
Abstract
Objective:
Severe neurosurgical central nervous system infections (sNCNSIs) are among the most serious complications of neurosurgical disease. Conventional methods have shown a poor prognosis. This study aims to analyze the clinical characteristics of vacuum-assisted closure (VAC) in sNCNSIs with the help of antibiotic irrigation treatment.
Patients and Methods:
A retrospective study was performed for patients diagnosed with sNCNSIs. A VAC device was placed on the incision after debridement and the surgical cavity was rinsed with antibiotic agents in the VAC group. Meanwhile the surgical cavity was drained after debridement in the control group. Medical data were reviewed and analyzed.
Results:
Twenty-eight patients met the inclusion criteria, including 18 cases in the VAC group and 10 cases in the control group. The basic medical data showed no differences. Bacteria was isolated from 24 (85.7%) patients. The cure rate was significantly higher in the VAC group (p < 0.05). The cure rate in patients with multi-drug–resistant (MDR) infections was significantly higher in patients treated with VAC therapy (p < 0.05). The prognosis evaluated by Glasgow Outcome Score (GOS) between the two groups showed significant difference (p < 0.05). No re-infection in the VAC group occurred in the follow-up period.
Conclusions:
It is suggested that VAC-assisted antibiotic irrigation is safe and effective for patients with severe NCNSIs and can improve the prognosis dramatically. The results can provide a new effective and reasonable therapeutic strategy for patients with sNCNSIs.
Neurosurgical central nervous system infections (NCNSIs) are complex complications in neurosurgery that usually emerged secondary to the neurosurgery, and nearly all of which required further neurosurgical treatment. Many patients experience severe surgical site infections and intra-cranial infection after neurosurgery. More importantly, such patients have a higher mortality because of severe intra-cranial infection. In light of this, we define this type of disease as severe neurosurgical central nervous system infections (sNCNSIs) and its definition is severe post-neurosurgical site infection with pus accumulation, combined with confirmed intra-cranial infection.
The incidence of NCNSIs is 4.6% to 25%, 1 constituting 10% of central nervous infections. 2 The incidence of meningitis after craniotomy is 1.5% to 8.6%, 3 whereas the incidence after traumatic brain injury is 1.4%. 4 The mortality of NCNSIs is 3% to 33%, 5 and the mortality is even higher in sNCNSIs. Treatment of sNCNSIs is expensive, especially for those who require secondary neurosurgery, which leads to severe pain, long length of stay, and poor prognosis.
For patients with sNCNSIs, the traditional neurosurgical methods are debridement surgery and drainage. Former studies have shown that traditional treatment can result in poor prognosis. Vacuum-assisted closure therapy is a proven technique that was introduced by Argenta and Morykwas in 1997, 6 and has been widely used in orthopedics, plastics, burns, and head and neck surgery. There have been studies describing the application of VAC in scalp and periosteal disease defects,7–11 and few referred to the utilization in NCNSIs. Only two studies have concentrated on this aspect and both were case reports,10,11 which may provide an incomplete analysis of the disease. To our knowledge, this is the first study to investigate the application of VAC-assisted antibiotic irrigation in sNCNSIs.
We hypothesized that VAC-assisted antibiotic irrigation would be effective in treatment of sNCNSIs. These data were collected in our department, which serves as the main tertiary treatment center in our province. The aim of this study is to analyze the clinical characteristics of this treatment in sNCNSIs.
Patients and Methods
A retrospective study was conducted at the Neurosurgery Intensive Care Unit of Shandong University Qilu Hospital. With approval from the hospital ethics committee, we identified 28 patients with sNCNSIs who were admitted during the period of July 2016 to April 2022. These patients were transferred from other hospitals in our province. The referring hospitals that transferred patients are the major hospitals in their respective districts. These data make this study important for providing a new efficient treatment.
Clinical manifestation
The inclusion criteria are verified evidence of severe infection at surgical site (pus, necrotic tissues, wound dehiscence) with clinical signs, full thickness wound larger than 10 cm and producing exudate, and verified laboratory abnormalities of NCNSIs. The exclusion criteria are as follows: patients with unstable fatal primary disease; patients with coagulation disorders; and patients with underlying diseases such as severe cardiopulmonary dysfunction.
