
Abstract
Background:
Infectious complications lead to worse post-operative outcomes and are used to compare hospital performance in pay-for-performance programs. However, the impact of social and behavioral determinants of health on infectious complication rates after emergency general surgery (EGS) remains unclear.
Patients and Methods:
All patients undergoing EGS in the 2019 Nationwide Readmissions Database were included. The primary outcome of the study was the rate of infectious complications within 30 days, defined as a composite outcome including all infectious complications occurring during the index hospitalization or 30-day re-admission. Secondary outcomes included specific infectious complication rates. Multivariable regression analyses were used to study the impact of patient characteristics, social determinants of health (insurance status, median household income in the patient's residential zip code), and behavioral determinants of health (substance use disorders, neuropsychiatric comorbidities) on post-operative infection rates.
Results:
Of 367,917 patients included in this study, 20.53% had infectious complications. Medicare (adjusted odds ratio [aOR], 1.3; 95% confidence interval [CI], 1.26–1.34; p < 0.001), Medicaid (aOR, 1.24; 95% CI,1.19–1.29; p < 0.001), lowest zip code income quartile (aOR, 1.17; 95% CI, 1.13–1.22; p < 0.001), opioid use disorder (aOR,1.18; 95% CI,1.10–1.29; p < 0.001), and neurodevelopmental disorders (aOR, 2.16; 95% CI, 1.90–2.45; p < 0.001) were identified as independent predictors of 30-day infectious complications. A similar association between determinants of health and infectious complications was also seen for pneumonia, urinary tract infection (UTI), methicillin-resistant Staphylococcus aureus (MRSA) sepsis, and catheter-association urinary tract infection (CAUTI).
Conclusions:
Social and behavioral determinants of health are associated with a higher risk of developing post-operative infectious complications in EGS. Accounting for these factors in pay-for-performance programs and public reporting could promote fairer comparisons of hospital performance.
Emergency general surgery (EGS) procedures comprise 7.1% of all inpatient admissions and are responsible for an increased rate of post-operative complications and death compared with elective procedures.1–4 In other words, patients undergoing EGS procedures are up to five times more likely to die, with more than 50% of survivors developing a post-operative complication. 4 On a national level, the financial strain posed by EGS is disproportionately high, with an estimated annual cost of $28.37 billion in the United States.1,5,6 In this framework, post-operative infectious complications are responsible for prolonged hospitalization, increased healthcare costs, and higher re-operation, re-admission, and mortality rates.7–9
Currently, post-operative infectious complications and hospital-acquired infections (HAI) rates are used as metrics to compare hospital performance and to reward or penalize institutions in pay-for-performance programs such as the Hospital-Acquired Condition Reduction Program (HACRP).10–14 The rationale is that HAI are potentially preventable in the hospital setting. However, the measures used in the HACRP program do not consider elements that may have an impact on post-operative infectious complication rates, such as sociodemographic factors, substance use disorders, or neuropsychiatric comorbidities. Furthermore, it has been shown in the literature that teaching hospitals and safety net hospitals serving the most vulnerable populations, such as those in federal poverty areas, may have been disproportionately penalized under the HACRP.15,16 Nationally, exposures such as low income, lack of health insurance, psychiatric disease, and substance use disorder often coexist.17–19
Although the associations between patient age, chronic comorbidities, surgical approach (i.e., laparoscopic vs. open), procedure complexity, and post-operative complications are well established in the literature, 20,21 the impact of social determinants of health, substance use disorder, and neuropsychiatric comorbidities on infectious complications remains unclear. In this study, we used a large administrative database to investigate whether social and behavioral determinants of health might be associated with an increased rate of infectious complications in patients undergoing EGS procedures.
