
Abstract
Background:
Imaging plays an essential role in the management of hepatic hydatid cysts (HCE). The objective of our study was to determine the correlation between pre-operative ultrasound, computed tomography (CT), and intra-operative ultrasound (IOUS) in studying the characteristics and complications of HCE.
Patients and Methods:
This was a prospective, descriptive, and analytical study conducted in the General Surgery Department of Habib Bourguiba Hospital in Sfax. The study included patients with HCE who underwent conservative surgery between April 2017 and June 2022.
Results:
We enrolled 49 patients with 94 cysts. At the end of our study, IOUS allowed for better detection of HCE (98.8%) regardless of the number of cysts per patient. IOUS and CT were accurate in studying the location of cysts (κ = 1), whereas pre-operative abdominal ultrasound was less efficient (κ = 0.870). IOUS was the best examination for detecting exocysts (κ = 0.961), studying daughter cysts (κ = 0.823), and exploring vascular relations, but it was less effective (κ = 0.523) in detecting calcifications. Regarding classifications, ultrasound and CT had similar results. However, IOUS was most reliable in differentiating between CE3b and CE4 types (κ = 0.653). Ultrasound, CT, and IOUS were not sensitive in detecting latent HCE suppurations and cystobiliary fistulas.
Conclusions:
Performing IOUS is essential to prevent recurrences and reduce post-operative morbidity.
In recent years, substantial progress has been made in the diagnosis and treatment of hepatic cystic echinococcosis (HCE). Current imaging techniques, especially pre-operative abdominal ultrasound and computed tomography (CT), allow for the diagnosis of HCE. However, their effectiveness in examining the peri-cyst and identifying complications related to HCE is still limited. 1 Cavity-related complications after conservative surgery could be as a result of occult biliary fistula that often go amiss and untreated on pre-operative imaging.2–4 In addition, cyst recurrence could be a result of a missed cyst or exocysts undetected during surgery. 5 Our objective is to assess the significance and contribution of intra-operative ultrasound (IOUS) by studying the correlation between IOUS and pre-operative imaging.
Patients and Methods
Study design and setting
We conducted a prospective descriptive and analytical study involving patients undergoing surgery for HCE at the General Surgery Department of Habib Bourguiba University Hospital in Sfax from April 2017 to June 2022. All the cysts were limited to the liver. The aim of this study was to determine the correlation between ultrasound, CT scans, and IOUS in studying the characteristics and complications of HCE.
Study participants
We included all cases of HCE observed in patients who provided their written informed consent and underwent elective or emergency surgery. All patients underwent a conservative therapeutic approach, initiating with the aspiration of cystic contents through puncture, followed by the meticulous extraction of the hydatid membrane. This procedural sequence is executed with precision to preclude any inadvertent inoculation into the peritoneal cavity. Subsequently, a resection of the protruding dome is conducted, encompassing the excision of the peri-cyst cap projecting on the hepatic surface. Patients operated on as emergencies because of septic or anaphylactic shock and those with contraindications for contrast-enhanced CT scans were excluded.
Study design
All patients underwent pre-operative abdominal ultrasound and CT scans, cholecystectomy, IOUS, and methylene blue test (MBT) through the transcystic drain for intra-operative exploration. Abdominal ultrasound was performed using a Samsung (Samsung Healthcare, South Korea) ultrasound machine with a convex probe emitting ultrasound waves at a frequency of 3-5 MHz to allow deep penetration of HCE and hepatic tissue. Abdominal CT scans were conducted using a Siemens 64-slice scanner (Siemens Healthineers AG, Germany) without and with contrast injection, followed by multiplanar reconstruction. Scans were acquired during arterial, portal, and delayed phases. For IOUS, a Samsung ultrasound machine with a convex probe and a linear probe emitting ultrasound waves at 4 MHz were used for a more detailed exploration of cyst walls and their vascular and biliary relationships.
Using these imaging modalities, parameters such as the number of cysts, the location of the cyst within the liver, details about the peri-cyst, and the cyst contents and the presence of complications of the cysts were recorded. The complications include a cystobiliary fistula (CBF), intra-peritoneal rupture, and cyst suppuration as well as compression of blood vessels and biliary ducts within the liver. These compressions range from total stenosis of the hepatic or portal veins by the cyst to appearing laminated on the imaging studies. Patency of these veins were verified using color Doppler imaging.
