
Abstract
Background:
In most cases of pulmonary or pleural post-coronavirus disease 2019 (COVID-19) complications, surgical interventions are performed to treat these complications, but the method of the surgery and its outcome in these patients is not clearly defined. We present 40 patients with pulmonary and pleural complications after COVID-19 who required surgical intervention.
Patients and Methods:
In this case series, patients' data were prospectively collected from April to August 2022 at Masih Daneshvari Hospital. Inclusion criteria were patients with COVID-19 who were referred to the thoracic surgery department because of pleural effusion, pneumothorax, empyema, infected or non-infected pneumatocele, and lung cavity with suspected fungal infections. The required intervention for each patient was assessed.
Results:
Patients' mean age was 49.21 ± 11.5 (30–69 years). Nine patients (22.5%) were female. Pure pleural effusion was reported in five (12.5 %), pneumothorax in eight (20%), empyema in 29 (72.5%), and infected pneumatocele in two patients (5%). Twelve patients had bronchial fistulas that were clarified at the time of surgery that needed repair after resection. In 13 patients (32.5%) because of pleural effusion or pneumothorax, a chest tube was inserted and after two weeks lungs were fully expanded. All patients with pneumothorax were managed by chest tube initially but in the presence of continuous air leakage and non-expanding lungs surgical thoracotomy or video-assisted thoracoscopic surgery (VATS) were considered for correction. In 10 patients who required thoracotomy, the chest tube was necessary for more than one month. In most of the patients, there were small cystic lesions or peripheral bronchopleural fistula. In 17 (42.5%) cases of empyema, necrotic pneumonia was documented and eight patients (20%) had aspergillus infection in the pathology report and two patients had a pulmonary abscess.
Conclusions:
Pleural COVID-19 complications can be treated with conventional surgical methods such as chest tube insertion, and debridement of infected tissue with no mortality and further complications.
After the outbreak of the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic, a substantial number of complications requiring pleural and pulmonary surgery have been reported in coronavirus disease 2019 (COVID-19)-infected patients. 1 Since December 2019, acute and severe respiratory infection with COVID-19 has spread all over the world and led to a wide range spectrum of clinical manifestations from asymptomatic to severe and acute respiratory failure.2,3 Risk factors for severe involvement and exacerbation of symptoms in COVID-19 include old age, cardiovascular disease, diabetes mellitus, hypertension, chronic respiratory diseases, obesity, malignancies, immune system disorders, poor living conditions, male gender, high virus load, and disturbed laborartory data findings. In addition, treatment of patients with COVID-19 was challenging. 4 In some cases, patient's symptoms improved without any side effects, and in some cases, they experienced numerous complications. 5
Some of the complications of COVID-19 include rhabdomyolysis, stroke, Kawasaki-like syndrome, Guillain-Barre syndrome, and secondary infection.6–10 Microvascular injuries and thrombotic events after COVID-19 infection are mainly due to the activation of multiple complement pathways, which is the cause of some of these complications. 11 However, numerous uncommon pulmonary and pleural complications have been reported after COVID-19 pneumonia, including para-pneumonic effusion (uncomplicated, complicated, or empyema), pneumomediastinum, pneumothorax, cystic lesion (pneumatocele) and lung cavities due to parenchymal damage and secondary infections such as fungi.12–15 In most cases surgical interventions are performed to treat these complications, but the method of the surgery and its outcome in these patients are not clearly defined. 16 In this study, we present 40 patients with pulmonary and pleural complication after COVID-19 infection who have undergone surgical intervention.
Patients and Methods
Subjects
In this case series study, we used the CARE reporting guidelines (Supplementary Table S1. 17 Patient data were gathered prospectively from April to August 2022. Inclusion criteria were all patients with COVID-19 who were referred to the thoracic surgery department of Masih Daneshvari hospital because of pleural effusion, pneumothorax, empyema, pneumatocele, and lung cavity. The study protocol was registered and approved by the ethics committee, and all the participants provided written informed consent.
