differences.
Many reports in the literature support the view that the use of chlorhexidine reduces the incidence of SSI/PJI after total joint replacement. Kapadia et al. 36 suggested that the pre-operative use of CHG wipes decreases the PRI rate on the total hip arthroplasty. Chlorhexidine is a broad-spectrum biocide effective against gram-positive and gram-negative bacteria. The overall superior protection of chlorhexidine has been attributed to its rapid bactericidal action as well as its residual effect. Two-percent CHG wipes have recently been introduced to improve ease of administration and have been shown to be as effective as 4% chlorhexidine solution in reducing bacterial skin counts. 37 Edmiston et al. 37 demonstrated that patients using 2% CHG wipes had a mean skin chlorhexidine wash concentration ranging from 12.7 to 27.4 times higher than with a 4% chlorhexidine wash at all cutaneous sites tested (p < 0.001). The National Nosocomial Infections Surveillance System also recommends routine skin cleansing with CHG wipes to reduce the incidence of SSI. 38 Because of the wide spectrum action of CHG, we suggest a partial bundle consisting of only 2% CHG wipes five days before surgery may be used in non-carriers for reducing these infections. However, further large-scale studies are required for assessing the adoption of CHG wipes in clinical care for the prevention of PRI/SSI after clean orthopedic surgeries.
This study had limitations. First, even though we found a substantial benefit of bundled interventions in reduction of SSI/PJI, these results should be interpreted with caution because of the small sample size. Second, the cumulative incidence of PRIs/SSIs was calculated by analyzing the data with minimum follow-up of mean 7.5 months (minimum, 3 months; maximum, 12 months). Hence, it was not possible to detect late-onset PRIs. Nevertheless, we do feel that the present data can still be of use for meta-analysis in the future.
Conclusions
To conclude, our data demonstrated the benefit of bundle intervention approach. Further, multicentric studies assessing the effectiveness of this bundled intervention and the individual components of the bundle can greatly inform clinical practice. Given the considerable clinical and economic consequences associated with PRIs/SSIs, the goal of any healthcare system should be zero tolerance to such infections and the associated adverse events. Efforts that move closer to this elusive goal hold tremendous value for clinicians, hospitals, and most importantly, patients.
Footnotes
Acknowledgments
The technical assistance of Ms. Azka Iram is acknowledged. We thank all the nurses and doctors from the participating wards and all others who contributed to this study.
The data of the present study were presented (partly) at the 67th Annual Conference of Indian Orthopaedic Association, Amritsar, Punjab, India, November 28, 2022, to December 3, 2022.
Authors' Contributions
Study concept and design: Dhawan, Juyal. Acquisition, analysis, or interpretation of data: Rawre, Sreenivas, Narayan. Drafting of the manuscript: all authors. Critical revision of the manuscript for important intellectual content: Dhawan, Juyal, Velpandian, Garg, Malhotra. Statistical analysis: Dhawan, Sreenivas. Administrative, technical, or material support: Dhawan, Rawre, Velpandian, Malhotra. Study supervision: Dhawan, Malhotra. Dr. Dhawan had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding Information
This study was supported by Indian Council of Medical Research (ICMR), New Delhi, India under grant no. 5/4-5/3/3/Ortho/Ad-hoc/18-NCD-I.
Author Disclosure Statement
The authors declare that there is no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.