Patients and Methods
Data source and study population
The Nationwide Readmissions Database (NRD) consists of a large administrative healthcare database designed to capture information on hospital readmissions in the United States. 22 We performed a retrospective analysis of the 2019 NRD to identify all adult patients who underwent a major abdominal surgical procedure, as defined by the American Association of Trauma (AAST) grading system, 23 during a non-elective admission. International Classification of Diseases (ICD)-10 Clinical Modification (CM), and Procedure Coding System (PCS) codes were used to abstract diagnoses and procedures of interest 24 (Supplementary Table S1 and Supplementary Table S2). To include all infectious complications occurring within 30 days from the index admission in the NRD annual dataset, we excluded all patients who were admitted during the last month of the year. Last, we excluded all patients who were transferred between hospitals and patients who were dead on arrival.
Clinical variables and hospital characteristics
Patient demographic characteristics, comorbidities, socioeconomic factors, and hospital-specific variables were identified within the included patient population (Table 1). Comorbidities were identified via ICD-10 CM codes and used to construct the Elixhauser comorbidity index. 25 All patient refined diagnostic related groups (APR-DRG) severity of illness, defined as the extent of organ system derangement or physiologic decompensation for a patient, was reported as indicated in the NRD database. Hospital bed size, hospital teaching status, and patient location according to the National Center for Health Statistics (NCHS) urban-rural classification were identified. The type of surgery, and the surgical approach (i.e., open vs. laparoscopic), were determined via ICD-10 PCS codes (Supplementary Table S2). In the NRD administrative dataset, surgical procedures are grouped into clinically meaningful categories using the ICD procedure mapping software provided with the database. However, the primary procedure for each patient is not indicated. As a result, surgical procedures are not mutually exclusive. For example, a patient undergoing a colectomy may also undergo a small bowel resection. All surgical procedures have been reported in Table 2.
Patient and Hospital Baseline Characteristics
Data are presented as median (IQR) for continuous measures, and n (%) for categorical measures.
IQR = interquartile range; NCHS = National Center for Health Statistics; DRG = diagnosis-related groups.
Surgical Procedures According to the Primary Outcome
Exposures
Insurance status and median household income were included as social determinants of health. Patient insurance status was categorized as Medicare, Medicaid, private insurance, self-pay, or other. The median household income quartile in the patient's residential zip code was reported according to the NRD data dictionary. Neuropsychiatric comorbidities were categorized using ICD-10 CM codes as schizophrenia, bipolar disorder, depression, and neurodevelopmental disorders. Substance use disorders were also identified via ICD-10 CM codes, and divided into opioid use disorder, cocaine use disorder, and other psychoactive substance use disorder (Supplementary Table S1).
Outcomes
The primary outcome was the 30-day infectious complication rate, defined as a composite outcome including all infectious complications that occurred during the index hospitalization or 30-day re-admission. In the primary outcome, the following infectious complications were included: pneumonia, urinary tract infection (UTI), surgical site infection (SSI), post-procedural sepsis or septic shock, catheter-associated urinary tract infection (CAUTI), central line-associate blood stream infection (CLABSI), Clostridioides difficile enterocolitis, and methicillin-resistant Staphylococcus aureus (MRSA) sepsis. Secondary outcomes included the rates of pneumonia, UTI, and infectious complications used as metrics for hospital performance in pay-for-performance programs such as the HACRP, including the rates of complex SSI, CAUTI, and MRSA sepsis. Complex SSI was defined as all deep and organ/space SSI occurring during the index admission or within 30 days after discharge.
Statistical analysis
Univariable analysis was performed to describe patient baseline and sociodemographic characteristics. Continuous variables were reported as median (interquartile range [IQR]) and a comparison was made using either a Wilcoxon rank-sum test or a Student t-test as appropriate. Frequencies (percent) were reported for categorical variables, and statistical analysis was conducted using Pearson χ 2 test or Fisher exact test. Multivariable regression analyses were used to study the impact of patient characteristics, social determinants of health (median annual income in the patient's residential zip code and insurance type), and behavioral determinants of health (substance use disorders, psychiatric illness, neurodevelopmental disorders) on the outcomes of interest.