Data gathering
Demographic data, past medical and drug history, and history of COVID-19 disease (the therapeutic approach and outcomes) were gathered. Patient's hospitalization in a COVID-19 ward included the severity of the involvement, history of vaccination, performed treatment, duration of hospitalization, and complications were collected. In addition, information about hospitalization in the surgical ward, including the patient's chief complaint, final diagnosis, type of therapeutic intervention, pathology of the lesion, duration of hospitalization and outcome of the treatment were evaluated.
Data analysis
The primary outcome of this study was to evaluate indications for surgery in post COVID-19 pleural complications, and the early outcomes of these procedures. SPSS software (IBM Corp, Armonk, NY) was used to collect and analyze the obtained information. Quantitative information was reported as mean and standard deviation and qualitative information as percentage. To compare categorical variables, a χ 2 and for quantitative data Student t-test were used. Also, p < 0.05 were considered statistically significant.
Results
The results of 40 patients with signs and symptoms of pleural and pulmonary involvement after COVID-19 that led to invasive intervention were presented. The mean age of the patients was 49.21 ± 11.5 years (30–69 years). In total, 31 (77.5%) of the patients were male. In 40% of cases, the patients have no past medical history of diabetes mellitus, hypertension, or immunosuppression. Table 1 shows the different medical history among the patients.
