
Abstract
Background:
Despite the high prevalence of post-operative fever, a variety of approaches are taken as to the components of a fever evaluation, when it should be undertaken, and when empiric antibiotic agents should be started.
Hypothesis:
There is a lack of consensus surrounding many common components of a post-operative fever evaluation.
Patients and Methods:
The Surgical Infection Society membership was surveyed to determine practices surrounding evaluation of post-operative fever. Eight scenarios were posed in febrile (38.5°C), post-operative general surgery or trauma patients, with 19 possible components of work-up (physical examination, complete blood count [CBC], fungal biomarkers, lactate and procalcitonin [PCT] concentrations, cultures, imaging) and management (antibiotic agents). Each scenario was then re-considered for intensive care unit (ICU) patients (intubated/unstable hemodynamics). Agreement on a parameter (<1/4 or >3/4 of respondents) achieved consensus, positive or negative. Parameters between had equipoise; α was set at 0.05.
Results:
Among the examined scenarios, only CBC and physical examination received positive consensus across most scenarios. Blood/urine cultures, imaging, lactate, inflammatory biomarkers, and the empiric administration of antibiotic agents did not reach consensus; support was variable depending on the clinical scenario, illness severity, and the individual preferences of the answering clinician. The qualitative portion of the survey identified “fever threshold and duration,” “clinical suspicion,” and “physiologic manifestation” as the most important factors for deciding about the initiation of a fever evaluation and the potential empiric administration of antibiotic agents.
Conclusions:
There is consensus only for physical and examination routine laboratory work when initiating the evaluation of febrile post-operative patients. However, there are multiple components of a fever evaluation that individual respondents would select depending on the clinical scenario and severity of illness. Parameters demonstrating equipoise are potential candidates for formal guidance or pragmatic prospective trials.
The incidence of post-operative fever can vary widely depending on the operation performed and the definition used, but it is, nonetheless, a common occurrence.1–3 There is a well-documented association between the tissue injury caused by surgery and elevations in pyretic cytokines, offering a physiologic explanation for this phenomenon.4–6 However, despite this knowledge, the untargeted fever evaluation, or work-up, remains ingrained in the care of post-operative patients with up to 50% of patients in contemporary cohorts undergoing diagnostic testing for fever. 7
The low yield and unnecessary increased cost associated with a broad battery of tests for post-operative fever has been documented in numerous studies dating back decades.1,8–11 However, in practice, clinicians balance this knowledge with the potential ramifications of delayed diagnosis or treatment of infection. 12 Perhaps, as with the overuse of antibiotic agents without documented infection, fear of missing an infection overrides the knowledge that an untargeted fever work-up is not likely to yield clinically useful results.13,14
Despite multiple published entreaties, fever evaluation in post-operative patients remains challenging, with continued ramifications for healthcare cost. As Dionigi et al. 15 espoused in 2006: “Perhaps more money is wasted in the evaluation of early postoperative fever than on any other aspect of postoperative care.” This survey examined how surgeons approach the evaluation of febrile post-operative patients based on a variety of case scenarios, seeking to identify areas of both agreement or equipoise that could be the targets of research efforts or formal guidance. The primary hypothesis being that, depending on the clinical scenario, there would be areas of controversy surrounding the appropriate approach to fever evaluation.
Patients and Methods
Survey design/contents
This web-based survey was distributed to the membership of the Surgical Infection Society (SIS) by e-mail between August 1 and November 30, 2022. Monthly reminder e-mails were sent during the period of data collection. The research questions and survey format were designed by the Scientific Studies Committee (SSC) of the SIS and hosted on Google Forms (Alphabet, Inc., Mountain View, CA.) A work group of the SSC first developed the survey format and the primary parameters of the survey before distributing it to the remaining members of the SSC. The entire SSC was then asked to complete the survey, provide suggestions, and identify portions of the survey that required clarification prior to distributing the survey more broadly. For each participant, an e-mail address was collected to serve as a unique identifier and prevent duplicate responses. In the event of duplicate respondents, a complete survey with the most recent timestamp was used. All survey responses were deidentified after data extraction and prior to data analysis. Additional demographic data that were collected included primary practice location and geographic region, years of post-training practice, primary field, description of practice environment (e.g., academic clinical faculty, private practice, still in training) and prior leadership roles (e.g., department chair, program director). The survey instrument/clinical scenarios can be found in the Supplementary Appendix.