Data analysis
The unit of study is the cyst. Data were entered and processed using SPSS Statistics, version 25 (IBM Corp, Armonk, NY). Quantitative variables were described using means and standard deviations after testing for normality. Qualitative variables were described using proportions. Associations between variables were analyzed using hypothesis tests. Concordance analysis of matched qualitative variables was performed using the κ coefficient with a significance threshold set at 5%. The strength of association was assessed using the κ value:
0.8 < κ ≤ 1: strong association 0.5 < κ ≤ 0.8: moderate association 0.2 < κ ≤ 0.5: weak association 0 ≤ κ ≤ 0.2: negligible or no association
Pearson or Spearman correlation coefficients (r) were used to measure the association between two quantitative variables. The strength of association was assessed using the r value:
0.8 < r ≤ 1: strong association
0.5 < r ≤ 0.8: moderate association
0.2 < r ≤ 0.5: weak association
0 ≤ r ≤ 0.2: negligible or no association
Sensitivity, specificity, their respective confidence intervals, and negative predictive value were calculated using Excel statistical software (Microsoft, Redmond, WA).
Informed patient consent
Prior to the start of our study, approval was obtained from the local ethics committee (Comité de Protection des Personnes adapté à l'Expérimentation Médicale ou Scientifique des Produits Médicaux destinés à la Médecine Humaine), under reference CPP sud numéro 0021/2017. This committee is the sole medical or scientific research center for human medicine in our institution, the University of Sfax. It is approved by the Ministry of Public Health. All patients who participated in our prospective study signed a written consent form.
Results
Descriptive study
A total of 49 patients with 94 HCE cases were included in our study. The average age of our patients was 46 ± 18 years, with a predominance of females (65%). Pain was the primary symptom. The most common finding during physical examination was tenderness upon palpation of the right hypochondrium. In terms of laboratory tests, 18 patients (37%) showed abnormal liver function tests, and 13 patients (27%) exhibited leucocytosis. Positive hydatid serology was observed in 41 patients (84%).
Pre-operative ultrasound data
Abdominal ultrasound detected 80 HCE cases (85%). Among these, 26 cases (32.5%) involved a single cyst. Of these cysts, 26.9% were located in the left lobe and 73.1% in the right lobe, with 55.1% at the hepatic dome. Daughter vesicles were observed in 27 cysts (28.7%). Parietal calcification was noted in 6 cases (7.5%). Exocysts were observed in five cysts (6.2%). According to the Gharbi classification, 25 cysts were type 3 (31.2%). According to the World Health Organization (WHO) classification, 21 cysts (26.2%) were type CE1, 21 cysts (26.2%) were type CE2, and 20 cysts were type CE3a (25%). Three cases of intraperitoneal rupture were suspected. Cystobiliary fistula was suspected in five cysts (6.2%). This fistula was directly visible in one case (1.2%) and inferred from indirect signs in four cysts. Vascular compression was observed in 26 cysts (32.5%).
Computed tomography findings
Computed tomography scans revealed 94 cysts. Among these, 27 patients (28.7%) had a single cyst. Daughter vesicles were observed in 34 cases (36.1%). Parietal calcification was observed in 16 cases (17%). Exocysts was noted in 12 cysts (12.7%).
According to the Gharbi classification, the cysts were type 1 in 30 cases (34.4%) and type 3 in 32 cases (34%). According to the WHO classification, the cysts were type CE1 in 30 cases (31.9%) and CE2 in 22 cases (23.4%). Suppuration was suspected in only one cyst (1%). Cystobiliary fistula was suspected seven times on CT scans (7.4%). Vascular compression was observed in 41 cysts (43.6%).
Intra-operative ultrasound (IOUS) findings
Intra-operative ultrasound detected 94 cysts. Among these, 28 patients (29.7%) had a single cyst. Of these cysts, 25.5% were located in the left lobe, 74.5% in the right lobe, and 48.9% at the hepatic dome. Daughter vesicles were observed in 37 cysts (39.3%). Parietal calcification was noted in 25 cysts (26.5%), exocysts were detected in 15 cysts (15.9%).
