
Abstract
Background:
Benign gallstone disease is the most frequent indication for cholecystectomy in the United States. Many patients present with complicated disease requiring urgent interventions, which increases morbidity and mortality. We investigated the association between individual and population-level social determinants of health (SDoH) with urgent versus elective cholecystectomy.
Patients and Methods:
All patients undergoing cholecystectomy (2014–2021) for benign gallstone disease were included. Demographic and clinical data were linked to population-level SDoH characteristics using census tracts. Data were analyzed using descriptive and inferential statistics.
Results:
A total of 3,197 patients met inclusion criteria; 1,913 (59.84%) underwent urgent cholecystectomy, 1,204 (37.66%) underwent emergent cholecystectomy, and 80 (2.5%) underwent interval cholecystectomy. On multinomial logistic regression, patients who were older (relative risk [RR], 1.010; p < 0.001), black (RR, 1.634; p = 0.008), and living in census tracts with a higher percent of poverty (RR, 0.017; p = 0.021) had a higher relative risk of presenting for urgent cholecystectomy. Patients who were female (RR, 0.462; p < 0.001), had a primary care provider (PCP; RR, 0.821; p = 0.018), and lived in census tracts with low supermarket access (RR, 0.764; p = 0.038) had a lower relative risk of presenting for urgent cholecystectomy. Only age (RR, 1.066; p < 0.001), female gender (RR, 0.227; p < 0.001), and having a PCP (RR, 1.984; p = 0.034) were associated with presentation for interval cholecystectomy.
Conclusions:
Patients who were older, black, and living in census tracts with high poverty levels had a higher relative risk of presenting for urgent cholecystectomy at our institution, whereas females and patients with PCPs were more likely to undergo elective cholecystectomy. Improved access to primary care and surgical clinics for all patients at safety-net hospitals may result in improved outcomes in the management of benign gallstone disease by increasing diagnosis and treatment in the elective setting.
Cholecystectomy is the most commonly performed elective and urgent general surgery operation in the United States, with at least 300,000 performed annually.1–4 Benign gallstone disease exhibits a wide range of symptoms and presentations, but many patients undergoing urgent cholecystectomy for acute conditions such as acute cholecystitis and choledocholithiasis have a history of chronic symptomatic biliary disease. A majority of cholecystectomies in the United States are performed electively, but not all populations have equitable access to elective cholecystectomy: racial and ethnic minorities, individuals with public insurance, and those living in socially vulnerable areas undergo ambulatory cholecystectomy less frequently.5–7
Patients undergoing urgent cholecystectomy have a higher risk of post-operative complications, re-admissions, and mortality compared with their elective counterparts.2,3,8,9 Urgent cholecystectomies are also more costly and portend a longer length of stay (LOS), whereas elective cholecystectomies are often outpatient surgeries.5,10–12 Prior studies have examined this relation at state and national levels of cholecystectomy populations but there is a paucity of data specific to underserved patient populations. We sought to examine social determinants of health (SDoH) associated with urgent versus elective cholecystectomy at our academic, urban, safety-net hospital at the individual and the population levels to identify potentially modifiable factors that reduce risk of urgent cholecystectomy, which could highlight areas of intervention to increase access to elective cholecystectomy.
Patients and Methods
Data source and sample population
After Institutional Review Board approval, all patients 18 years and older who underwent cholecystectomy at our institution between July 2014 and December 2021 were identified through our institution's Clinical Data Warehouse (CDW) using Current Procedural Technology (CPT) codes for cholecystectomy with and without cholangiogram and with and without common bile duct exploration (47562, 47563, 47564, 47600, 47605, 47610, 47612, 47620). Any patients who, despite having one of these CPT codes, received a cholecystectomy for traumatic injury, gallbladder polyp(s), masses, malignancy, or as part of another operation as identified via chart review were excluded.
Primary outcome
The primary outcome of interest was the acuity of cholecystectomy performed. This was defined as elective cholecystectomy (cholecystectomy performed in an elective, planned, ambulatory setting; urgent cholecystectomy (cholecystectomy performed in an urgent or emergent setting); and interval cholecystectomy (cholecystectomy performed after prior urgent or emergent presentation managed non-operatively with percutaneous drainage or antibiotic agents). We determined whether a patient had an elective, urgent, or interval cholecystectomy using the case classification field in the electronic medical record case request order (elective or urgent/emergent) cross referenced with diagnosis on admission, prior admissions, and length of stay via chart review.