To address potential confounding, the multivariable logistic regression model was adjusted for age (used as a continuous variable), gender, Elixhauser Comorbidity Index, severity of illness, laparoscopic or open surgical approach, hospital bed size, hospital teaching status, patient location (as defined by the NCHS urban-rural classification), insurance status, income quartile based on residential zip code, opioid use disorder, cocaine use disorder, other psychoactive substance use disorder, depression, bipolar disorder, schizophrenia, and neurodevelopmental disorders. All outcomes were modeled separately, and hospital clustering was taken into account. To evaluate if the results seen in our main analysis varied according to the surgery type, we performed a sensitivity analysis including only patients undergoing one of two common surgical procedures associated with different post-operative infection rates: colectomy and appendectomy. All analyses were conducted using STATA, version 17.0 (StataCorp, CollegeStation, TX).
Ethical oversight
This study was exempted from Institutional Review Board approval. Our methods and results have been reported in compliance with the STrengthening the Reporting of OBservational studies in Epidemiology and REporting of studies Conducted using Observational Routinely-collected Data (RECORD) statements (Supplementary Table 3). 26
Adjusted Odds Ratios of Developing Specific Infection Types According to Insurance Type, Income Quartile, Substance Use Disorder, and Neuropsychiatric Comorbidities
aOR in bold have been identified as independent predictors for the specific infection type. P values in bold are considered statistically significant.
aOR = adjusted odds ratio; CI = confidence interval; SSI = surgical site infection; CAUTI = catheter-associated urinary tract infection; MRSA = methicillin-resistant Staphylococcus aureus.
Results
Patient population characteristics
A total of 367,917 patients, of whom 75,522 (20.53%) developed an infectious complication at index admission or at 30-day re-admission, were included in the analysis (Table 1). The most performed surgeries were cholecystectomy (141,280; 38.4%), appendectomy (64,526; 17.5%), and colectomy (55,527; 15.1%). The surgeries with the highest infectious complication rates were colectomy (20,737; 27.5%), cholecystectomy (19,517; 25.8%), creation of bowel ostomy (17,162; 22.7%), adhesiolysis (15,523; 20.6%), and small bowel resection (13,094; 17.3%) (Table 2). The patients who developed post-operative infectious complications after EGS procedures were older (67 vs. 57 years; p < 0.001), had an increased Elixhauser Comorbidity Index (4 [IQR, 2–5] vs. 2 [IQR, 1–3]; p < 0.001), and a higher severity of illness (3 [IQR, 2–4] vs. 2 [IQR, 1–3]; p < 0.001) compared with patients who did not develop infectious complications. Patients who suffered infectious complications had a higher proportion of Medicare recipients (60.6% vs. 36.4%; p < 0.001), a lower proportion of Medicaid recipients (13.9% vs. 17.9%; p < 0.001) a lower proportion of privately insured patients (19.7% vs. 36.1%; p < 0.001), and a lower proportion of self-pay patients (2.9% vs. 5.7%; p < 0.001) compared with patients who did not develop infectious complications.
Furthermore, patients living in a zip code area with a lower median household income appeared to be more represented in the infectious complications cohort (first quartile, 28.6% vs. 26.3%, p < 0.001; second quartile, 25.9% vs. 25.4%; p < 0.001), whereas patients living in high-income zip code areas were less represented in the infectious complications cohort (third quartile, 24.9% vs. 25.8%; p < 0.001; fourth quartile, 19.2% vs. 21.2%; p < 0.001). In the univariable analysis, patients with infectious complications had higher rates of opioid use disorder (2.1% vs. 1.1%; p < 0.001), cocaine use disorder (0.5% vs. 0.3%; p < 0.001), and other psychoactive substance use disorder (1.1% vs. 0.8%; p < 0.001). Additionally, patients who developed infectious complications had a higher rate of neuropsychiatric comorbidities, such as schizophrenia (1.7% vs. 0.8%; p < 0.001), bipolar disorder (2.1% vs. 1.6%; p < 0.001), depression (1.3% vs. 0.7%; p < 0.001), and neurodevelopmental disorders (0.8% vs. 0.3%; p < 0.001).