The study was divided into sections to determine the effect of post-operative day (i.e., 0, 1, 3, 5), degree of temperature elevation (38.0°C vs. 38.5°C), initial surgery (general surgery (wound classes 1–4) and trauma (negative laparotomy, splenectomy, mesenteric injury, colon injury), additional symptoms (upper respiratory symptoms, dysuria/hematuria, unilateral limb swelling, rigors, abdominal pain), the appearance of the incision, and the presence of artificial devices (Foley catheters, abdominal drain, central venous catheter, epidural catheter, endotracheal tube/tracheostomy) on a respondent's selected approach to fever evaluation.
For each section, participants were given a case scenario and instructed to identify how they would manage a post-operative patient (immunocompetent and without major comorbidities) with a fever of unknown origin. For each scenario, there were 18 fever work-up components, from which any number could be selected. Those components were physical examination; complete blood count (CBC); procalcitonin (PCT); β-
The final portion of the survey provided three, open-ended response questions: “What criteria should be met prior to initiating an infectious work-up in a post-operative patient?”; “What would you consider to be the ‘ideal’ infectious “work-up” for a patient that doesn't have a clear source of infection?”; and “What criteria should be met before starting empiric (antibiotic agents) in a patient without a documented source of infection?”
Analysis/statistics
Consensus surrounding an individual fever evaluation component for each scenario was determined based on quartile of respondents: >75% of respondents (positive consensus), 50% to 75% (no consensus, leans yes), 25% to 50% (no consensus, leans no), <25% (negative consensus). Data are reported as either means with standard deviations (SD) or counts with percentages for continuous and categorical variables, respectively. Themes for qualitative responses were coded using an iterative process. Responses were first reviewed by three independent reviewers (PD, JS, SS) who independently identified themes within the responses. These themes were then compiled and re-distributed to the reviewers for consensus on identified themes. Finally, each of the reviewers re-coded the responses based on the consensus themes (Fig. 1). To achieve consensus on identified themes within a response, two-thirds of reviewers were required to code identical themes. Any question without consensus among reviewers was discussed until consensus could be achieved. All statistical analyses and figures were designed and completed in R 4.2.1 (The R Foundation for Statistical Computing, Vienna, Austria.)
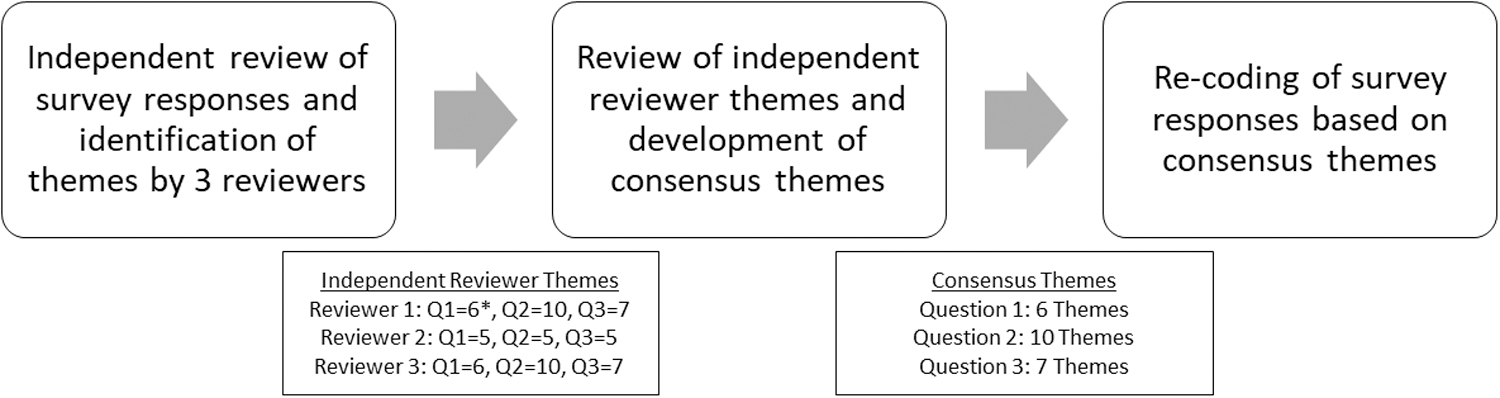
Process for development of consensus themes amongst qualitative survey responses. Q = question.
Results
Demographic data
A total of 47 survey responses were used for final analysis (one survey was excluded for being <50% complete, whereas eight responses were excluded for being from duplicate respondents). Most respondents identified a primary practice location within the United States (n = 38; 81%) and at an academic medical center (n = 41; 87%). Approximately one-half of respondents also reported having >15 years of experience post-training. The remainder of collected demographic variables can be found in Table 1.