Independent variables
Demographic variables were obtained through the CDW and supplemented through manual chart review, including age, gender (male, female), and race/ethnicity (categorized as non-Hispanic white, non-Hispanic black, Hispanic, and other). Our sample included 27 languages, which we categorized as the four most common primary languages spoken: English, Spanish, Portuguese, and Haitian Creole, with all other languages categorized as “other.” Patients were classified as employed (any level of employment including part-time, freelance, self-employed), unemployed, or unknown based on chart review. Insurance status was categorized into public (Medicare and Medicaid), private, and other/none/unknown for patients who were uninsured or for whom this information was unavailable. Other clinical data obtained included body mass index (BMI) (continuous), whether the patient had a primary care provider (PCP), diagnosis leading to cholecystectomy, and case classification (elective vs. urgent vs. interval).
Patient address at the time of surgery was used to obtain population level variables by census tract. Patient addresses were geocoded and plotted into census tracts and census tract data was linked to patient data via spatial join in ArcGIS geocoding software. Census tract variables included percent of census tract living in poverty, median income, percent of census tract with less than a high-school diploma, percent of census tract without internet, dollars spent on food annually, low supermarket access, low income, and food desert designation. These variables were extracted from PolicyMap, a data warehouse and mapping platform that compiles population data from publicly available sources including the American Community Survey and the Economic Research Service/United States Department of Agriculture (ERS/USDA) Food Access Research Atlas. The USDA defines low supermarket access as at least one-third of the population living farther than 0.5 miles from a supermarket in an urban setting and 10 miles in a rural setting; low income as a poverty rate of at least 20%; and a food desert as a census tract with low supermarket access or low income. 13
Statistical analysis
Continuous variables are reported as mean ± standard deviation (SD) for normally distributed variables and median and interquartile ranges (IQR) for non-normally distributed variables. Categorical variables are reported as numbers and percentages. Categorical variables were compared using Pearson χ 2 tests. Continuous variables were analyzed using analysis of variance (ANOVA) and Kruskal-Wallis tests for parametric and non-parametric variables, respectively. A stepwise approach was used to create a multivariable logistic regression adjusted for factors significantly associated with the acuity of cholecystectomy (elective, urgent, or interval) on univariable analysis. Statistical analyses were performed using STATA, version 14 (StataCorp LP, College Station, TX) and statistical significance was set at α = 0.05.
Results
Sample characteristics
We identified 3,427 patients who underwent cholecystectomy during our study period. After excluding patients receiving a cholecystectomy for traumatic injury, gallbladder polyp(s)/masses, malignancy, or as part of another operation, there were 3,197 patients left for analysis. Demographically, our sample was 75% female, 48% Hispanic, 50% English-speaking, 58.5% unemployed, 73% publicly insured, and 68.7% of patients had a PCP. The median age was 44 years (IQR, 33–58) and the mean BMI was 31.2 (SD, 6.91) (Table 1). Geographically, our population came from neighborhood clusters across a relatively broad area (Fig. 1). Our whole cohort lived in census tracts with more than 15% of people living in poverty, a highest median income of slightly over $60,000 per year, a highest average of approximately $8,000 spent on food annually, a 76% to 78% low income rate, a 37% to 43% rate of people living in a food desert, and a 53% to 63% rate of low supermarket access (Table 2).