Multivariable analysis: Independent predictors of 30-day infectious complications
After adjusting for patient age, comorbidities, severity of illness, and hospital characteristics, Medicare (adjusted odds ratio [aOR], 1.3; 95% confidence interval [CI], 1.26–1.34; p < 0.001), Medicaid (aOR,1.24; 95% CI,1.19–1.29; p < 0.001), opioid use disorder (aOR,1.18; 95% CI, 1.10–1.29; p < 0.001), other substance use disorder (aOR, 1.14; 95% CI, 1.02–1.26; p = 0.01), schizophrenia (aOR, 1.23; 95% CI, 1.13–1.34; p < 0.001) and neurodevelopmental disorders (aOR, 2.16; 95% CI, 1.90–2.45; p < 0.001) were associated with higher rates of 30-day infectious complications. The median household income of the patient's residential zip code appeared to be inversely proportional to the odds ratio of developing infectious complications after EGS procedures. Namely, residing in areas with the lowest household income was identified as an independent predictor of infectious complications (aOR, 1.17; 95% CI, 1.13–1.22; p < 0.001), followed by the second to lowest income quartile (aOR, 1.11; 95% CI, 1.07– 1.15; p < 0.001), and by the third income quartile (aOR, 1.07; 95% CI, 1.03–1.10; p < 0.001) compared with patients living in high-income areas (Fig. 1).
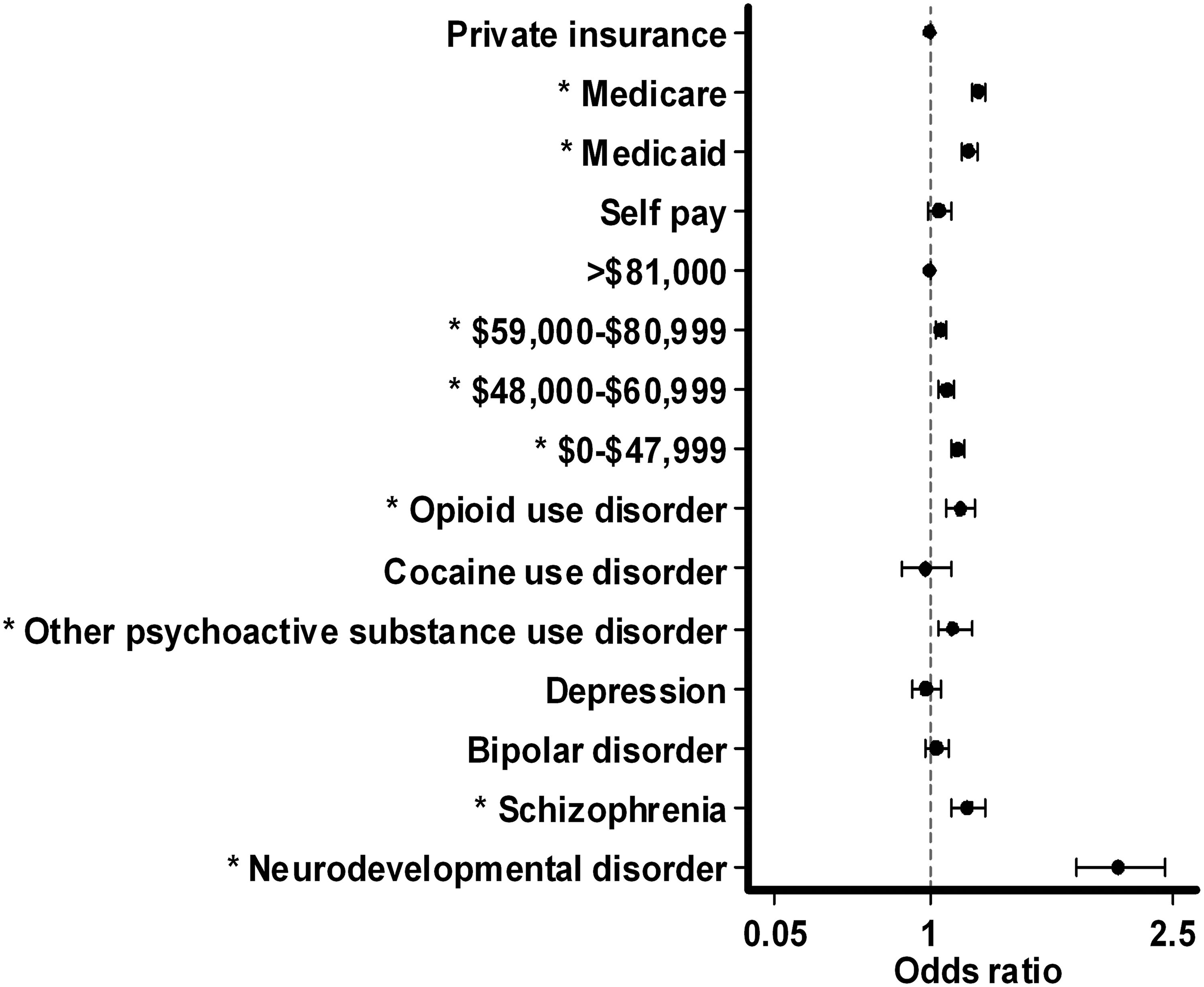
The adjusted risk of developing 30-day infectious complications after emergency general surgery (EGS) procedures according to social and behavioral determinants of health.
Multivariable analysis: Independent predictors of specific post-operative infections
Pneumonia
