
Abstract
Background:
Because of the established path of bacterial entry and contamination-associated mechanisms, grade 3 open orthopedic fractures represent a substantial infection risk. The Eastern Association for the Surgery of Trauma (EAST) guidelines recommended covering Staphylococcus aureus and adding aminoglycoside gram-negative coverage. Local institutional guidelines rely on ceftriaxone for gram negative coverage and add methicillin-resistant Staphylococcus aureus coverage with vancomycin.
Patients and Methods:
The electronic health records of adults admitted for a grade 3 open fracture between January 1, 2016, and October 31, 2021, were retrospectively reviewed. Patients who received cefazolin and gentamicin (CZ+GM) or ceftriaxone and vancomycin (CRO+VA) as prophylaxis were included. We recorded the rate of a composite treatment failure outcome of receipt of antibiotic agents, infection-related hospitalization, or subsequent debridement for injury-site skin and soft tissue infection or osteomyelitis. The presence of acute kidney injury (AKI) was also evaluated.
Results:
There were 65 patients included in the CZ+GM group and 53 patients in the CRO+VA group. Patients in the CZ+GM group were younger (mean 42.6 compared with 50.6 years; p = 0.02). Otherwise, there were no significant differences between groups' demographics, mechanism and site of injury, timeline of care, or surgical interventions. More patients in the CZ+GM arm met the composite treatment failure outcome, but it was not statistically significant (45% vs. 32%; p = 0.2). There were similar rates of treatment failure at 30 days (21% vs. 26%; p = 0.5) and for only osteomyelitis (8% vs. 9%; p = 1).
Conclusions:
The trend in numerically lower treatment failure rates in the CRO+VA group across outcomes provides sufficient evidence to continue the current local recommendations. Given our sample size, type 2 error may have occurred, and studies with greater power should analyze this question.
Open fractures are graded by severity using the Gustilo-Anderson system, where grade 3 represents the most significant degree of injury to tissue and bone with a correspondingly higher risk of infection including osteomyelitis. 1 A number of modifiable risk factors have been evaluated including use of any antibiotic prophylaxis versus no prophylaxis, 2 time to first antibiotic agents, duration of antibiotic agents,2,3 time to first incision and debridement,4,5 and time to wound closure. 6 Although it is well described that antimicrobial prophylaxis is recommended, best practice regarding agent selection, and namely spectrum of prophylactic coverage, remains controversial. 3
The Eastern Association for the Surgery of Trauma (EAST) guidelines recommend covering Staphylococcus aureus for Gustilo-Anderson grades 1 and 2 open fractures, and adding gram-negative coverage with an aminoglycoside for grade 3 open fractures. 1 These guidelines were updated in 2011 to include cephalosporins alongside aminoglycosides for gram-negative coverage. 7 These regimens do cover the common causative pathogens anticipated in open fractures, such as Staphylococcus aureus and Streptococcus species, with the addition of gram-negatives such as Escherichia coli in grade 3 open fractures. 8
Recent studies have questioned the need for any gram-negative coverage. A large, propensity score-matched, retrospective cohort study by Suzuki et al. 9 in 2023 found no difference between narrow-spectrum (gram-positive only) versus broad-spectrum (gram-positive and gram-negative) prophylactic regimens in preventing surgical site infections related to open long bone fractures. However, this study was conducted among registry data from Japan and neither group commonly had methicillin-resistant Staphylococcus aureus-active agents in the regimens. Similarly, the 2022 Surgical Infection Society Guidelines for Antibiotic Use in Open Extremity Fractures suggest that routine methicillin-resistant Staphylococcus aureus (MRSA) coverage may not be necessary, although it may be reasonable if patients are at a high risk or are known carriers. 10
Overall, concerns exist if the EAST guideline recommendations remain the most relevant, given the potential toxicities related to aminoglycoside administration compared with counterparts conferring gram-negative coverage. Similarly, although data are promising for potentially narrowing regimens even for grade 3 fractures, MRSA remains a prominent threat in the United States according to the U.S. Centers for Disease Control and Prevention and locally at our institution. 11
To these points, our local institutional guidelines for grade 3 open fractures were updated in June 2019 to ceftriaxone and vancomycin, rather than cefazolin and aminoglycosides recommended in the EAST guidelines to best match our landscape of suspected causal pathogens.
