
Abstract
Background:
Necrotizing soft tissue infections (NSTIs) are rare but deadly infections that require early and often extensive surgical debridement. After debridement, patients frequently have substantial morbidity because of large, open wounds.
Hypothesis:
Negative pressure wound therapy with instillation (NPWTi) results in higher wound closure rates compared with traditional negative pressure wound therapy (NPWT) or wet to dry dressings (moist wound care dressing).
Patients and Methods:
A prospectively maintained Acute and Critical Care Surgery database spanning 2008–2018 was queried for patients with a diagnosis of necrotizing fasciitis, Fournier gangrene, or gas gangrene. Data were collected on patient comorbidities, operative management, and clinical outcomes. Patients were stratified by use of moist wound care dressing, traditional NPWT, or NPWTi. Data were analyzed using analysis of variance (ANOVA), χ2, and logistic regression.
Results:
During the 10-year study period, patients were treated for NSTI; 173 were managed with moist wound care dressing, 150 with NPWT, and 48 with NPWTi. Patients were similar in terms of demographics, body mass index (BMI), diabetes mellitus, and smoking rates. Overall, complication rates were not substantially different, but mortality was higher in the moist wound care dressing group (16.2% vs. 10.7% NPWT vs. 2.1% NPWTi; p = 0.02). In the moist wound care dressing group, 81.5% of patients had an open wound at discharge compared with 52.7% of the NPWT group and only 14.6% of the NPWTi group (p < 0.001). On multivariable regression, NPWTi was associated with closure rates five times higher than the NPWT group (odds ratio [OR], 5.28; 95% confidence interval [CI], 2.40–11.61; p < 0.001) after controlling for smoking status, intravenous drug use, number of operations, and involvement of the most common region of the body.
Conclusions:
Negative pressure wound therapy with instillation is associated with higher rates of wound closure without increasing complication rates in patients with NSTI compared with traditional NPWT or moist wound care dressing. Although prospective studies are needed, this indicates the potential to improve patient quality of life through reduced pain and outpatient home health needs.
Necrotizing soft tissue infection (NSTI) is a severe, rapidly progressive skin and soft tissue infection associated with tissue necrosis, sepsis, and multisystem organ failure. Necrotizing soft tissue infections encompasses previous terminology that grouped infections by location (perineum, Fournier gangrene; submandibular space, Ludwig's angina) and depth of tissue invasion (necrotizing fasciitis versus myonecrosis). Necrotizing soft tissue infections can be defined further by the causative organisms: group 1 (polymicrobial with gram-positive cocci, gram-negative rods, and anaerobes); group 2 (monomicrobial typically with group A streptococcus but methicillin-resistant Staphylococcus aureus [MRSA] has also been isolated); group 3 (gram-negative marine organisms, such as Vibrio vulnificus), and group 4 (fungal).1–3
Necrotizing soft tissue infections are overall rare but devastating. The incidence in the United States ranges from 3,800 to 5,800 admissions per year. 4 Mortality in the literature ranges from 11% to 40%.5–8 Predisposing factors for NSTI include diabetes mellitus, obesity, smoking, intravenous drug use, immunosuppression, and peripheral vascular disease.7,9 Nonetheless, NSTI, particularly group 2 NSTI, is still seen among young and healthy individuals. 2 The first line of therapy for NSTI is broad-spectrum antibiotic agents, surgical debridement, and physiologic resuscitation. 10 However, after debridement, there are widely varying practices for the management of these frequently large open wounds. Current practice varies from moist wound care dressing to negative pressure wound therapy (NPWT) with or without instillation.
Negative pressure wound therapy functions to improve wound healing through four different mechanisms: reduction of tissue edema, reduction of bacterial burden, increased granulation tissue and blood vessel formation due to mechanical stress, and a reduction in wound tension. 11 With the addition of negative pressure wound therapy with instillation (NPWTi), the ability to irrigate the wound with topical solution at regular intervals allows for decreased viscosity of wound exudate and decreased biofilm formation.12,13
We hypothesized that the use of NPWTi results in a higher wound closure rate after debridement of NSTI compared with traditional NPWT or wet to dry dressings (moist wound care dressing).