Medicare (aOR, 1.30; 95% CI, 1.24–1.36; p < 0.001), Medicaid (aOR, 1.28; 95% CI, 1.21–1.35; p < 0.001), opioid use disorder (aOR, 1.28; 95% CI, 1.16–1.40; p < 0.001), bipolar disorder (aOR, 1.17; 95% CI, 1.06–1.29; p = 0.002), schizophrenia (aOR, 1.36; 95% CI, 1.22–1.52; p < 0.001), and neurodevelopmental disorders (aOR, 2.77; 95% CI, 2.38–3.23; p < 0.001) were identified as independent predictors of developing pneumonia. Patients living in an area with the lowest (aOR, 1.24; 95% CI, 1.17–1.30; p < 0.001) and second to lowest median household income (aOR, 1.12; 95% CI, 1.06–1.18; p < 0.001) had an increased risk of developing pneumonia compared to patients living in high-income areas (Table 3).
Urinary tract infection
Medicare (aOR, 1.52; 95% CI, 1.45–1.59; p < 0.001), Medicaid (aOR, 1.51; 95% CI, 1.43–1.60; p < 0.001), self-pay (aOR, 1.36; 95% CI, 1.26–1.48; p < 0.001), other psychoactive substance use disorder (aOR, 1.35; 95% CI, 1.17–1.56; p < 0.001), schizophrenia (aOR, 1.33; 95% CI, 1.19–1.47; p < 0.001), and neurodevelopmental disorders (aOR, 2.12; 95% CI, 1.82–2.45; p < 0.001) were associated with an increased risk of developing a UTI. The median household income of the area where the patient resided was inversely proportional to the adjusted odds ratio of developing a UTI. Patients living in the lowest income area (aOR, 1.38; 95% CI, 1.31–1.47; p < 0.001), second to lowest income area (aOR, 1.23; 95% CI, 1.16–1.30; p < 0.001), and third quartile income area (aOR, 1.16; 95% CI, 1.10–1.22; p < 0.001) had a higher risk of developing a UTI compared to patients living in areas with the highest median household income (Table 3).
Complex SSI
Depression (aOR, 1.58; 95% CI, 1.08–2.32; p = 0.02) was identified as an independent predictor of developing complex SSI. Living in an area with a low household income, Medicaid status, and self-pay were not associated with an increased risk of developing complex SSI. Medicare (aOR, 0.8; 95% CI, 0.68–0.93; p = 0.005) and schizophrenia (aOR, 0.57; 95% CI, 0.33–0.99; p = 0.05) were identified as protective (Table 3).