Demographic Data for Survey Respondents
ICU = intensive care unit; PD = program director; PGY = post-graduate year.
Non-ICU scenarios
The provided survey had a total of 42 clinical cases that can be broadly categorized into non-ICU (n = 30) and ICU (n = 12) scenarios. To analyze the utility of a component of the fever work-up more broadly, the number of non-ICU scenarios was tabulated of the possible 30 in which that element achieved positive or negative consensus. For each of these scenarios, each potential element was categorized as to the integer number of scenarios in which that component achieved positive consensus (>75% indicated they would utilize), leans yes (50%–75%), leans no (25%–50%), and achieved negative consensus (<25%). Only two components, namely physical examination and CBC, achieved positive consensus across all 30 non-ICU scenarios (Table 2).
Summary of Non-ICU Scenarios (n = 30) by Quartile of Respondents Who Selected an Individual Fever Work-Up Component
ICU = intensive care unit; CT = computed tomography; A/P = abdomen/pelvis; US = ultrasound; DVT = deep venous thrombosis.
Conversely, several components achieved negative consensus across all or nearly all of the same 30 scenarios with <25% of respondents selecting that component at the following rates: PCT (n = 26 of 30 scenarios; 87%), β-
ICU scenarios
Among the 12 ICU scenarios, only physical examination and CBC received positive consensus across all scenarios (Table 3). By contrast, there were several fever work-up components that achieved negative consensus across all, or nearly all, of the same 12 ICU scenarios: β-
Count of All ICU Scenarios (n = 12) by Quartile of Respondents Who Selected an Individual Fever Work-Up Component
ICU = intensive care unit; CT = computed tomography; US = ultrasound; A/P = abdomen/pelvis; BAL = bronchoalveolar lavage; DVT = deep venous thrombosis.
Qualitative responses
At the conclusion of the survey, participants were given the opportunity to answer several open-ended questions, to which 27 participants (57%) chose to respond. The first question was related to criteria that should be met prior to initiating an infection work-up in a post-operative patient. There were five primary themes that were identified among the responses: fever threshold/duration; physiologic manifestation; patient/case factors; laboratory values; and clinical suspicion. A summary of these themes and their frequency within the responses is shown in Figure 2. The presence of a fever and its proximity to surgery were the themes encountered most throughout the responses, but identified within the responses at a nearly equal frequency (n = 14) was the general concept of clinical suspicion by the treating provider without definitive criteria, as shown by excerpts in Table 4.

Percentage of total responses (n = 25) that contain each of the identified themes for the following open-ended question: “What criteria should be met prior to initiating an infectious work-up in a post-operative patient?”
Select Individual Responses to Open-Ended Survey Questions Regarding Criteria for Initiation of a Fever Work-Up
The second open-ended question asked participants to identify the components of an ideal fever work-up without a clear source of infection. The frequency of components that were identified among the responses can be seen in Figure 3. However, eight (30%) of the recorded responses had “no ideal work-up/targeted work-up” as the primary theme of the response. Example responses can be found in Table 5.