Patients and Methods
After obtaining Institutional Review Board approval, the prospectively maintained Acute and Critical Care Surgery database of one academic hospital spanning 2008 to 2018 was queried for patients with a diagnosis of necrotizing fasciitis, Fournier gangrene, or gas gangrene using both International Classification of Diseases (ICD)-9 and ICD-10 codes. Patients who did not undergo an operation were excluded.
From the registry, demographic data, pre-existing conditions, laboratory data, microbiologic data, and hospital outcomes were extracted. We calculated the number of ICU-free days as 30 minus the number of ICU days (ranging from 0 to 30 days), and we deducted 0 ICU-free days for patients who died within 30 days in the ICU.
Laboratory data including white blood cell (WBC) count, hemoglobin, sodium, creatinine, blood glucose, and albumin at the time of presentation to our medical center were collected. C-reactive protein levels were only obtained in a minority of patients (24); 6.5% of them were not included in the analysis. Operative data, encompassing wound measurements, closure method, utilization of NPWT, the number of operations involving dressing changes or NPWT application, and the count of debridement procedures, were manually extracted from operative reports as distinct variables.
Tissue loss was defined as the difference between the wound size at the end of the final operative debridement from the wound size at the end of the initial debridement. Because of variability in measurements, some wounds demonstrated negative tissue loss (or tissue gain) across debridements and were reported as zero for the purpose of calculations. Complications were defined as surgical site infections (SSI) and re-admission because of wound complications within 100 days.
Patients were stratified into three groups based on a review of operative reports. Patients in the moist wound care dressing group never had NPWT. Some patients received both NPWT and NPWTi throughout the course of their treatment; these patients were analyzed in the NPWTi group. The primary outcome measure was wound closure, classified as open, partially closed, or completely closed based on operative dictation.
Data were analyzed using SPSS (IBM Corp, Armonk, NY). Univariable analysis was performed using analysis of variance (ANOVA) and Pearson χ 2 . Categorical results are reported as percentages and absolute values and continuous variables as mean and interquartile ranges. A p value of less than 0.05 was considered statistically significant. Multivariable logistic regression models were used to estimate the effect of the use of NPWTi on wound closure at discharge and mortality.
Results
Demographic data, comorbidities, and clinical characteristics
In total, 371 patients met inclusion criteria; 173 were managed with moist wound care dressing, 150 were managed with NPWT, and 48 were managed with NPWTi. The groups were similar in terms of age, race, and gender distribution (Table 1). Rates of diabetes mellitus, smoking, and peripheral vascular disease did not vary substantially. Intravenous drug use was more common in the NPWTi group (20.8% vs. 6.7% in the NPWT group and only 4% in the moist wound care dressing group). Distribution of NSTI locations differed somewhat according to treatment group. With NPWT and NPWTi use, a perineal location was less common, but an extremity location was more common, although this did not reach statistical significance.
Patient Characteristics
NPWT = negative pressure wound therapy; NPWTi = negative pressure wound therapy with instillation; SD = standard deviation; PMH = past medical history; DM = diabetes mellitus; IVDU = intravenous drug use; PVD = peripheral vascular disease; qSOFA = Quick Sequential Organ Failure Assessment.
Of six cases of head or neck wounds, 67% were treated with moist wound care dressing, and 33% with NPWT, with none using NPWTi. For chest or upper back wounds, 28 cases were noted, with 29% treated with moist dressings, 57% with NPWT, and 14% with NPWTi. In the abdomen or flank region, there were 73 cases, with treatments divided into 37% moist dressings, 52% NPWT, and 11% NPWTi. The groin, perineum, or buttocks area had 167 cases, with a treatment distribution of 57% for moist dressings, 31% for NPWT, and 12% for NPWTi. Upper extremity wounds, totaling 36 cases, were treated with 28% moist dressings, 53% NPWT, and 19% NPWTi. Last, the lower extremity had 153 cases with 44% receiving moist dressings, 41% NPWT, and 15% NPWTi.