Patients and Methods
Objectives
The primary objective of our study was to compare the rate of treatment failure up to one year post-injury for patients who received ceftriaxone and vancomycin (CRO+VA) versus cefazolin and gentamicin (CZ+GA) as their prophylaxis regimen. Treatment failure was defined as fulfilling at least one of the following conditions intended to treat either surgical site skin and soft tissue infection (SSTI) or osteomyelitis: receipt of antibiotic treatment, infection-related hospitalization, or need for surgical debridement within one year. For patients who met the receipt of antibiotic treatment criteria for SSTI or osteomyelitis, prescription fill data were validated against orthopedic clinic notes or inpatient progress notes to avoid treatment for unrelated sources of infection being credited as therapy failure. The same composite treatment failure criteria were applied at 30 days from injury as a secondary outcome. Another secondary outcome was incidence of osteomyelitis within one year. Cases of osteomyelitis were confirmed by health record documentation.
Additionally, safety was assessed using a composite any one of three Kidney Disease: Improving Global Outcomes (KDIGO) guideline criteria for acute kidney injury (AKI) within seven days of starting antibiotic prophylaxis: increase in serum creatinine of ≥0.3 mg/dL within 48 hours, increase in serum creatinine of ≥1.5 times baseline, or urine output volume <0.5 mL/kg per hour for at least six hours. 12
Study design
The present study was a retrospective electronic health record review conducted at a level 1 trauma center. This study was evaluated and approved by the network research institute's Institutional Review Board and determined to be exempt from annual review. The authors did not receive any funding for the performance of this research.
Participants
Patients were identified using the local trauma registry as well as International Classification of Diseases (ICD)-10 codes for open fracture. Adult patients admitted for a grade 3 open fracture between January 1, 2016, and October 31, 2021, were eligible for inclusion. Only patients who received CZ+GA or CRO+VA as their prophylaxis were included. Patients who suffered Gustilo-Anderson grades 1 or 2 fractures, fractures involving the skull or mandible, or traumatic digit amputation injuries were excluded. To account for potential one-time emergency department doses prior to final wound grading, patients were permitted to receive up to 24 hours of CZ to be included in the CRO+VA group or up to 24 hours of penicillin G to be included in the CZ+GA group. Patients were also excluded if they were managed at an outside facility for 24 hours or longer, or those who expired within seven days of their injury.
Patients who suffered multiple open fractures were included as multiple cases only if fractures occurred on at least two separate extremities. Time to first antibiotic agent was calculated as the difference between first antibiotic dose administered in medication administration record, regardless of which agent was administered first in the respective protocol regimens, and time charted for presentation to the emergency department. If patients in the CRO+VA group received a dose of CZ prior to a protocol antibiotic, this did not count toward the time to analysis. All cases were reviewed by resident orthopedic physicians, and definitions for wound debridement, revision, and closure were determined at their clinical discretion, based on information available in the electronic health record. To account for potential confounding causes of AKI, concomitant nephrotoxic medications were also recorded: angiotensin II inhibitor or angiotensin receptor antagonist, acyclovir, amphotericin B, calcineurin inhibitor, intravenous contrast, intravenous immunoglobulin, loop diuretic, non-steroidal anti-inflammatory, sulfonamide, or vasopressors. 13 All VA was dosed according to an institutional, pharmacist-driven protocol utilizing two-level area-under-the-curve calculations.
Statistical methods
Categorical variables were compared using the χ 2 test or Fisher exact test as appropriate. Continuous variables were compared by t-test for normally distributed data or Wilcoxon rank sum for non-normally distributed data. Descriptive statistics were used to record causative pathogens in cases of SSTI or osteomyelitis. A p value <0.05 was considered statistically significant. Finally, a multivariable logistic regression was performed for the primary composite outcome using a backwards-selection method. All statistical analysis was performed using R, version 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 517 patients were identified and screened for inclusion in the study. Three hundred ninety-nine patients were excluded, most frequently because of receipt of a non-protocol antibiotic regimen (219), skull or mandible involvement (85), age >89 or <18 (16), death within 7 days (15), and grade 1 or 2 fracture (15). In total 53 patients were included in the CRO+VA group and 65 patients were included in the CZ+GA.