According to the Gharbi classification, the cysts were type 3 in 35 cases (37.2%). Regarding the WHO classification, 20 cysts (21.2%) were type CE1, 22 cysts (23.4%) were type CE2, and 20 cysts (21.2%) were type CE3a. Suppuration was observed in only one cyst (1%). Cystobiliary fistula was suspected in 21 cysts (22.3%). Vascular compression was detected in 53 cysts (56.3%).
Intra-operative characteristics of cysts
Cysts were solitary in 27 cases and multiple in 22 patients. Cysts were found in both lobes of the liver in 15 patients (30,6%). Among these cysts, 28 cysts (30%) were located in the left lobe, and 66 (70%) were in the right lobe. Regarding the peri-cyst, parietal calcification was noted in 14 cases (14.9%; Table 1). Upon exploration of cyst contents, a clear water-like content was observed in 65 cysts (69.1%). Daughter vesicles were noted in 39 cysts (41.5%). A mastic, biliary, or purulent content was found in 40 cysts (42.6%). Exocysts were noted in 16 cysts (17%; Table 1).
Characteristics of Cysts According to Intra-Operative Findings
Characteristics of Cysts According to Intra-Operative Findings
WHO = World Health Organization; CBF = cystobiliary fistula; CBD = common bile duct.
According to the Gharbi classification, cysts were type 2 in 24 cases (25.5%) and type 1 in 15 cases (16%). Types were almost evenly distributed according to the WHO classification (Table 1). Suppuration was observed in four cysts (4.3%) of cases. No cases of thoracic fistulization or intraperitoneal rupture were observed. Cystobiliary fistula was found in 18 cysts (19.1%), including one cyst (1%) with large fistulas (>5 mm). In total, 48 fistulas were detected intra-operatively with an average of 2.35 fistulas per cyst complicated with CBF (Table 1). No cases of angiocholitic abscess were observed, and hydatid material in the common bile duct was seen in only one patient with a single cyst (1%; Table 1).
Of the 94 cysts that were considered for this study, six developed an external bile fistula, which was managed conservatively with antibiotic agents. Recourse to endoscopic sphincterotomy was not required and the fistula resolved spontaneously. The overall morbidity was 12,8% and we report no post-operative mortality in our participants. After a median follow-up of 32 months, no recurrence was detected in the participants of this study.
Analytical study
Correlations between abdominal ultrasound and surgical findings
Abdominal ultrasound enabled the detection of 80 cysts (85%) with a strong correlation (mean of 1.81 vs. 1.94; r = 0.891; p < 0.001). Ultrasound detected all single cysts. It identified 82% of multiple cysts (≥2) with a correlation coefficient of 0.74.
Abdominal ultrasound showed excellent agreement with intra-operative data regarding cyst location (κ = 0.870; p < 0.001; Table 2). The observations from abdominal ultrasound were weakly consistent with intra-operative findings concerning parietal calcifications (κ = 0.412) and the detection of exocysts (κ = 0.447; Table 2). Abdominal ultrasound observations were moderately consistent with intra-operative findings regarding the visualization of daughter cyts (κ = 0.731) and the WHO classification (κ = 0.609; Table 2). Abdominal ultrasound findings were not consistent with intra-operative findings regarding cyst suppuration (κ = 0) and the detection of CBFs (κ = 0.005; Table 2). Regarding the detection of hydatid material in the common bile duct, abdominal ultrasound observations strongly correlated with intra-operative exploration, detecting hydatid material in the bile duct in 100% of cases (Table 2).
Concordance of Abdominal Ultrasound With Intra-Operative Findings in Studying Cyst Characteristics
WHO = World Health Organization; CBF = cystobiliary fistula.
In summary, abdominal ultrasound was not reliable in detecting HCE. In the study of the peri-cyst, particularly concerning the detection of calcifications and exocysts, abdominal ultrasound was not reliable. Despite its moderate agreement in defining the WHO cyst types, it was not accurate in distinguishing between CE3b and CE4 types. Similarly, abdominal ultrasound was not reliable in detecting latent suppurations of HCE, biliary-cyst fistulas (BCFs), and hydatid material in the common bile duct.