Laboratory and microbiology data
There were no differences in the WBC count, serum sodium, creatinine, or blood glucose values at the time of admission among the groups (Table 2). Operative cultures were performed in patients; 111 were polymicrobial, 124 were monomicrobial, and 99 had no growth. The most common pathogens in monomicrobial samples were Staphylococcus aureus (18.%), Group F streptococcus (15.3%), and Bacteroides fragilis (10.5%; Table 5). Among polymicrobial samples, the most common pathogens isolated were Escherichia coli (23.4%), Group F streptococcus (10.8%), and Staphylococcus aureus (10.8%; Table 6).
Laboratory Data
NPWT = negative pressure wound therapy; NPWTi = negative pressure wound therapy with instillation; WBC = white blood cell.
Negative pressure wound therapy with instillation resulted in full wound closure in 50% of patients, compared with only 23.3% of those who received NPWT and 15% of those who used moist wound care dressing. The median debridement showed that the original wound size was largely constant across all groups. The NPWTi group, however, showed noticeably less tissue loss (Table 3).
Clinical Outcomes
NPWT = negative pressure wound therapy; NPWTi = negative pressure wound therapy with instillation; POD = post-operative day; LOS = length of stay; SD = standard deviation; ICU = intensive care unit.
Multivariable regression analysis showed that NPWTi was linked to closure rates that were roughly five times higher than those seen in the NPWT group after adjusting for variables like smoking status, intravenous drug use (IVDU), the number of procedures, and the body location most frequently affected by the condition (odds ratio [OR], 5.28; 95% confidence