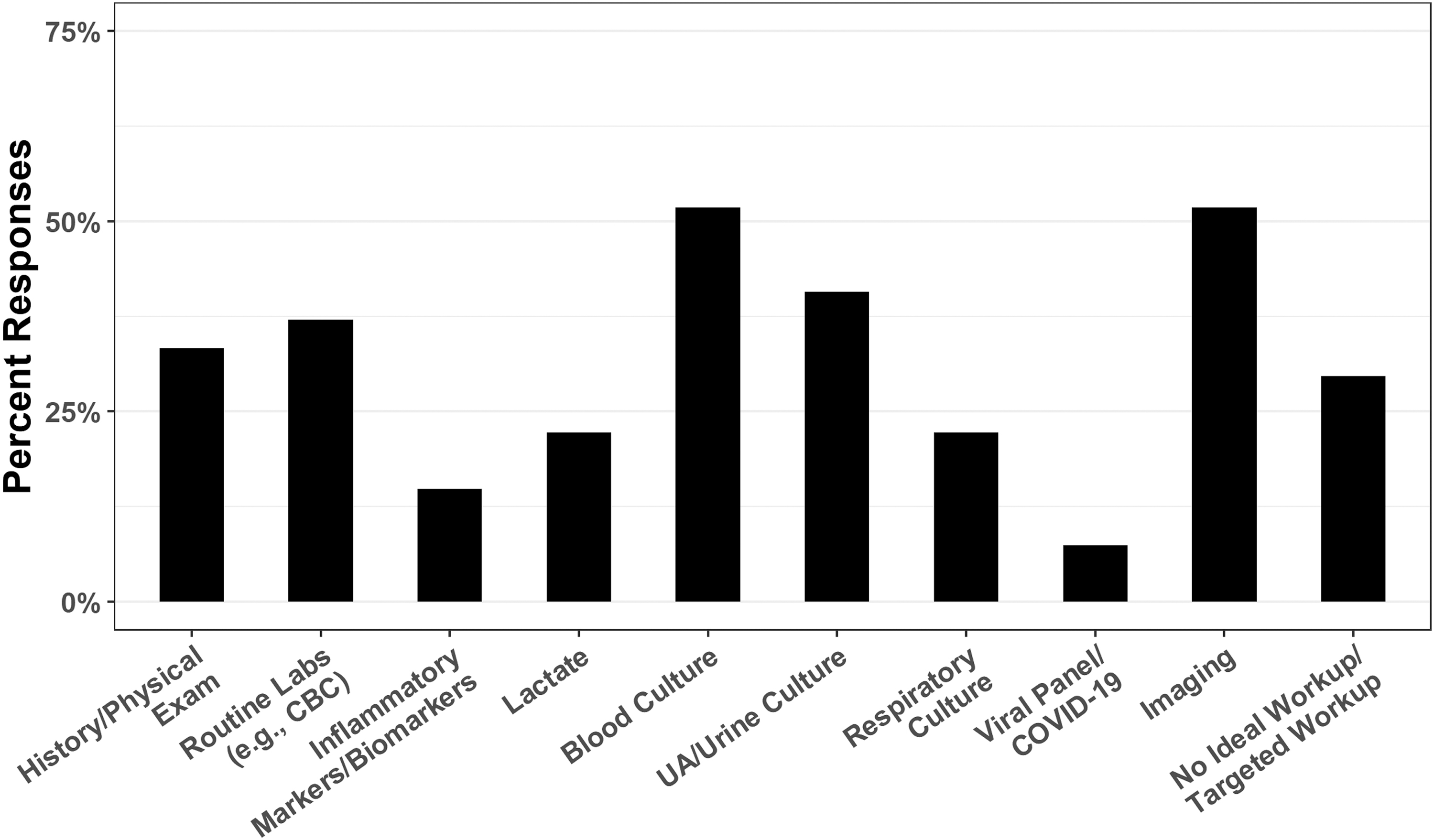
Percentage of total responses (n = 27) that contain each of the identified themes for the following open-ended question: “What would you consider to be the ‘ideal’ infectious “work-up” for a patient that doesn't have a clear source of infection?” UA = urinalysis; CBC = complete blood count.
Select Individual Responses to Open-Ended Survey Questions Regarding Components of an Ideal Fever Work-Up
Finally, respondents were asked what criteria should be met before starting empiric antibiotic therapy (i.e., without a documented source of infection). The general themes identified within this section were similar to those for the first open-ended question, with the exception of adding “targeted antibiotic duration/section” and “never.” The themes identified most commonly included “fever threshold/duration” and “physiologic manifestation” (Fig. 4; Table 6).

Percentage of total responses (n = 27) that contain each of the identified themes for the following open-ended question: “What criteria should be met before starting empiric (antibiotic agents) in a patient without a documented source of infection?”
Select Individual Responses to Open-Ended Survey Questions Regarding Criteria for Initiation of Empiric Antibiotic Agents
Discussion
This study demonstrated several areas of widespread agreement among individual surgeons for the evaluation of post-operative fever in a variety of ICU and non-ICU scenarios, namely physical examination and CBC for all scenarios. Regarding negative consensus, the use of fungal markers or empiric antifungal agents was almost ubiquitously rejected regardless of scenario (ICU or non-ICU). Also, there was >80% negative consensus for the routine use of PCT, sputum cultures, and respiratory viral panels in non-ICU patients. However, it also shed light on a variety of components (e.g., lactate, blood culture, urine culture) that respondents opined had only situational utility, or that equipoise was demonstrated. Whereas it seems that the general principle of avoiding broad, untargeted work-ups for febrile post-operative patients is reflected in the responses to this survey, there are still clearly areas of disagreement in which formal organizational guidance or targeted research studies may provide clarity for active clinicians.