Patient's Characteristics and Past Medical History
BMI = body mass index.
In some cases more than one comorbidity were reported.
Clinical manifestation(s)
The mean time between the current complication and the diagnosis of COVID-19 was 39.8 days (7–150 days). Clinical manifestations included shortness of breath in 32 patients (80%), pleuritic chest pain in 26 patients (65%) and flank pain in four patients (10%). In one patient, the pulmonary findings were incidental, and the patient was asymptomatic.
Chest radiography and computed tomography (CT) scan assessments are summarized in Figures 1, 2 and 3. Pleural effusion was reported in five patients (12.5%), pneumothorax in eight patients (20%), empyema in 29 patients (72.5%), lung abscess in two patients (5%), and aspergilloma in eight patients (20%). Indeed, in some patients, there was more than one complication. In addition, 12 patients had bronchial fistulas that were established during surgery and required reconstruction after resection.
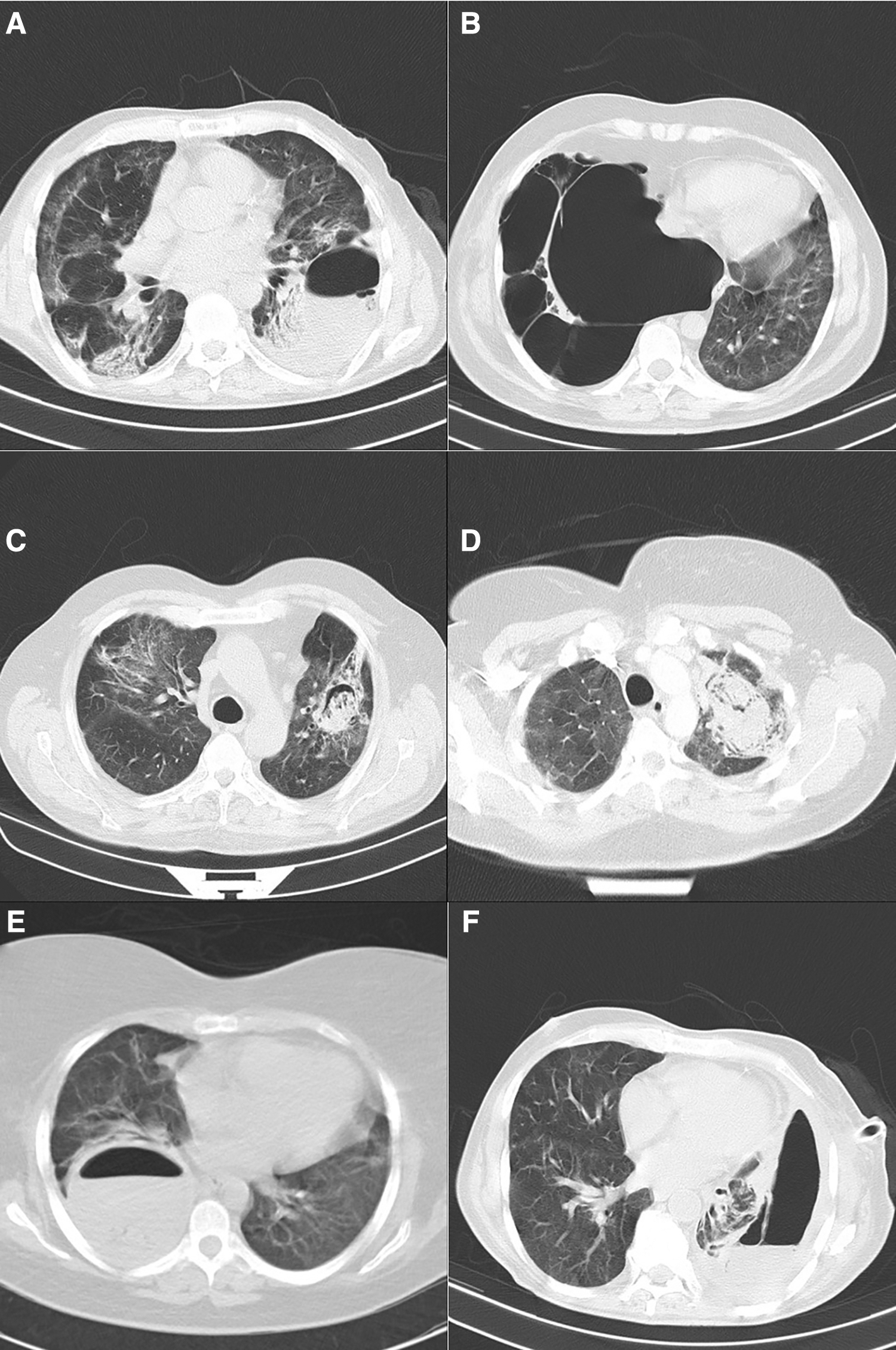
Computed tomography findings in patients with pleural complications:
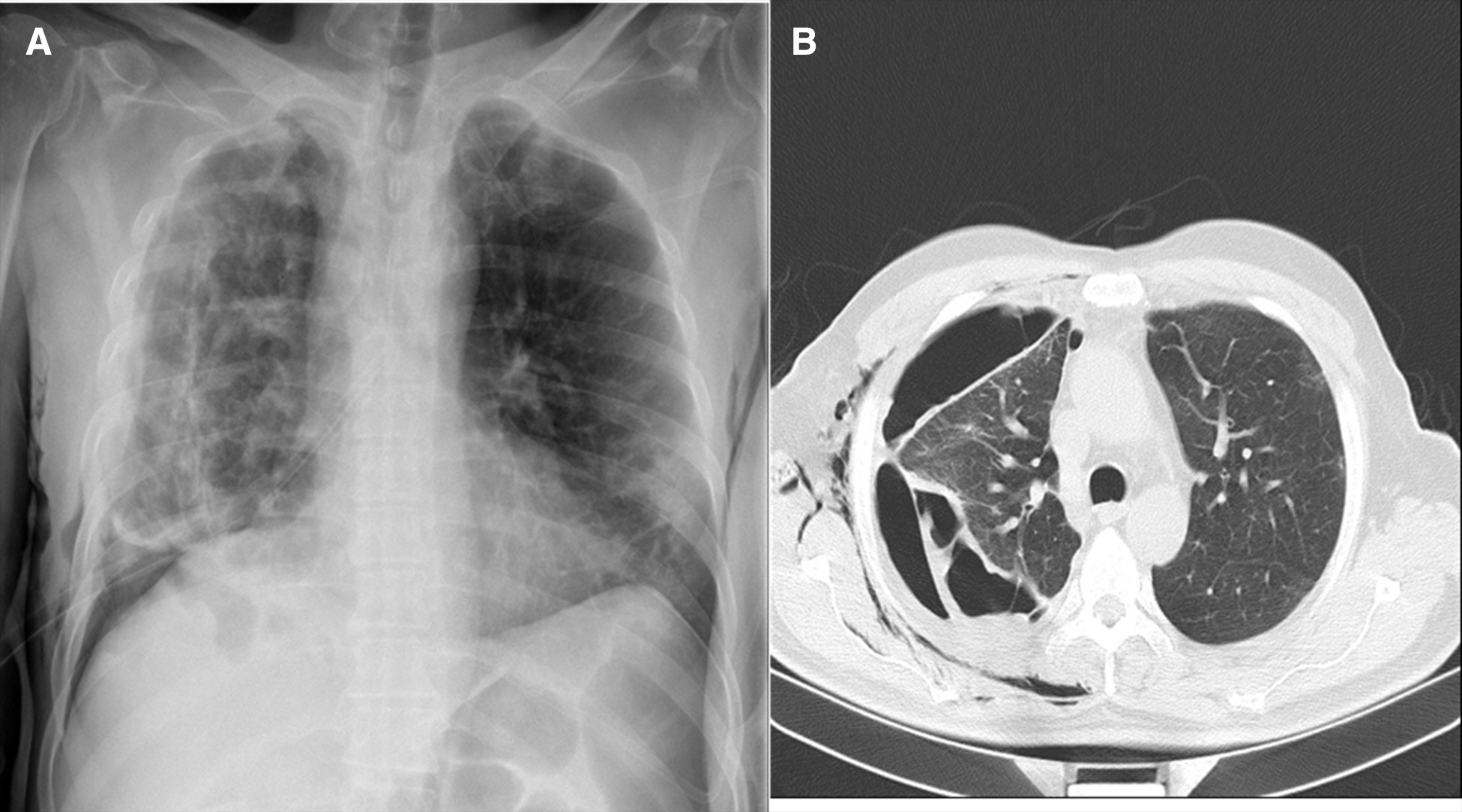
Chest radiograph
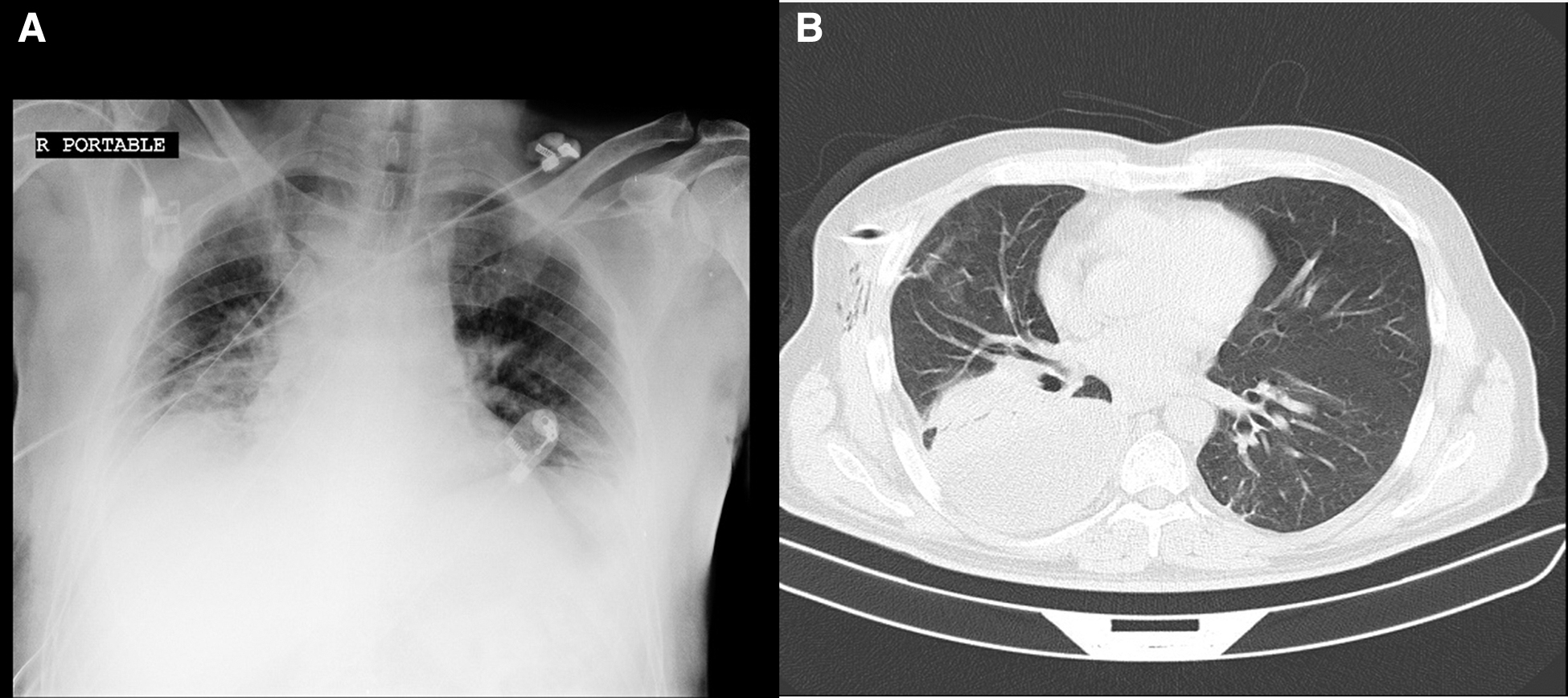
Chest radiogram
Necrotizing pneumonia was reported in 17 of 29 (42.5%) cases of empyema and eight patients (20%) had aspergillosis infection in the pathology report. At the same time, these patients also had bronchial fistula. Some of our patients had more than one lesions including empyema and aspergilloma.
Therapeutic approaches