Indications for the use of VAC therapy are the same as the inclusion criteria. Patients admitted before September 2019 were treated with traditional methods, and patients admitted after September 2019 were treated with VAC therapy.
On admission, all the wounds had inflammatory secretions or pus, but there were no obvious defects. General data were reviewed and collected. These data include general conditions such as age, gender, blood pressure, tobacco and alcohol use, cause of infection, cerebrospinal fluid (CSF) leak, hemiparesis, pupillary function, communication and verbal response, duration of infection prior to presentation, Glasgow Coma Scale (GCS) score, pathogen type, etc.
Surgical technique
Patients were assigned into the VAC group or the control group. For the VAC group, a VAC device was placed on the incision after debridement and the surgical cavity was irrigated with antibiotic agents. For the control group, the surgical cavity was drained simply after debridement and the dressing of incision was changed every two to three days. All patients underwent debridement and drainage tubes were placed in the surgical cavity. All operations were performed by the same senior physician. Dura was sealed during surgery. Fascia lata was taken from the thigh to repair the CSF leak in cases of obvious dural defect. Drainage tubes were placed at subdural or epidural spaces depending on the infection. The surgical cavity was thoroughly rinsed with antibiotic agents during the operation. The antibiotic agents used for intra-operative flushing included amikacin and vancomycin and were selected by pre-operative empirical judgments or laboratory results. If the infection invaded the skull, the bone flap would be removed. All scalps were watertight sutured. Specimens were sent for culture immediately after operation. Intravenous antibiotic agents were administrated after debridement, which included cefoperazone sulbactam, meropenem, vancomycin, linezolid, voriconazole, etc. Sensitive antibiotic agents were immediately administrated after micro-organism culture report.
In the VAC group, at least two drainage tubes were placed in the surgical cavity depending on the circumstance of infection. The negative pressure ranges from 50 to 125 mm Hg. The sponge was changed every seven to nine days if necessary. The surgical cavity was slowly flushed with antibiotic agents through a sterile infusion set attached to one of the drainage tubes and drained through the remaining tubes. Antibiotic agents used for rinsing were dissolved in 250 mL lactated Ringer's solution. The antibiotic agents used for flushing included amikacin, vancomycin, polymyxin B, and amphotericin. The irrigation lasted for at least five hours. Specimens taken from drainage fluid and CSF were sent for culture during therapy.
Debridement would be performed again in following circumstances: the indicators of aspiration fluid taken from the surgical cavity remained abnormal, clinical symptoms had not improved, the flushing was not smooth, and computed tomography (CT) or enhanced CT still showed abnormalities. When the number of white blood cells in the aspiration fluid was less than 100*106/L and clinical symptoms improved, the operative cavity irrigation would be replaced by injection of antibiotic cocktail (proper antibiotic diluted with 5–6 mL normal saline), and the cocktail liquid would be retained for two hours. The dosage of proper antibiotic agents referred to the expert consensus from both China and the United States, which is as follows: amikacin, 20 mg; vancomycin, 20 mg; polymyxin B, 5 mg; and amphotericin, 0.5 mg.3,12 The drainage tubes would be removed when the following conditions were met: for CSF and surgical cavity drainage, indicators had been normalized for three consecutive times within a week (culture negative, routine test met the normal standard); clinical signs of intra-cranial infection disappeared; and CT scan or enhanced CT scan were normal. An example of surgery is shown in Figure 1.