interval [CI], 2.40–11.61; p = 0.001). After controlling for variables including body location most frequently affected by the condition and wound closure at discharge, moist wound care dressing was associated with mortality that was approximately two times higher than that observed in the NPWT group (OR, = 2.12; 95% CI, 1.08–4.17; p = 0.02) (Table 4). Wound closure at discharge was also increased with the increase in the use of NPWTi over the last few years (Figs. 1 and 2).
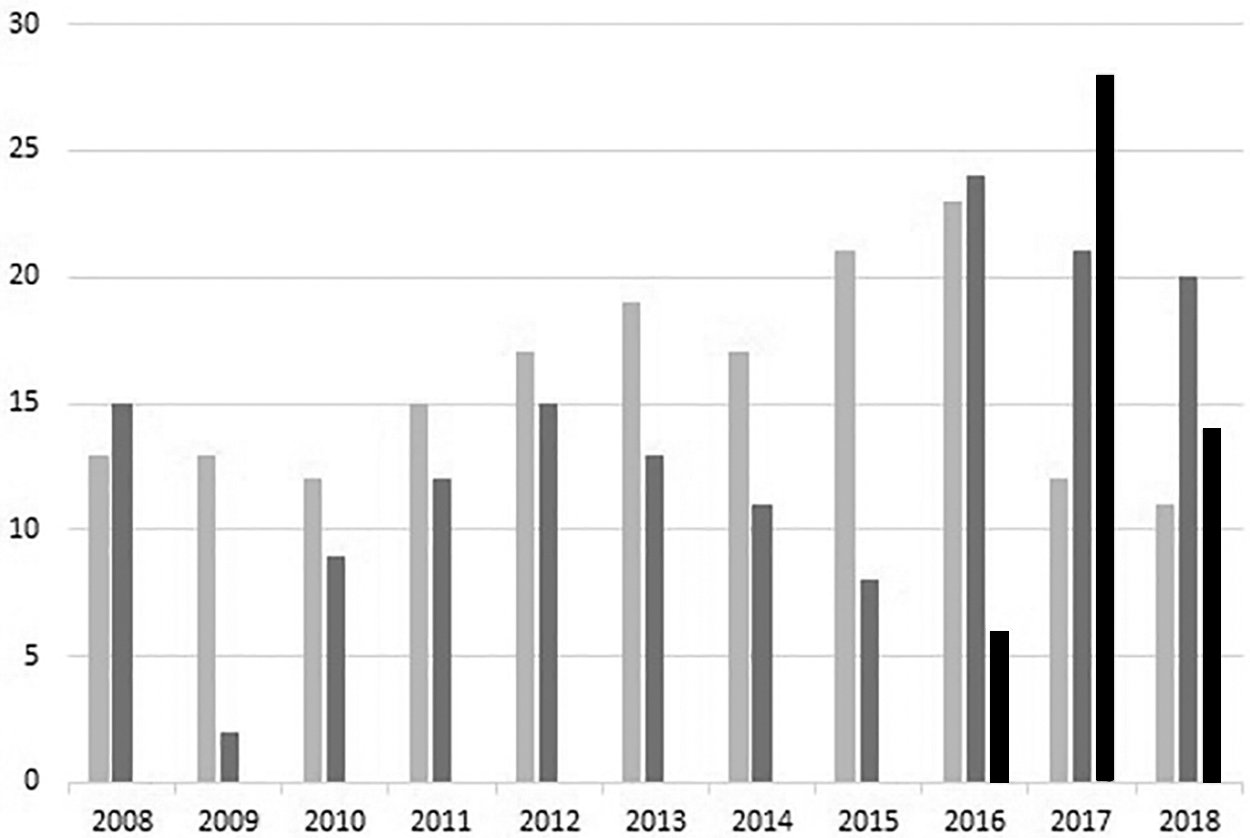
Therapy used over the time. Light gray: Percentage of patients who had moist wound care dressing. Dark gray: Percentage of patients who had negative pressure wound therapy (NPWT). Black: Percentage of patients who had negative pressure wound therapy with instillation (NPWTi). x-axis: Time (years). y-axis: Number of patients.
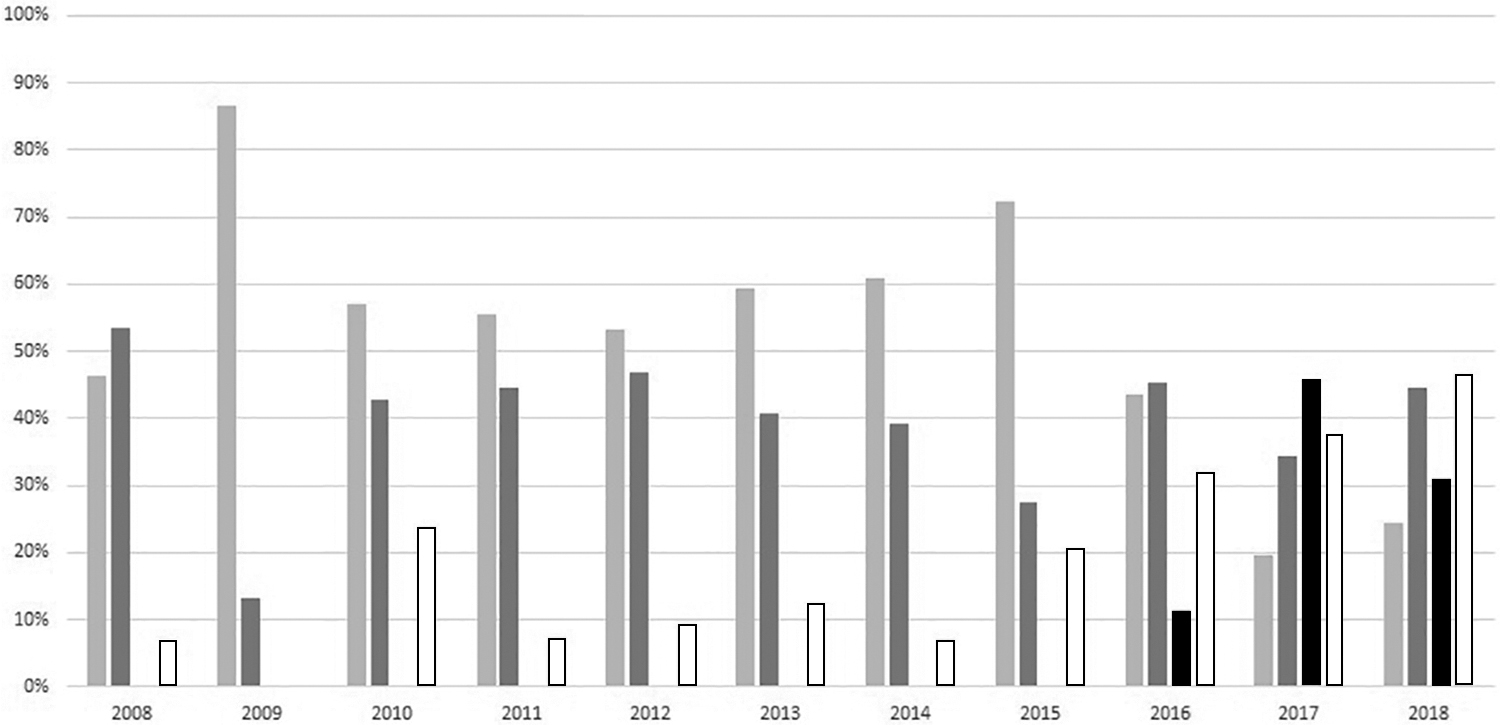
Status of wound closure at discharge over the time. Light gray: percentage of patients who had moist wound care dressing. Dark gray: Percentage of patients who had negative pressure wound therapy (NPWT). Black: Percentage of patients had who negative pressure wound therapy with instillation (NPWTi). White: Percentage of patients discharged with complete wound closure x-axis: Time (years). y-axis: Percentage of patients.
Logistic Regression
OR = odds ratio; CI = confidence interval; NPWT = negative pressure wound therapy; NPWTi = negative pressure wound therapy with instillation; IVDU = intravenous drug use.
Most Common Pathogens in Monomicrobial Samples
MRSA = methicillin-resistant Staphylococcus aureus.
Most Common Pathogens in Polymicrobial Samples
