
Abstract

To the Editor:
T
We present the case of a 43-year-old male patient who was admitted with a four-day history of abdominal discomfort and fever, with a maximum temperature of 39.5°C. He had previously received antibiotic treatment at a local hospital without improvement. The patient was admitted to our hospital for further evaluation and treatment.
Ultrasound examination revealed a heterogeneous echogenic mass measuring 6.6 × 4.2 cm in the left lobe of the liver, suggestive of a liver abscess. Adjacent to the heterogeneous echogenic mass, an abnormally echogenic area measuring approximately 2.8 cm in length was observed (Fig. 1). Abdominal computed tomography (CT) imaging demonstrated a mixed-density lesion in the left lateral segment of the liver, measuring approximately 6.0 × 3.5 cm, with ill-defined borders, indicative of an infectious lesion. Additionally, a linear, high-density shadow measuring approximately 2.5 cm in length was observed in the left lateral segment of the liver (Fig. 2). Based on our assessment, we strongly suspected a fish bone as the cause, even though the patient could not recall swallowing a fish bone. After discussion, the patient underwent surgical intervention.

Ultrasound examination of the abdomen. Fish bone in the liver (black dashed line).
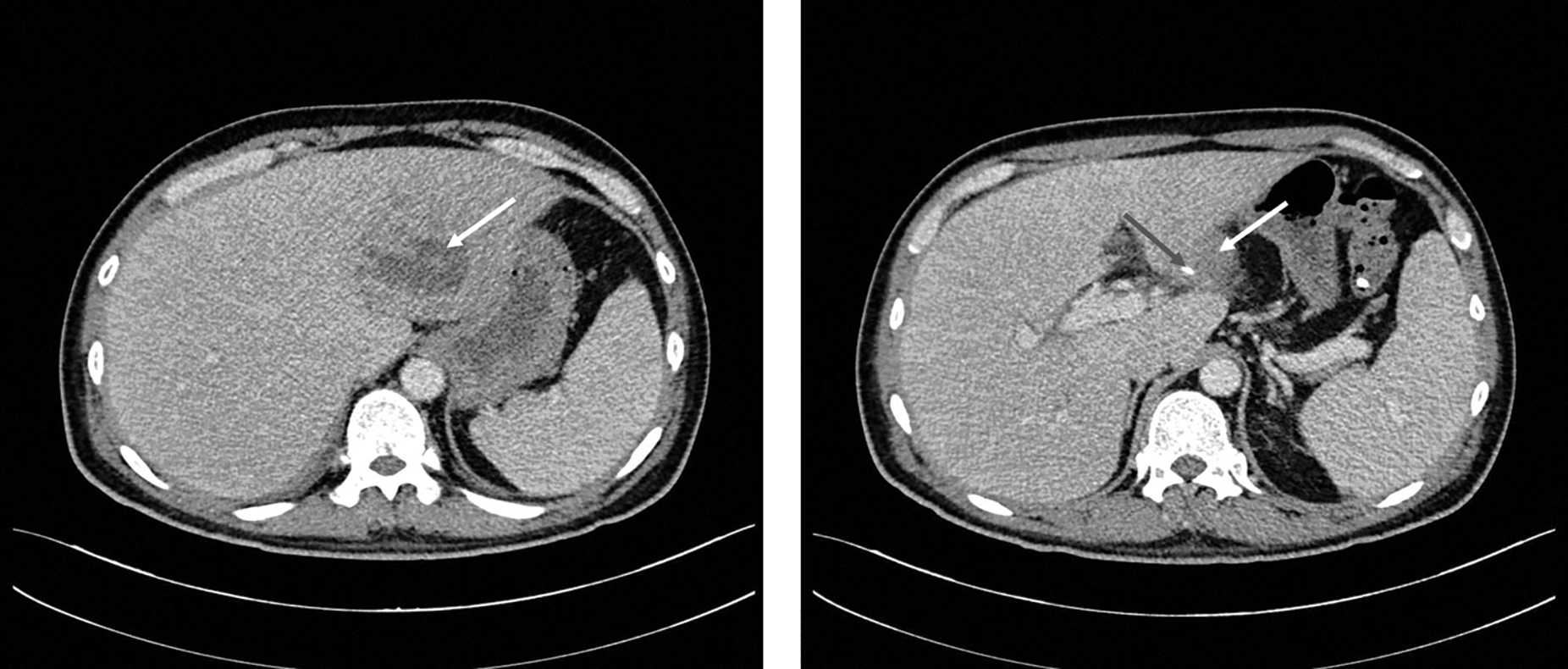
Computed tomography (CT) examination of the abdomen. A mixed-density and ill-defined borders lesion (blue arrow) and high-density shadow measuring approximately 2.5 cm in the left hepatic lobe (white arrow).
Intraoperatively, we found adhesions between the anterior wall of the gastric antrum and the left lobe of the liver, creating a sinus tract. We identified a fish bone approximately 3 cm in length in the left lobe of the liver (Fig. 3). The surface of the left lobe of the liver exhibited localized elevation, measuring approximately 5 cm in size. We performed a left hepatic lobectomy with foreign body removal and repaired the gastric wall. The patient had an uneventful recovery and did not experience any complications.

Surgical specimen. A fish bone measuring approximately 2.5 cm was removed during the operation.
It is noteworthy that only 12% of patients can recall ingesting foreign objects.2,3 Moreover, even in cases in which a diagnosis of foreign body ingestion is established, most patients do not remember swallowing a fish bone. This lack of patient recollection poses a diagnostic challenge. Liver abscesses resulting from the migration of fish bones rarely present with typical liver abscess symptoms, such as fever, upper abdominal pain, and jaundice. Foreign objects may remain within the body for extended periods without any clinical symptoms until the development of infection or abscess formation. Diagnostic methods primarily include CT, color Doppler ultrasound, and endoscopic examinations. Computed tomography offers superior sensitivity to ultrasound for diagnosing liver abscesses and provides more precise localization. Because foreign bodies lodged within the liver cannot be naturally expelled from the body, providing antibiotic treatment can only alleviate symptoms. Therefore, early diagnosis is crucial.
In clinical practice, when encountering bone-like high-density shadows accompanied by inflammation or abscess formation in tissue organs outside the abdominal gastrointestinal tract or within the abdominal fat interspace, the possibility of a fish bone should be considered. Treatment of liver abscesses induced by fish bone migration involves prompt and appropriate antibiotic therapy and surgical removal of the foreign body. For larger-diameter abscesses, continuous catheter drainage or partial hepatectomy may be contemplated. In cases with extended medical histories, gastroscopy may not necessarily yield positive results. In such instances, the heightened sensitivity of CT to the presence of fish bones aids in making a rational diagnosis and treatment plan for patients.