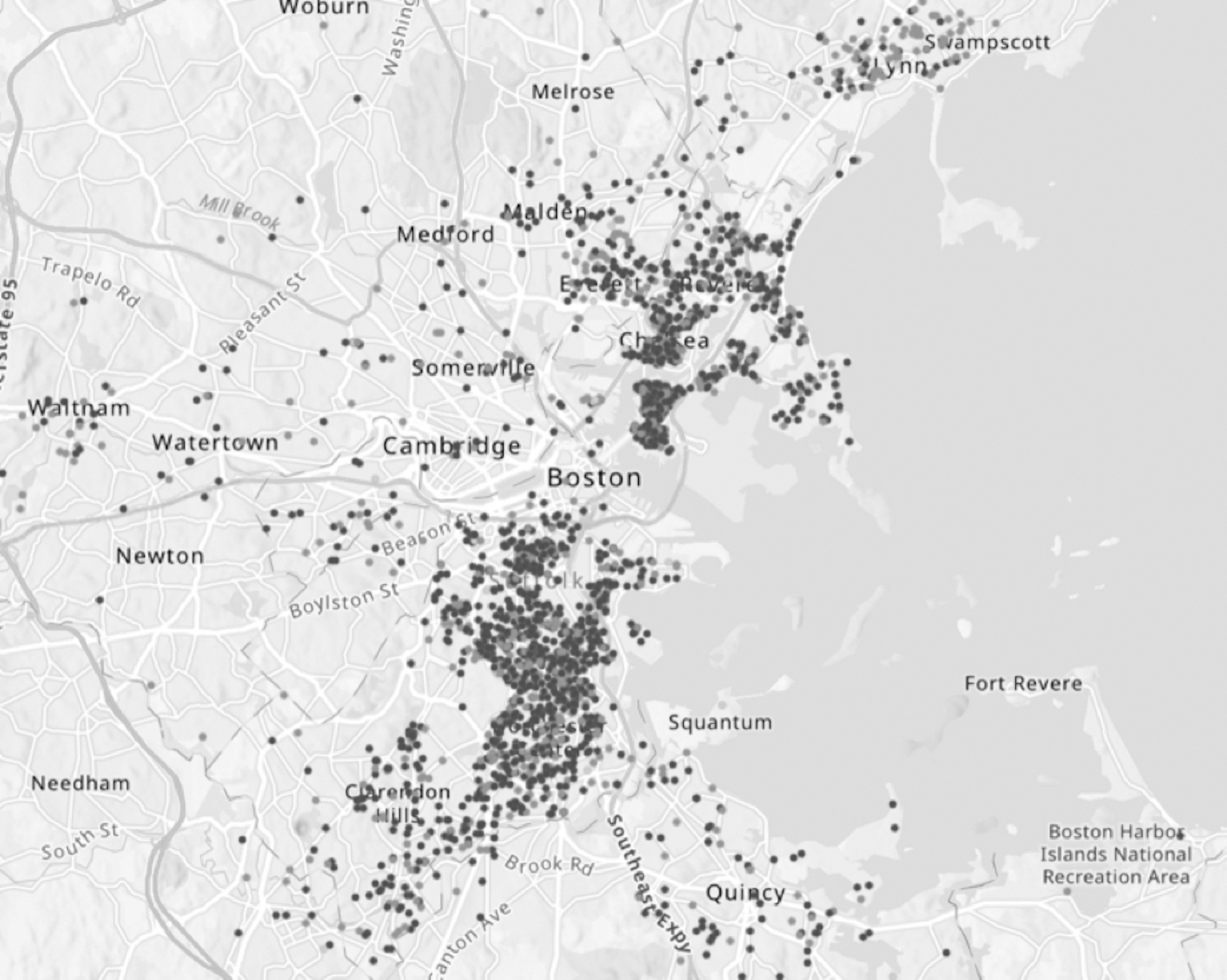
Our institution's cholecystectomy population focusing on neighborhoods around Boston. Elective cholecystectomy patients are represented with black dots, urgent cholecystectomy with dark gray dots, interval cholecystectomy with light gray dots.
Individual-Level Characteristics of Patients Undergoing Elective, Urgent, and Interval Cholecystectomy
IQR = interquartile range; BMI = body mass index; SD = standard deviation; PCP = primary care provider.
Population-Level Characteristics of Patients Undergoing Elective, Urgent, and Interval Cholecystectomy
IQR = interquartile range; SD = standard deviation.
Univariable analysis
Most patients underwent urgent cholecystectomy (n = 1,913; 59.84%), whereas 1,204 (37.66%) underwent elective cholecystectomy, and 80 (2.5%) presented for interval cholecystectomy. Demographic and clinical characteristics by cholecystectomy acuity are presented in Table 1. In univariable analysis of these characteristics, age, gender, race/ethnicity, primary language spoken, employment status, indication for cholecystectomy, completing the cholecystectomy laparoscopically, and having a PCP were all associated with the acuity of cholecystectomy.
Population level characteristics of the cohort by cholecystectomy acuity are presented in Table 2. In univariable analysis of SDoH at the census tract level, there was a significant difference among the three groups for percent living in poverty (p < 0.001; Fig. 2), dollars spent on food annually (p = 0.009), residence in a food desert (p = 0.038), and low supermarket access (p < 0.001). A higher percentage of the urgent and interval cholecystectomy cohorts lived in census tracts with more poverty and less money spent on food annually.