The results also showed notable differences in the course of treatment for individuals with NSTIs affecting the extremities. The amputation rate was 6.7% lower in the NPWTi group and 17.9% higher in the group using moist wound care dressing. The Quick Sequential Organ Failure Assessment (qSOFA) score was used to determine the severity of the sickness, and it revealed only minor variations between the therapy groups (Table 3). The intensive care unit (ICU)-free days are not different among the treatment groups. The mortality rate was considerably greater in the moist wound care dressing group (16.2% vs. 10.7% in the NPWT group vs. 2.1% in the NPWTi group; p = 0.02), even though the overall rates of complications at 100 days were not different (Table 3).
Discussion
In this retrospective study of the management of open wounds after debridement of NSTI, we demonstrated an association between NPWTi and increased wound closure at the time of hospital discharge. Additionally, patients with NSTI who received NPWTi were less likely to die or need an amputation. Tissue loss was lower in NPWTi patients, but the clinical significance of this improvement may be compromised by the inconsistency observed in wound measurement documentation. As a result, it is essential to undertake further comprehensive prospective studies to confirm and validate these findings. Future studies should be prospective and with standardized wound measurements between providers and returns to the OR and should include photographic measurement/documentation. Although NPWTi appears to have a positive effect on wound closure at discharge and a lower number of days in the ICU, they received more operations than those patients who did not receive negative pressure wound therapy.