Baseline characteristics were similar between the two groups, as displayed in Table 1. Patients in the CZ+GA group were younger, with a mean age of 42.6 years compared to 50.6 years in the CRO+VA group (p = 0.02). Otherwise, the patient demographics, characteristics of their injuries, or factors of their open fracture management outside the antibiotic regimen were not statistically different between the groups. Notably, the mean time to first antibiotic dose was under 1.5 hours for both groups, and the mean time to first debridement was within 10 hours for both groups.
Baseline Characteristics
ATV = all-terrain vehicle.
Expressed as mean ± standard deviation.
Expressed as count (percent).
Expressed as median (interquartile range).
The median duration of antibiotic receipt was two days for CZ, VA, and CRO, as displayed in Figure 1. Cefazolin showed the widest range of duration, up to 19 days of therapy. Most patients received a single dose of GA at a dose of 5 mg/kg. Although it was permissible in the protocol for up to 24 hours in the CZ+GA, no patients received penicillin. There were some CRO+VA patients who received one dose of CZ in the emergency department.
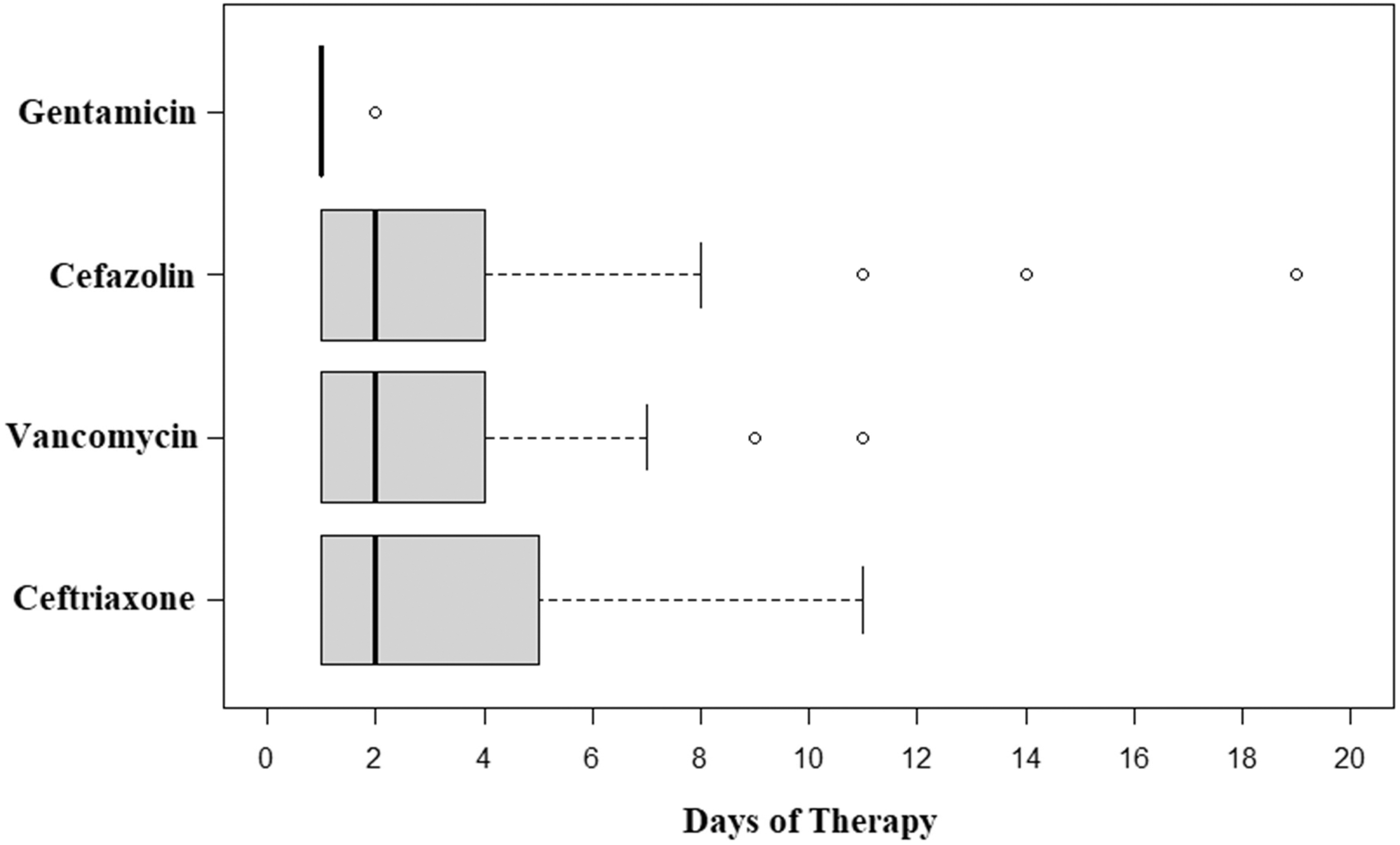
Therapy duration by antibiotic agent.