Our institution's cholecystectomy population overlaid onto percent of census tract living in poverty, where darker purple represents a higher percentage of patients in that census tract living in poverty. Elective cholecystectomy patients are represented with black dots, urgent cholecystectomy with dark gray dots, interval cholecystectomy with light gray dots.
Multivariable analysis
We created a multinomial logistic regression using a stepwise approach controlling for variables found to be significantly associated with acuity of cholecystectomy on univariable analysis, including age, gender, race/ethnicity, employment status, having a PCP, living in poverty, dollars spent on food annually, residence in a food desert, and low supermarket access. There was significant collinearity between race/ethnicity and language spoken; we chose to control for race/ethnicity in the final model, because we believe race/ethnicity is more representative of a patient's SDoH than language spoken. There was also collinearity between the diagnosis leading to cholecystectomy, the operation being performed laparoscopically, and the acuity of cholecystectomy, so diagnosis and approach were similarly omitted from the final model.
On multinomial logistic regression, we found that patients who were older (RR, 1.010; p < 0.001), black (RR, 1.634; p < 0.001), and residing in a census tract with higher levels of poverty (RR, 1.017; p = 0.008) had a higher relative risk of presenting for urgent compared with elective cholecystectomy. Patients who were female (RR, 0.462; p < 0.001), had a PCP (RR, 0.821; p = 0.018), and lived in census tracts with lower supermarket access (RR, 0.764; p = 0.038) had a lower relative risk of presenting for urgent compared with elective cholecystectomy (Table 3). Comparing interval with elective cholecystectomy, patients who were older (RR, 1.06; p < 0.001) and had a PCP (RR, 1.984; p = 0.034) also had a higher relative risk of presenting for interval cholecystectomy, whereas females (RR, 0.227; p < 0.001) had a lower relative risk of presenting for interval surgery.
Multinomial Logistic Regression of Factors Associated With Receipt of Urgent and Interval Cholecystectomy
CI = confidence interval; PCP = primary care provider.
Discussion
In this study, we examined SDoH and social risk factors associated with presenting for elective versus urgent cholecystectomy in a safety-net hospital population. Our patient cohort differed from the national cholecystectomy population, as nationally a majority of cholecystectomies are performed electively, whereas at our institution, a majority of cholecystectomies were performed urgently. 1 Also, the national cholecystectomy population is mostly white and privately insured, whereas only 19% of our cholecystectomy patients were white and 17% were privately insured.14–16 We found that patients who were older, black, and residing in census tracts with higher levels of poverty had a higher relative risk of presenting for urgent cholecystectomy rather than elective cholecystectomy. Although we found some significant differences in the SDoH of the census tracts of patients undergoing urgent versus elective versus interval cholecystectomy, the population we evaluated is generally underserved.
Our study was consistent with prior studies examining risk of urgent surgery. Many studies have demonstrated that non-white patients are more likely to undergo urgent surgery and less likely to undergo elective surgery, likely because of structural barriers to care.5,14,15,17–20 These barriers include provider bias in referrals and surgical recommendations as well as socioeconomic characteristics associated with being of minority race such as worse access to insurance, transportation, and housing.17–19 In our study, patients who were female, had a PCP, and lived in census tracts with lower supermarket access had a higher relative risk of undergoing elective cholecystectomy. Females have a higher incidence of gallstone disease and providers likely have a higher index of suspicion for benign gallstone disease when females present with chronic abdominal complaints.21–23 This could explain the association we found between female gender and elective cholecystectomy. Furthermore, females are more likely to engage in healthcare and seek primary care, which are often prerequisites to undergoing elective cholecystectomy.24,25
The finding that patients living in areas of lower supermarket access have a lower relative risk of presenting for urgent cholecystectomy can be perplexing. Although we do not have information regarding the specific shopping habits of the populations in these census tracts, we hypothesize that traveling longer distances to access a supermarket may lead to different shopping and food consumption habits. These behaviors may thus affect presentation with biliary pathology. In contrast to this finding, prior studies have demonstrated that income and food security, rather than supermarket proximity alone, impact health outcomes for diabetes mellitus, cardiovascular disease, and kidney stone disease. 26–28
We also examined the population of patients who underwent interval cholecystectomy. Most patients managed with interval cholecystectomy are poorly optimized for surgery at the time of their acute presentation, and instead are managed with percutaneous cholecystostomy tube placement and antibiotic agents as a temporizing measure until they are optimized for interval cholecystectomy. We found patients in the interval cholecystectomy population were more likely to have a PCP, possibly because these patients already had chronic medical comorbidities requiring active PCP management. The interval cholecystectomy patients were also older, likely with less physiologic reserve to tolerate an operation, resulting in initial non-operative management. If these patients presented to clinic with symptoms of biliary colic, they may have been considered too high risk to undergo elective surgery. However, when these patients developed acute cholecystitis or cholangitis, they were too sick to undergo an emergent operation as well.