Catheter-associated urinary tract infection
Medicare (aOR, 2.59; 95% CI, 2.06–3.26; p < 0.001), Medicaid (aOR, 1.97; 95% CI, 1.53–2.54; p < 0.001), residing in an area with a median household income in the third quartile (OR 1.21; 95% CI, 1.02–1.44; p = 0.03), depression disorder (aOR, 1.56; 95% CI, 1.03–2.36; p = 0.04), and neurodevelopmental disorders (aOR, 1.82; 95% CI, 1.08–3.08; p = 0.03) were associated with an increased risk of developing CAUTI. Patients with other psychoactive substance use disorders (aOR, 0.35; 95% CI, 0.13–0.91; p = 0.03) appeared to be protected against the development of post-operative CAUTI (Table 3).
Methicillin-resistant Staphylococcus aureus sepsis
Medicare (aOR, 1.48; 95% CI, 1.03–2.13; p = 0.03), Medicaid (aOR, 1.58; 95% CI, 1.14–2.18; p = 0.006), and opioid use disorder (aOR, 2.13; 95% CI, 1.35–3.35; p = 0.001) were identified as independent predictors of the development of MRSA sepsis (Table 3).
Sensitivity analysis: Appendectomy
We identified 64,526 patients who underwent a non-elective appendectomy at the index admission (Supplementary Table S4). Medicare (aOR, 1.15; 95% CI, 1.05–1.25; p = 0.002), Medicaid insurance status (aOR, 1.18; 95% CI, 1.08–1.29; p < 0.001), and residing in an area with the lowest household income (aOR, 1.26; 95% CI, 1.15–1.39; p < 0.001) were identified as independent predictors of 30-day infectious complications. The use of psychoactive substances (aOR, 1.77; 95% CI, 1.29–2.45; p < 0.001) and neurodevelopmental disorders (aOR, 1.72; 95% CI, 1.14–2.59; p = 0.01) were associated with an increased risk of 30-day infectious complications.
Sensitivity analysis: Colectomy
A total of 57,829 patients who underwent a non-elective colectomy during the index admission were included in this sensitivity analysis (Supplementary Table S5). Similar to our main analysis, Medicare (aOR, 1.25; 95% CI, 1.17–1.33; p < 0.001), Medicaid (aOR, 1.19; 95% CI, 1.1–1.28; p < 0.001) insurance status, and residing in an area with the lowest household income (aOR, 1.1; 95% CI, 1.02–1.19; p = 0.009) were identified as independent predictors for the development of 30-day infectious complications. Neurodevelopmental disorders (aOR, 2.26; 95% CI, 1.74–2.93; p < 0.001) were also identified as a predictor for 30-day infectious complications.
Discussion
In the present study, we found that after EGS procedures, living in a low household income area, Medicaid insurance status, neuropsychiatric comorbidities, and substance use disorders were associated with an increased risk of 30-day infectious complications and of specific infectious complications such as pneumonia, UTI, MRSA sepsis, and CAUTI.
In a recent paper, Qi et al. 27 found that in patients undergoing colectomy, Medicare insurance, Medicaid insurance, or living in a low-income neighborhood were associated with an increased risk of developing an SSI. Similarly, government insurance and a low household income are associated with an increased infection risk following orthopedic surgical procedures, 28 as well as a higher rate of infections-related re-admission compared with patients with private insurance or a higher household income.29,30 Additionally, patients with low income have been shown to have worse surgical outcomes, increased post-operative length of stay, and increased overall 30-day and 90-day post-operative mortality.30,31
Although there is a paucity of data regarding the impact of socioeconomic factors in post-operative infectious complications after EGS procedures, our findings align with what is reported in the literature for other kinds of surgical procedures. Namely, Medicare and Medicaid insurance were associated with an increased risk of developing 30-day infectious complications following EGS compared to patients with non-government health insurance. Additionally, residing in a low household-income area was also identified as an independent predictor of 30-day infectious complications following EGS procedures. In our study, similar associations between residing in a low household-income area, government insurance, and the risk of developing an infectious complication were also found for specific infection types, including pneumonia, UTI, CAUTI, and sepsis due to MRSA. Conversely, residing in a zip code area with a lower median household income and insurance status were inconsistently associated with complex SSI rates.