Consensus regarding obtaining blood culture was lacking among surveyed surgeons. Although on the surface, the lack of positive consensus for obtaining routine blood and urine culture to evaluate febrile post-operative patients aligns with studies demonstrating low diagnostic utility, neither is there widespread support for their avoidance.1,16–21 In fact, equipoise existed for blood culture for 77% of scenarios in non-ICU patients and 83% of ICU scenarios, with a similar distribution for urine culture (64% non-ICU; 100% ICU). Copeland-Halperin et al. 16 found the overall incidence of blood culture true-positivity to be approximately 4% for post-operative patients within 10 days of an operation, but by multivariable analysis the incidence of positive blood culture increased to approximately 37% among patients at highest risk, with the primary drivers being surgical specialty (cardiac, otolaryngology, obstetrics, and urology being highest risk), greater time since procedure, and maximum temperature (highest risk, >102.5°F). 16
Although there was no statistical difference among the scenarios with respect to the procedure performed, more respondents selected blood culture as the post-operative day increased for non-ICU (post-operative day 0, 11%; post-operative day 1, 25%; post-operative day 3, 49%; post-operative day 5, 55%; p < 0.001) and ICU scenarios (post-operative day 0, 40%; post-operative day 1, 51%; post-operative day 3, 77%; post-operative day 5, 85%; p < 0.001).
These data also need to be put into the context of current consensus guidelines for fever work-up in the ICU from the Infectious Diseases Society of America/American College of Critical Care Medicine. 22 O'Grady et al. 22 make a specific recommendation against performing any routine assessments outside of a physical examination in the first 72 hours in post-operative patients (to include blood culture, urine culture, or CXR) because of the low yield of these tests. However, at least 40% of respondents reported that they would obtain a blood culture on post-operative day 0 in critically ill patients, suggesting that this recommendation is either not widely known or behavior is not widely in conformance.
Whereas the study was not designed specifically to examine the work-up for non-infectious causes of fever, participants were provided with the option to obtain cross-sectional imaging of the chest or abdomen to potentially search for PE or intra-abdominal complications of surgery. They were also provided with the opportunity to obtain a DVT US. Considering that Barie et al. 11 described the incidence of an infectious source being identified in febrile, post-operative ICU patients at approximately 10% in the first 72 hours and 46% overall, it seems that the search for a non-infectious source would have been utilized more heavily. However, CT abdomen/pelvis did not receive positive consensus for any of the scenarios examined, even in the setting of a post-operative patient with worsening abdominal pain (27/47 respondents; 57%, no consensus, leans yes).
Similarly, DVT US only obtained positive consensus in a single scenario in a febrile patient with unilateral limb swelling. Considering that most scenarios examined the early post-operative period (72 hours), it is somewhat surprising that there was much more support for infectious rather than non-infectious work-ups. Furthermore, the pursuit of non-infectious causes of fever was not mentioned in any of the open-ended responses.
By contrast, PCT had little support among either the ICU or non-ICU scenarios, there being no scenarios in which >50% of respondents reported inclusion as part of their evaluation. This finding was somewhat surprising considering the mounting evidence that PCT likely has some benefit in monitoring the treatment of bacterial infections and sepsis.23,24 Whereas its exact role in post-operative patients remains to be elucidated fully, PCT seems to have some utility if cutoff thresholds are adjusted higher because of stimulation of a PCT response by surgical tissue injury. 25 Cross-sectional imaging (i.e., CT abdomen/pelvis) received more support, but there was still only a single non-ICU scenario in which >50% of respondents reported that they would utilize it (worsening abdominal pain in a post-operative febrile patient) and seven of 12 ICU scenarios in which >50% of respondents reported that they would utilize it. Again, this contrasts somewhat with the literature, particularly the work of da luz Moriera et al., 3 considering that under the proper circumstances it may be more likely to yield an appropriate diagnosis at, perhaps paradoxically, lower overall cost.