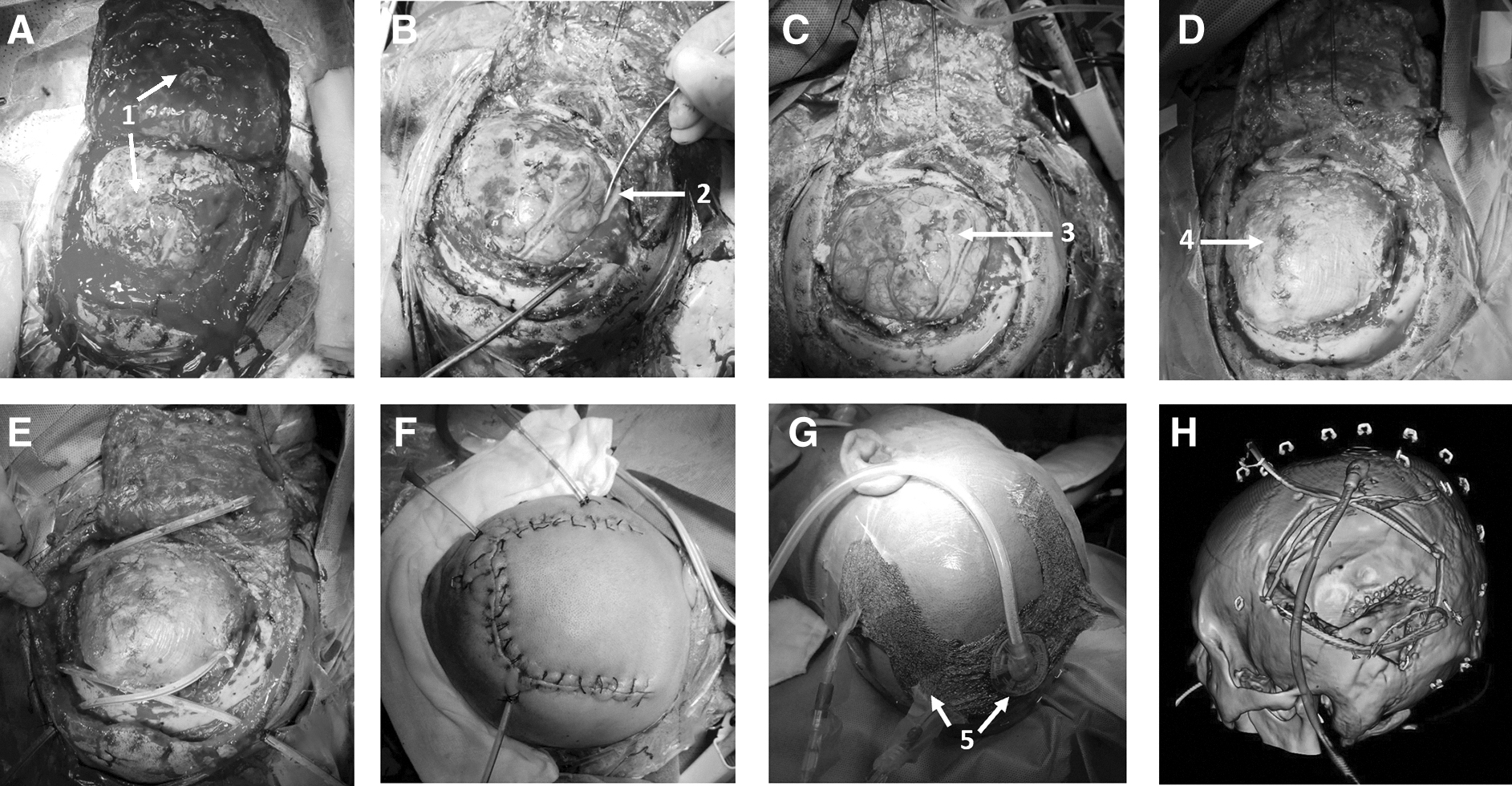
Photographs of a patient during surgery illustrate the surgical treatment in the vacuum-assisted closure (VAC) group patients.
The control group used traditional methods. Drainage tubes were placed and the incision was sutured primarily after debridement. The dressing of the incision was changed regularly. Drainage tubes would be removed for two to three consecutive days with a daily drainage of less than 50 mL.
Follow-up studies were conducted via direct video and outpatient review. The follow-up investigation started from the day of discharge. All the living patients received rehabilitation treatment. Follow-up data include Glasgow Outcome Score (GOS), complications of infection, etc. All patients were followed up for 12 months. The last patient was followed until April 2023. All wounds were visually inspected during follow-up.
Safety monitor
The process of irrigation was kept strictly sterile and the amount of fluid extracted from surgical cavity was monitored. Accidental CSF leakage through VAC drainage tube was also monitored. All patients underwent regular CT scans during the treatment. Any abnormal neurologic function changes would be managed promptly. Hepatic and renal functions were monitored throughout the administration of medication.