The mean duration of hospitalization was 12 ± 8 days. In 13 patients (32.5%), a chest tube was inserted after diagnosis and pneumothorax or non-emphysematous pleural effusion, and according to minimal parenchymal damage lungs fully expanded after two weeks, these patients were discharged from the hospital without any complications.
Considering that thoracic surgical complications of COVID-19 were different in each patient surgical management was not the same in any individuals. For all patients with empyema at the beginning of treatment a chest tube was inserted and according to thick pleural peel decortication was done through thoracotomy or video-assisted thoracoscopic surgery (VATS). In this group of patients, pleural peel was removed when the lung was trapped with or without debridement of necrotic tissue and fungal pulmonary lesions. In most patients who had undergone decortication, there were some necrotic lung tissues in combination with small peripheral cystic lesions so debridement was done by non-anatomic wedge resection. All patients with pneumothorax were managed by chest tube initially but in the presence of continuous air leakage and non-expanding lungs surgical thoracotomy or VATS considered for correction. In most of these patients, there were small cystic lesions or peripheral bronchopleural fistula.
Peripheral cystic lesions were also managed in the same manner. In all patients with fungal lesion with small size and peripheral location a wedge resection was done. There was no need for anatomic resection of lung (segmentectomy or lobectomy) in any of the patients. In patients with lung abscess, if that lesion was small and peripherally located, drainage and wedge resection was considered with maximum resection. In addition, in all patients with bronchopleural fistula in the presence of pathologic lesions, minimal resection with staples had satisfactory results for closure at the time of surgery.
In 10 patients after thoracotomy, the chest tube was necessary for more than one month because in the first week after surgery, the symptoms of recovery such as no air leakage and pulmonary expansion were not observed; conclusively, these patients managed by a Heimlich valve (in cases with prolonged air leakage) or empyema tube (in cases with not fully expanded lungs). Then, chest tubes removed one month after surgery.
Thirty-nine patients recovered after the treatments; one patient died because of a heart complication unrelated to the surgical complications. None of the patients had bleeding, and there was no need for multiple surgeries in any patient.
Discussion
In this study, the pulmonary and pleural complications caused by COVID-19 infection have been evaluated and analyzed. Coronavirus disease 2019 has a wide spectrum of clinical manifestations, so our knowledge of the management of COVID-19 is constantly developing. Physicians should be aware of the common and rare manifestations of COVID-19. Pleural and lung involvement that require surgical intervention have been reported in COVID-19–infected patients. Pleuritic chest pain or shortness of breath should be included in the differential diagnosis as a post-COVID-19 complication and necessary treatment should be performed.