Although there have been no prior studies specifically examining the effect of NPWTi on NSTI, Gabriel et al. 13 showed a decreased time to infection clearance in wounds treated with NPWTi compared with wounds managed with moist wound care dressing in a study of 30 patients with complex infected wounds, including three cases of necrotizing fasciitis. Negative pressure wound therapy with instillation has been shown to decrease bioburden more effectively than NPWT alone after debridement in chronically infected wounds. 14 Furthermore, NPWTi produces more robust granulation tissue and reduction of wound size than NPWT alone. 15 Prior studies have shown that NPWTi has the potential to decrease healing time, both through reduction of bioburden, which inhibits healing, and solubilization of exudate.16–18 Although final healing time was not documented in this retrospective study, the higher proportion of closure at discharge suggests improved wound contracture and healing among the NPWTi group.
Negative pressure wound therapy with instillation has been used effectively as a salvage therapy in patients with infected orthopedic implants, and there are case reports of its use to salvage limbs in cases of severe necrotizing fasciitis. 19 Negative pressure wound therapy with instillation does not replace the need for serial debridements, as evidenced by the higher number of operations in the NPWT and NPWTi groups; however, it could potentially lead to a reduction in tissue loss. Although we were unable to clearly demonstrate this through a review of operative measurements, the association between NPWTi and lower rates of amputation in the NSTI of the extremities suggests less tissue loss, potentially allowing for limb salvage. Higher rates of wound closure at discharge also indicate less need for outpatient wound care and improved patient quality of life, as open wounds are typically managed with twice-daily dressing changes and have been reported to decrease independence and mobility and increase depression in patients. 20
Limitations
Because this was a retrospective study, it was impossible to determine the reasoning behind the choice of NPWT, NPWTi, or moist wound care dressing from the medical record. As such, it is unclear if the associations between NPWTi and outcome have more to do with the types of patients in which NPWTi was used or with the therapy itself. Furthermore, data on complications were obtained via medical record review and likely represent an underestimate of actual rates, as patients could present to outside institutions with complications not captured by our hospital's medical records.
Our study is limited in its ability to retrospectively gather data points regarding the presence of technical issues and the specifics of conventional NPWT applications. These details, such as the duration of therapy and potential technical problems, could shed light on the challenges and outcomes associated with both treatments. It is important to acknowledge that NPWT therapy itself is known to present various technical complexities, and it is reasonable to anticipate that these challenges may not have been lessened in our study. Moreover, comprehensive insights into the use of conventional NPWT, including the materials used and the level of negative pressure applied, could have further enriched our analysis but were not attainable within the scope of our study's retrospective design. It was also challenging to analyze the results of wounds based on the regions of the wounds because of the complexity of the wounds, which overlapped multiple body parts, and due to the retrospective nature of the study.
Conclusions
Negative pressure wound therapy with instillation appears to be a promising adjunct to wide local excision in the management of NSTI, associated with increased wound closure without an increase in complication rate. However, a longer hospital stay and more debridements could outweigh the potential cost savings from decreased wound care needs at follow-up. Further prospective evaluations are needed to determine if NPWTi contributes to decreased tissue loss, mortality, and amputation rates in patients with NSTI.
Footnotes
Authors' Contributions
Data curation: Afzal, Dawson, Fonseca, Canas, Diaz, Di Filippis. Formal analysis: Afzal, Dawson. Investigation: Afzal, Dawson, Fonseca, Canas, Diaz, Di Filippis. Writing—original draft: Afzal, Dawson. Writing—review and editing: Afzal, Mazuski. Visualization: Afzal, G.V. Bochicchio. Project administration: K. Bochicchio. Supervision: K. Bochicchio, G.V. Bochicchio. Conceptualization: G.V. Bochicchio. Validation: G.V. Bochicchio.
Funding Information
The authors have no funding to report.
Author Disclosure Statement
The authors have no conflict of interest to report.