Statistical analysis
The data were analyzed using SPSS Statistics, version 25 (IBM Corp, Armonk, NY) and Excel 2016 (Microsoft, Redmond, WA). The collected data that conformed to normal distribution were expressed as mean ± standard deviation. The measured data were analyzed using Student t-test, whereas the categorical variables as number of cases were analyzed using Fisher exact test. The collected data that did not conform to the normal distribution were analyzed by Mann-Whitney U test. A significance difference was indicated by a p level of <0.05.
Results
General information of the patients
Twenty-eight cases were enrolled, which included 20 males (71.4%) and eight females (28.6%). The patient's age ranged from eight to 70 years of age, with a mean age of 40.82 ± 18.649 years. In the VAC group, the patient's age ranged from 14 to 69 years, with a mean age of 42.56 ± 16.249 years. The control group patients ranged in age from eight to 70 years with a mean age of 37.70 ± 22.974 years. In the VAC group, there were 12 males and six females, whereas there were eight males and two females in the control group. General data such as GCS score, etiology, and pathogen types were collected, and no differences were seen between the two groups (Table 1). All patients underwent craniotomy. Before debridement, seven patients retained bone flaps in the VAC group and three patients in the control group retained bone flaps. After debridement, only one patient in the VAC group retained cranial flap. After excluding the patients who died and were automatically discharged, the treatment period for the 17 patients in the VAC group ranged from 11 to 40 days, whereas the treatment period for the six patients in the control group ranged from 14 to 29 days.
Descriptive Characteristics of the Patients
Microbiologic results and systemic medication
Both gram-positive and gram-negative micro-organisms were isolated from the infected incisions. Bacteria were isolated from 24 patients. Although specimens from four patients had no micro-organisms isolated, a clinical diagnosis could still be established based on clinical diagnosis criteria.
Gram-negative bacteria were isolated in 16 patients (66.7%), including Klebsiella pneumoniae, Pseudomonas aeruginosa, Serratia urealyticum, and Acinetobacter baumanii. Ten of the gram-negative bacteria were multi-drug–resistant (MDR) bacteria. Meanwhile, gram-positive bacteria were isolated from eight patients (33.3%), including Staphylococcus epidermidis, Staphylococcus aureus, Staphylococcus capitis, and streptococcus. One of the gram-positive bacteria was MDR organism. One case of Klebsiella pneumoniae infection in the VAC group was cured after treatment, but was followed immediately by a Candida albicans infection, and was clinically cured after continuing treatment in the VAC group (Table 2). In the VAC group, seven patients were infected with MDR bacteria. In the control group, four patients were infected with MDR bacteria (Fig. 2).

Multi-drug–resistant (MDR) bacteria in two groups. VAC = vacuum-assisted closure.
Microbiologic Results of the Patients With sNCNSIs
sNCNSIs = severe neurosurgical central nervous system infections; VAC = vacuum-assisted closure; MDR = mult-drug–resistant.
Bacteria were isolated in 24 patients. Gram-negative bacteria were isolated in 16 patients whereas gram-positive bacteria in eight patients. One patient infected with Klebsiella pneumoniae in the VAC group developed a secondary fungal infection after being cured, and was cured by the same treatment finally.
Accessory examination
Computed tomography examinations were conducted for all patients during hospitalization, with an average of 4.1 CT scans and at least two CT scans for each patient. Six patients received contrast enhanced CT scans.
Safety monitor
Hepatic and renal functions were monitored throughout the treatment. No fatal dysfunction emerged. No evidence of CSF leakage occurred during the treatment. No case of herniation or intra-cranial hemorrhage caused by CSF leakage were observed. Additionally, there was no evidence of new obvious complications during the treatment, such as epileptic seizures, acute hydrocephalus, ischemic stroke, sinus thrombosis, acute neuromuscular blockade, etc.