Although age, gender, and race/ethnicity are not modifiable factors in this population, access to primary care is modifiable. Our findings emphasize the overwhelming evidence in support of expanding primary care for vulnerable populations as a way to improve health outcomes.29–32 Strengthening partnerships with community health centers, connecting patients in the emergency department with PCPs, and providing patient instructions in the patient's primary language are all interventions that could improve access to elective cholecystectomy at our institution. On a larger scale, advocating for improved primary care services for the elderly and racial/ethnic minorities may improve overall access to elective cholecystectomy.
Additionally, we found that poverty, also a modifiable variable, was associated with urgent cholecystectomy. This finding adds to the growing body of literature suggesting that poverty is associated with adverse medical and surgical outcomes.33–39 Although 11.3% of census tracts nationally have high levels of poverty, 16.3% of the census tracts among our population had high levels of poverty. 40 Many aspects of poverty are mediated at the state and national levels, but advocacy for policy change to eliminate poverty in the United States is an avenue through which the medical community can contribute to improved healthcare outcomes for underserved populations.
Because of constraints on hospital bed availability and operating room time, not all patients presenting to the emergency department with biliary colic can be offered cholecystectomy. However, we recognize that this presentation is an opportunity to intercept patients, lest they re-present more acutely and require a riskier operation with a longer hospital stay in the future. Ideally, patients discharged from the emergency department with biliary colic would be able to follow up in a general surgery clinic and be scheduled for elective cholecystectomy. However, this can be challenging because of issues such as unreliable transportation, inability to leave work, and family obligations, among others. Offering cholecystectomy to patients in the emergency department while they are stable and without complicated biliary disease could benefit patients, surgeons, and hospitals by leading to safer operations with fewer complications and reduced LOS. Future research could examine the outcomes of patients presenting to the emergency department with non-urgent benign gallstone disease who do not undergo surgery, and whether these patients are subsequently seen by PCPs, general surgeons, continue to present to the emergency department, or are lost to followup.
This study has several limitations. First, it is a single institution study and the patient population at our urban safety-net hospital differs from the national cholecystectomy population. Thus, our results are not generalizable to the entire U.S. population but do likely apply to other institutions that serve traditionally marginalized communities. Second, our patients generally live in underserved neighborhoods with high poverty rates, low incomes, and limited access to supermarkets. This limits our ability to evaluate the association between population level SDoH and the receipt of elective, urgent, or interval cholecystectomy. A similar study including multiple institutions or institutions serving patients with broader socioeconomic differences could help identify whether the population level variables we studied are in fact associated with the risk of urgent versus elective cholecystectomy.
Conclusions
Older, black, and patients living in census tracts with higher poverty have a higher relative risk of presenting for urgent cholecystectomy at our institution, whereas females, patients with a PCP, and patients living in areas with low supermarket access are more likely to receive elective cholecystectomy. Improved access to primary care and surgical clinics for all patients at safety-net hospitals may result in improved outcomes in the management of benign gallstone disease by increasing diagnosis and treatment in an elective, ambulatory setting. Further research is needed to elucidate the mechanisms through which population-level SDoH and individual social risk factors impact access to elective cholecystectomy.
Footnotes
Acknowledgments
Thank you to the Boston University/Boston Medical Center chapter of Socially Responsible Surgery for assisting with data acquisition.
Authors' Contributions
Conceptualization: Myers, Kenzik, Dechert, Sanchez. Analysis: Sanchez. Data curation: Myers. Investigation: Myers. Methodology: Myers, Kenzik, Sanchez. Software: Sanchez. Resources: Myers, Kenzik, Allee. Writing: Myers, Dechert, Theodore, Jaffe, Sanchez. Supervision: Kenzik, Sanchez. Funding acquisition: Allee.
Funding Information
There were no relevant financial relations or sources of support in the form of grants, equipment, or drugs.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.