A numerically higher rate of the primary composite treatment failure outcome was observed in the CZ+GA group compared with the CRO+VA group, but it was not statistically significant (45% vs. 32%; p = 0.2; Table 2). The rate of meeting each respective criterion for the primary composite were also similar across the two groups, with antibiotic receipt being the most common. There were similar rates of treatment failure at 30 days (21% vs. 26%; p = 0.5) and when only cases of osteomyelitis were examined at one year (8% vs. 9%; p = 1). In a multivariable logistic regression for the primary composite outcome, shown in Figure 2, the only factor that significantly predicted treatment success was time to first antibiotic agents (odds ratio [OR], 0.51; 95% confidence interval [CI], 0.22–0.94). Significant predictors of treatment failure were number of debridement procedures (OR, 1.65; 95% CI, 1.13–2.52) and number of revision procedures (OR, 2.95; 95% CI, 1.4–6.99). Selection of antibiotic prophylaxis regimen was not a significant predictor in the model.

Multivariable logistic regression for primary treatment failure composite.
Primary and Secondary Outcomes
Categories are not mutually exclusive.
Twenty-six percent of patients in the CZ+GA arm met AKI criteria within seven days of antibiotic agents, whereas this was observed in only 19% of patients in the CRO+VA group (p = 0.4). The median number of concomitant nephrotoxic medications per patient was two in both arms (p = 0.8). We found no cases in which antibiotic therapy was stopped earlier than planned because of AKI.
The most common organism identified via culture in cases of therapeutic failure was Staphylococcus aureus (n = 10), with 60% (6/10) being MRSA. Excluding culture-negative cases, there was no significant difference in the rate of gram-positive infections in the CRO+VA group versus the CZ+GA group (16% vs. 14%; p = 0.8). Similarly, the rate of gram-negative infections was comparable between groups (12% vs. 10%; p = 1). Other pathogen data can be found in Table 3.
Treatment Failure Causative Pathogens a
SSTI = skin and soft tissue infection; OM = osteomyelitis; MRSA = methicillin-resistant Staphylococcus aureus; MSSA = methicillin-susceptible Staphylococcus aureus.
Counts represent each time an organism was cultured, not necessarily each patient case, to include polymicrobial infection data.
Discussion
The purpose of our study was to evaluate efficacy and safety outcomes for CRO+VA compared with CZ+GA as prophylaxis against downstream infectious complications of grade 3 open orthopedic fractures. CRO+VA was hypothesized to perform as well as CZ+GA at preventing infections with an anticipated improved safety profile. We observed a trend of numerically less frequent treatment failure and rate of AKI with the use of CRO+VA; however, this was not statistically significant. This study provided insufficient evidence to deviate from the current institutional recommendation of CRO+VA, because no clinical efficacy difference was observed, this regimen corresponds to common pathogens observed, and the true safety difference between regimens was likely underappreciated in the study given the limited exposure to gentamicin. Larger studies are needed to determine if this regimen is superior to the previous practice of using CZ+GA.