Outcomes
The criteria for defining a cure that referred to the expert consensus from China and the United States3,12 are as follows. For drainage fluid and CSF (control group only underwent CSF testing), normalized indexes of the following for three consecutive times in one week: negative culture; routine test met normal standard; clinical signs of NCNSIs disappeared; normalization of blood leukocytes and neutrophils (except abnormal elevation caused by infection of other organs); and healed incision.
In the VAC group, 17 patients were clinically cured with a cure rate of 94.4%. Six patients in the control group were clinically cured and the cure rate was 60%. The cure rate was higher in the VAC group (p < 0.05). Patients in both groups who were not cured were automatically discharged or died due to aggravated intra-cranial infection associated with sNCNSIs. For patients infected with MDR bacteria, six ofseven patients in the VAC group were clinically cured, whereas only one out of four patients in the control group was clinically cured. The cure rate in patients with MDR infections was higher in patients treated with VAC therapy (p < 0.05; Table 3).
Comparison of the Therapeutic Outcomes Between the Two Groups
Seventeen (94.4%) patients were clinically cured in the vacuum-assisted closure (VAC) group, whereas six (60%) patients were clinical cured in the control group. For patients infected with multi-drug–resistant (MDR) bacteria, six out of seven patients in the VAC group were clinically cured, whereas only one of four patients in the control group was clinically cured. Both therapeutic outcomes between the two groups showed significant differences.
During the follow-up period, two patients in the VAC group developed hydrocephalus and underwent ventriculoperitoneal shunt. One patient in the control group developed hydrocephalus; the CT scan showed mild dilation of the ventricular system and interstitial cerebral edema, but the symptoms did not improve after the lumbar tap test, and eventually this patient did not undergo neurosurgery. Three patients in the VAC group and one patient in the control group suffered from epilepsy. With an interval of at least six to nine months, 13 patients in the VAC group and three patients in the control group underwent cranioplasty, respectively. No evidence of other complications emerged in the surviving patients. No re-infection occurred in the VAC group after the follow-up period, whereas two patients in the control group developed re-infection and recovered after another debridement (Table 4).
Outcomes, Complications, and Follow-Up Results
VAC = vacuum-assisted closure.
The GOS scores were collected after follow-up (12 months) and were used to evaluate the prognosis. The assessment standard includes excellent, effective, and poor. The recovery criteria are as follows: excellent for GOS score of four to five; effective for GOS score of three; poor for GOS score of one to two. A good outcome is defined as patients with excellent and effective recovery. In this study, the rate of good outcome was higher in the VAC group (p = 0.041; Table 5).
Comparison of the Prognosis Between the Two Groups Using GOS Score
The recovery criteria: excellent, GOS score 4–5; effective, GOS score 3; poor, GOS score 1–2. The total patients with good outcome were defined as those with excellent and effective recovery. In this study, comparison of the prognosis between the two groups using GOS score showed significant differences (p < 0.05).
GOS = Glasgow Outcome Score; VAC = vacuum-assisted closure.
Discussion
Severe NCNSI is a problematic occurrence in neurosurgery. Once an sNCNSI occurs, it causes substantial suffering to patients and leads to poor prognosis. Previous studies have shown that VAC therapy can stabilize the internal environment of incision, increase blood flow in incision, reduce tissue edema, isolate external environmental pollution, etc.13–20 Recently, this therapy has been applied to complex cranial and scalp reconstruction as well as gastrointestinal leakage.21,22 Unfortunately, few studies have shown the application of VAC as an antibiotic lavage aid in sNCNSIs.
The basis of this treatment is thorough debridement to remove intra-cranial infection and necrotic tissue, and primary suturing to maintain skin tension, barrier function, and enclosed internal environment. In previous studies, the probability of infection caused by retaining implants after incomplete debridement was 32% to 86%. 23 In this study, artificial implants such as prosthetic dura matter and titanium mesh were completely removed.