When respondents were asked in an open-ended fashion to identify factors that they would utilize to determine either the need for a fever work-up or for initiation of empiric antibiotic agents, respondents indicated that they put the most weight on magnitude of fever, their own clinical suspicion for infection, and any physiologic manifestations of illness. Superficially this is consistent with myriad recent studies supporting the use of more targeted approaches to the febrile post-operative patient,3,26–30 but these data also suggest inconsistency of execution. Perhaps a widely utilized algorithm or updated guideline for the evaluation of fever in post-operative patients might lead to more uniformity. Russo et al. 31 demonstrated that implementation of an internal guideline can lead to a marked reduction in both cost (−60%) and time to treatment (−78%.) Similarly, Kendrick et al. 2 showed no increase in comorbidities with the implementation of a risk-stratified approach to the fever work-up in post-operative gynecology patients. Or, perhaps, this is an area where technology should be utilized to improve the diagnostic accuracy of individual clinicians. In 2012, Fadlalla et al. 30 described their attempt at creating a computerized, clinical support tool to assist clinicians with diagnosis of infections, although this model was too limited for clinical practice, the overall goal continues to have merit.
Kane et al. 32 described a clearly higher incidence of pulmonary infections in trauma patients compared with non-trauma surgical patients and a higher incidence of abdominal infections in the latter. However, there were no statistically significant difference in the proposed infectious work-ups when comparing trauma patients with non-trauma patients within the responses of this survey.
The limitations of this survey-based study design are several. First, although the scenarios were designed and tested by the membership of the Scientific Studies Committee of the SIS before distribution, they were not validated externally. Individual respondents may have interpreted scenarios in a manner unintended by the authors. Furthermore, the scenarios were designed to be straightforward, with limited parameters, so that the effects of individual variables could be examined. However, there are many other factors that might influence a surgeon to customize their evaluation (e.g., comorbid conditions, the results of history and physical examination, specific operative details) that were excluded purposely from the provided scenarios. This may have biased individual surgeons in reporting a narrower, or broader, evaluation. In fact, even amongst the excluded duplicate responses, an individual's responses varied by an average of 33%, suggesting that a respondent's opinion regarding this topic is fluid or that the survey lacked the specificity to evoke the same response over multiple reads.
The study was also only distributed to the SIS membership, which may not be reflective of the broader surgical community. The survey was distributed as a public access link, so it is impossible to accurately report a survey response rate. However, if the survey population was considered to be the active membership of the SIS (approximately 300 members) the response rate would be approximately 15%. It is also difficult to calculate a margin of error with certainty, but using the above assumptions would result in a margin of error of 11% at a confidence level of 90%. The small sample size may introduce potential response bias into the results. Because these case scenarios were theoretical, it is also impossible to determine whether the proposed work-up for each scenario was appropriate or cost-effective. Moreover, these data represent an approach to theoretical clinical scenarios, thus it is possible that the clinical practice of each surgeon may not comport with their response to a survey.
In conclusion, this study suggests that there is consensus only for the utility of physical examination and CBC work in the evaluation of post-operative fever. However, of the multiple components that we tested, there exists equipoise surrounding the utility of many of these components. In particular, consensus was lacking regarding blood culture, urine culture, lactate, and CXR in both ICU and non-ICU patients, with the addition of PCT, cross-sectional imaging, and bronchoscopy/bronchoalveolar lavage for those who are critically ill. Targeted trials or pragmatic guidelines may be beneficial for standardizing the evaluation of post-operative patients with fever, with particular focus on those variables with considerable equipoise.
Footnotes
Scientific Studies Committee of the Surgical Infection Society
Rondi Gelbard (University of Alabama at Birmingham, Birmingham, AL), Sebastian Schubl (University of California, Irvine, Orange, CA), Jonathan Wisler (The Ohio State University Wexner Medical Center in Columbus, OH), George Koch (Vanderbilt University Medical Center, Nashville, TN), Gregory Priebe (Boston Children's Hospital, Boston, MA) Joseph Cuschieri (University of California, San Francisco, San Francisco, CA), Jennifer Leonard (Washington University in St. Louis, St Louis, MO) John Berne (Florida International University, Fort Lauderdale, Florida), Deepak Ozhathil (University of Texas Medical Branch at Galveston, Galveston, TX), Jacob Edwards (University of Tennessee, Knoxville, TN), Amy McDonald (Case Western Reserve University, Cleveland, Ohio), Patrick Delaplain (Boston Children's Hospital, Boston, MA), Sabrina Goddard (University of Alabama at Birmingham, Birmingham, AL), Elizabeth Krebs (Vanderbilt University Medical Center, Nashville, TN), Christopher Guidry (University of Kansas Medical Center, Kansas City, Kansas), and Catherine Hunter (Oklahoma University Health, Oklahoma City, OK).
Funding Information
No external funding source was obtained or utilized for this project.
Author Disclosure Statement
None of the authors of this paper have relevant financial disclosures related to this project. As a voluntary, survey-based study, this study is exempt from institutional board review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.