In the present study, patients with opioid use disorder were at an increased risk of developing 30-day infectious complications and MRSA sepsis. Similarly, in previous studies the use of illicit drugs in patients presenting for trauma was associated with an increased risk for infectious complications.32,33 The use of opiates in particular has been shown to compromise the immune system,34–38 increase the risk of community-acquired and opportunistic infections, 38,39 and is associated with post-operative infections complications.40,41
In our adjusted analysis, schizophrenia and neurodevelopmental disorders were identified as independent predictors of 30-day infectious complications after EGS procedures. Interestingly, although the impact of the different psychiatric comorbidities varied according to the specific infection type, patients with schizophrenia had an increased risk of developing pneumonia and UTI. Similarly, having a neurodevelopmental disorder was identified as an independent predictor of developing pneumonia, UTI, and CAUTI. In a recently published metanalysis, McBride et al. 42 reported that patients with serious psychiatric comorbidities had higher rates of post-operative complications and longer length of stay after surgery.
Additionally, in patients undergoing surgical procedures, the presence of psychiatric comorbidities or neurodevelopmental disorders was associated with increased post-operative complications, re-admission rates, infections, and mortality.43–48 In patients with neuropsychiatric comorbidities, the increased incidence of post-operative infections could be because of behavioral alterations, impaired communication with the healthcare providers, and variable reactions to pain and drugs, which could potentially lead to delayed diagnosis and additional challenges in the peri-operative setting, thus contributing to an increase in post-operative complications.
Our findings suggest that in the setting of socioeconomic disparity, neuropsychiatric comorbidities, and substance use disorders patients are at an increased risk of developing infectious complications after EGS. The current nationwide quality improvement framework prioritizes the prevention of hospital-acquired infections and enhancing patient safety. However pre-existing factors such as the patient's residential area household income, insurance status, and behavioral determinants of health are outside of hospital control at the time of admission and might have an unmeasured impact on hospital benchmarking. For this reason, adjusting for socioeconomic and behavioral factors in pay-for-performance programs and public reports could lead to a fairer comparison between centers and avoid the risk of penalizing hospitals that are serving underserved areas and a socially fragile patient population. Although recent efforts have been made by the U.S. Department of Health and Human Services (HHS) to investigate the impact of social determinants of health on patient outcomes,49,50 social determinants of health remain a major driver of health disparity. Our findings add to the body of evidence supporting this effort and further underline the need for addressing socioeconomic disparities in surgical patients through evidence-based health policies.
This study has limitations that must be acknowledged. First, we used a national administrative database to investigate the impact of social and behavioral determinants of health on infectious complications after EGS. Although the use of the NRD database enabled us to use large numbers of patients, variables such as patient race, hospital geographical location, and antibiotic use are not captured in the dataset. Second, this database does not capture data regarding outpatient follow-up, indication for surgery, the complexity of the surgery, surgeon volume, and hospital policies that might affect post-operative outcomes. Third, the NRD database captures only inpatient re-admission, therefore we were not able to capture patients treated in the outpatient setting or patients who elected to avoid further inpatient treatment, as might be the case in the uninsured or low-income population. Last, we included all patients undergoing non-elective abdominal general surgery procedures; although this might increase the generalizability of our findings, this resulted in a heterogeneous patient population. Future prospective studies using granular data, specifically including patient race, should be conducted to understand further the impact of intersectionality and socioeconomic disparity on the contemporary healthcare setting.
Conclusions
In patients undergoing EGS procedures, socioeconomic factors and behavioral determinants of health are associated with an increased risk of developing post-operative infectious complications. These findings warrant the inclusion of social and behavioral determinants of health in pay-for-performance programs and for the implementation of evidence-informed health policies aimed at improving post-operative outcomes and patient safety in the setting of socioeconomic disparity.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.