The brain should be isolated from VAC equipment. Repair of dura and watertight suture of the scalp assist with proper negative suction pressure and can prevent CSF suction from the wound. It is essential to monitor the occurrence of fluid extraction in VAC drainage tube closely. Once there is liquid suction, it is essential to remove the VAC device and determine the scalp seepage location. The leakage area of incision should be tightly sutured before replacing the VAC equipment. Previous studies have shown improper drainage of CSF would cause severe neurologic deficits and have shown reliable methods of treatment in complex craniotomy wounds.10,24,25
For the VAC group, slow rinsing with antibiotic solution can remove residual micro-organisms and inflammatory mediators from the operative cavity, helping to achieve effective antibiotic concentration in surgical cavity and avoiding insufficient local drug concentration caused by blood–brain barrier. Another important thing is to guarantee that the heads of drainage tubes extend to the deepest region of the surgical cavity in opposite directions, facilitating thorough flushing. Lactated Ringer's solution, which is more similar to the intra-cranial environment rather than normal saline, can be chosen as the lavage fluid. Meanwhile, the solution should also be properly heated before entering the surgical cavity, especially the ventricle, to avoid abnormal conditions such as spasm caused by excessive temperature difference.
In this study, 17 patients in the VAC group were clinically cured, with a cure rate of 94.4%. Only six cases in the control group were cured. Meanwhile, the cure rate of MDR bacteria was higher in the VAC group. The observed differences between the two groups suggest that the effectiveness of the VAC group is superior to that of the traditional treatment group. The results also provide a reasonable reference for future treatment of MDR bacterial infection.
After excluding the patients who died and were automatically discharged, the treatment times range of the control group is shorter than that of the VAC group. The cure rate is higher in the VAC group. This could also be seen in patients with MDR. There were more patients not cured in the control group and their treatment time was shorter, whereas similar patients in the VAC group were cured after longer treatment. This explains the shorter treatment times frame for the control group. Because of these reasons and limitation of the sample size, median treatment times was not specifically compared. The cause of death was aggravated intra-cranial infection associated with sNCNSIs. The aggravated intra-cranial infection would cause diffuse brain swelling or intra-cerebral hematoma. The main problem for these patients is intra-cranial infection. The outcomes demonstrated the effectiveness of the VAC therapy.
The follow-up results show the complications that emerged in the two groups. One study showed that complications caused by acute bacterial meningitis included seizures (17%), ischemic stroke (14%–25%), hydrocephalus (3%–5%), subdural empyma (3%), and brain abscess (5%). 26 The incidence of complications in our study is different, and the reason for the difference might be the infections in our study are more serious.
The recovery outcomes showed a difference between the two groups, even though the initial GCS score did not show substantial difference. This indicates that patients in the VAC group could have better prognosis. Meanwhile, a higher percentage of patients survived and underwent cranioplasty in the VAC group, allowing them to return to society and bringing great benefits to their families.
Former studies of VAC application in neurosurgery were limited to case reports. This study certainly has some limitations. The retrospective nature of this study finds the data dependent on medical records, and has the possibility of selection bias. This study is not a multicenter study, and small cohort size limits the statistical power. In addition, this study did not involve complex scalp reconstruction. However, this study has its own advantages. Our patient population was sampled from a major academic tertiary medical center in our province where the treatment course may differ from resource-limited sites. Further studies with more patients will further clarify characteristics and prognostic factors for sNCNSIs.
Conclusions
This study shows that the treatment of VAC-assisted antibiotic irrigation is safe and effective for patients with sNCNSIs, and the prognosis is ideal compared with traditional therapy. Our study demonstrates a new therapeutic strategy for this type of critical disease. In future research, it will be essential to expand to more patients and multicenter research, combine risk factors and rehabilitation, and standardize the technology, which will provide better clinical treatment and rehabilitation for patients with sNCNSIs.
Footnotes
Authors' Contributions
Data curation (lead): H. Wang. Formal analysis (lead): H. Wang, Sun. Investigation (lead): H. Wang. Methodology (equal): H. Wang, Huang, Zhang.
Resources (equal): H. Wang, G. Wang, Zhang. Writing—original draft (lead): H. Wang. Writing—review and editing (equal): H. Wang, Huang, Zhang.
Conceptualization (equal): Huang, Zhang. Project administration (lead): Huang. Supervision (equal): Zhang.
Funding Information
This study was supported by National Natural Science Foundation of China (grant no. 82171362) and Natural Science Foundation of Shandong Province (grant no. ZR2021MH366).
Author Disclosure Statement
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.