Forty patients were assessed in this prospective study, which to the best of our knowledge is the largest case series study of patients who developed pulmonary and pleural complications with surgical approaches after COVID-19 infection. In approximately one-half of the cases, the patients did not have any past medical history, which is considered as a risk factor for the development of these complications. Most patients were male and were younger compared with non-COVID-19 empyema.
In this study, 20% of the patients had pleural effusion. This complication is not common among patients with COVID-19, and a recent study showed that pleural effusion occurred in 10.3% of patients with COVID-19, and the prevalence of pleural effusion were more in treatment-resistant patients than normal COVID-19 patients, which indicates a more obvious inflammatory response in the lung 18 after COVID-19 was 7.6% (18% among severe lung involvement and 1.3% in moderate lung involvement).
The prevalence of pleural effusion has an association with the patient's age, so that patients over 50 years are more likely to develop pleural effusion. It is worth noting that the results of this study are in line with other studies that have reported the prevalence of 3.7% of pleural effusion in systematic review studies. 19
Tsang et al., 20 in a study of 63 patients with para-pneumonic effusion reported that 26% of the isolated micro-organisms were streptococci, 14% Bacteroides, and 12 Klebsiella pneumoniae. In addition, they showed that pneumonia caused by COVID-19 is accompanied with neutrophil-dominant effusion and increased pleural lactate dehydrogenase (LDH) to serum LDH ratio.
Zhange et al. 21 assessed 34 patients with COVID-19 with an age range of seven to 88 years and reported the occurrence of pleural effusion in only one case, and in general, the studies showed that long hospital stay is associated with higher incidence of plural effusion.
Para-pneumonic complications such as empyema are different in patients who are infected with COVID-19 compared with those patients without COVID-19; need for wedge resection is one of these differences. In our center, pulmonary empyema usually does not require lung wedge resection or lung reconstruction with suture, but because of the creation of bronchial fistulas and destruction of the lung due to necrotizing pneumonia and aspergillus infection, eight patients needed lung reconstruction after resection. Indeed, para-pneumonic effusion may be sterile fluid in post-COVID-19 patients, but antibiotic therapy is recommended empirically. In this regard, by assessing three patients, Tessitore et al. 1 declared empyema due to COVID-19 as a life-threatening condition and claimed that chest tube insertion was insufficient. They recommended simultaneous medical and surgical treatment. In our center, all patients recovered without developing complications and surgery was required in all cases of empyema. Patients that were presented by Tessitore et al. 1 had fibrosing pleuritic, edema, and granulation tissue in pathology. Also, there was granulation tissue in 60% of the patients who underwent wedge resection.
The length of hospitalization after surgery of empyema in case of COVID-19 complications was longer than those with empyema and no history of COVID-19. Among the reported patients in this center, one case of mortality after cardiac arrest was documented and it was not associated with the surgical complication. In one of the case series studies, among 13 patients who had undergone surgery, one case of mortality was reported, which was due to hemothorax. 22
Complications of pleural and pulmonary surgery in patients with COVID-19 are a new range of problems that thoracic surgeons are involved in. How to approach these complications and appropriate surgical methods are not well known. In the present study, we showed that most patients can be treated with common surgical methods such as chest tube insertion, debridement of infected tissue, etc.
Most of the concern was related to patients who had developed fungal infections. Most of these fungi were Aspergillus, but the outcome of common surgical intervention on these patients was good and the patients recovered well. We did not have any cases of lung involvement with mucormycosis in this study. However, there are reports of lung involvement with mucormycosis in other studies, which should be further investigated for the appropriate method of treatment and its outcomes.
Footnotes
Authors' Contributions
Conceptualization (lead): Dezfili, K. Sheikhy, A. Sheikhy. Editing: Dezfili, K. Sheikhy, A. Sheikhy. Formal analysis (lead): Ghorbani. Writing—first draft: Dezfuli, Razaghi, Daneshman. Writing—review and editing: Ghorbani, Soleimani. Software: Soleimani. All authors attest that they meet the current ICMJE criteria for authorship.
Funding Information
This study was supported by National Research Institute of Tuberculosis and Lung Diseases.
Author Disclosure Statement
The authors have no financial disclosures. The study was approved by ethical committee of National Research Institute of Tuberculosis and Lung Diseases.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.