It was interesting to see the duration of therapy for gentamicin to be essentially one day, despite time to closure being longer than this. We hypothesize that providers are unwilling to continue to use gentamicin because of concern for toxicity, whereas providers seemed more amenable to continuing CRO and VA until wound closure. We also observed the longest duration of therapy among CZ recipients, with outliers of 11, 14, and 19 total days of therapy. Of note, CZ is not routinely under antimicrobial stewardship program review at our institution, whereas CRO and VA are targeted daily for optimization, including duration. This fact, combined with the similarity of number of debridement and revision procedures between the two groups, leads the authors to conclude that the longer CZ durations do not necessarily reflect more critically ill or surgically complex patients.
Additionally, we observed that time to first dose of antibiotic agent was approximately twice as long in the CRO+VA group as compared with the CZ+GA group, whereas the CRO+VA group's mean time to start breached the goal 66 minutes observed by Lack et al., 14 although this difference did not meet significance. We hypothesize this may be caused by the time necessary for formal fracture staging and/or orthopedic surgeon availability for bedside evaluation in the emergency department succeeding administration of empiric CZ doses.
One noteworthy strength of the study was the similarity between groups in both demographics and aspects of their open fracture care aside from their antibiotic regimen. We observed a similar rate of the primary composite outcome as was observed in external literature, noting that this study included only grade 3 open fractures with the highest risk of infectious complications.2,3
Finally, we reported causal microbes in cases of surgical site SSTI to guide potential future regimens. Similar to other studies, Staphylococcus aureus, and particularly MRSA, was the most frequent organism identified. Interestingly, it was commonly found in early (30-day) infections in patients who received VA prophylaxis, which may serve as a future research question when a larger sample is available. Similarly, Enterobacter cloacae was observed in four cases, three of which were in the CZ+GA group. This suggests that prophylaxis with an ampC β-lactamase–resilient agent, such as gentamicin, may not be necessary to prevent Enterobacter infections.
The study was limited by its retrospective nature. This can be noticed in the provider-specific, wide variation in treatment durations. Additionally, the possibility cannot be excluded that patients were lost to follow-up or to outside institution care at one year, which could falsely decrease the study's treatment failure rate. Similarly, incomplete charting of urine output and unclear true baseline serum creatinine values may have falsely decreased the rate of acute kidney injury observed in both groups. Although we attempted to capture confounding causes of AKI in recording concomitant nephrotoxic medications, we acknowledge that patients with traumatic injuries are subject to other precipitating factors of AKI such as hypovolemia and adverse effects of operative anesthesia that are not represented in the present retrospective study. Although we had trends in improved outcomes with CRO+VA, the study was ultimately underpowered, so it cannot be excluded that a type 2 error occurred and a difference in outcomes exists between the regimens studied. Last, this study did not comment on the use of antibiotic bead pouch installation, antibiotic-impregnated cement, or use of vacuum devices for wound closure as it pertains to infectious outcomes.
Conclusions
In conclusion, there is sufficient evidence to maintain CRO+VA as the first-line local recommendation for grade 3 open fractures. The rate of infectious complications was comparable between patients who received CZ+GA and those who received CRO+VA, although type 2 error may have occurred. The difference in safety by using CRO+VA was likely underappreciated in this study, because of the retrospective nature and short durations observed of GA.
Footnotes
Acknowledgments
Authors' Contributions
Literature search: Shifko, Jenniches, Bremmer. Study design: Shifko, Jenniches, Holmberg, Andreini, Bremmer. Data collection: Shifko, Holmberg, Andreini. Data analysis: Shifko, Bremmer. Data interpretation: Shifko, Jenniches, Philp, Altman, Bremmer. Writing: Shifko, Jenniches, Bremmer.
Critical revision: Shifko, Jenniches, Holmberg, Andreini, Philp, Altman, Bremmer. All authors reviewed the final manuscript.
Funding Information
The authors of this manuscript have received no funding for the performance of this study.
Author Disclosure Statement
The authors of this manuscript have no conflicts of interest.