Correlations between abdominal ct scan and surgical findings
Abdominal CT scans enabled the detection of most cysts with an excellent correlation (average: 1.92 vs. 1.94; r = 0.996; p < 0.001). Computed tomography scans demonstrated excellent agreement in defining the location of the cysts (Table 3). Computed tomography scan observations strongly correlated with intra-operative findings regarding the detection of exocysts (κ = 0.831; Table 3). Moreover, abdominal CT were moderately consistent with intra-operative findings concerning parietal calcifications (κ = 0.629), the detection of daughter vesicles (κ = 0.788), and the WHO classification (κ = 0.613; Table 3). The observations from abdominal CT scans were not consistent with intra-operative findings regarding cyst suppuration (κ = −0.017) and the detection of CBFs (κ = 0.051). In terms of detecting hydatid material in the main bile duct, CT scan findings strongly correlated with intra-operative exploration, detecting all HCE cases associated with hydatid material in the common bile duct.
Concordance of Abdominal CT Scans With Intra-Operative Findings in Studying Cyst Characteristics
CT = computed tomography; WHO = World Health Organization; CBF = cystobiliary fistula; CBD = common bile duct.
In summary, abdominal CT scans showed excellent agreement in counting HCE cases and exhibited strong agreement in detecting exocysts. However, they had moderate agreement in detecting calcifications. Despite its good reliability in defining the WHO classification of HCE, CT scans had low agreement in differentiating between CE3b and CE4 types albeit without statistical significance. Computed tomography scans were not reliable in detecting latent suppurations of HCE and CBFs.
Correlations between IOUS and surgical findings
Intra-operative ultrasound enabled the detection of all cysts with excellent correlation (average, 1.94 vs. 1.94; r = 1; p < 0.001). Intra-operative ultrasound demonstrated excellent agreement in defining the location of the cysts (Table 4). Intra-operative ultrasound observations strongly correlated with intra-operative findings regarding the detection of exocysts (κ = 0.961), the detection of daughter vesicles (κ = 0.823), the detection of hydatid material (κ = 1), and the WHO classification (κ = 0.865; Table 4). Intra-operative ultrasound observations moderately correlated with intra-operative findings concerning parietal calcifications (κ = 0.523; Table 4). Intra-operative ultrasound observations were not consistent with intra-operative findings regarding the detection of CBFs (κ = 0.316; Table 4).
Concordance of IOUS With Intra-Operative Findings in Studying Cyst Characteristics
IOUS = intra-operative ultrasound; CBF = cystobiliary fistula; CBD = common bile duct.
In summary, IOUS exhibited excellent concordance in studying the number, location, and peri-cyst of the cysts. Intra-operative ultrasound demonstrated strong agreement in defining the WHO types of HCE (κ = 0.865) and moderate agreement in differentiating between CE3b and CE4 types (κ = 0.635); however, it was not reliable in detecting CBFs.
Comparison of correlations
Computed tomography scans and IOUS were superior to abdominal ultrasound in counting the cysts. Intra-operative ultrasound allowed for a better detection of all HCE regardless of the number of cysts per patient. Both IOUS and CT scans were accurate in studying the cysts' localization with a κ = 1, whereas pre-operative abdominal ultrasound was less efficient (κ = 0.870).
Intra-operative ultrasound excelled in detecting exocysts but was less reliable in identifying calcifications (Table 5). It outperformed in studying daughter vesicles. In terms of classifications, ultrasound and CT scans showed similar results. However, IOUS was superior in this regard because of its ability to detect daughter vesicles. Therefore, IOUS was the best at differentiating between CE3b and CE4 types compared to CT scans and abdominal ultrasound (Fig. 1 and Table 5).

Comparison of k coefficients of the different imaging modalities to the intra-operative findings.
Correlations Between Abdominal Ultrasound, CT Scans, and IOUS in Studying Cyst Wall, Daughter Vesicles, and Classifications
CT = computed tomography; IOUS = intra-operative ultrasound; CBF = cystobiliary fistula.
Denotes statistically significant p values.
In the absence of suggestive clinical and biologic signs, ultrasound, CT scans, and IOUS were not sensitive in detecting latent suppurations of HCE (Fig. 1). Regarding the detection of CBFs, ultrasound, CT scans, and IOUS were not effective (Fig. 1). Abdominal ultrasound and CT scans had low sensitivities to classify CE3b and C4 cysts pre-operatively but have high specificities (Figs. 2 and 3).
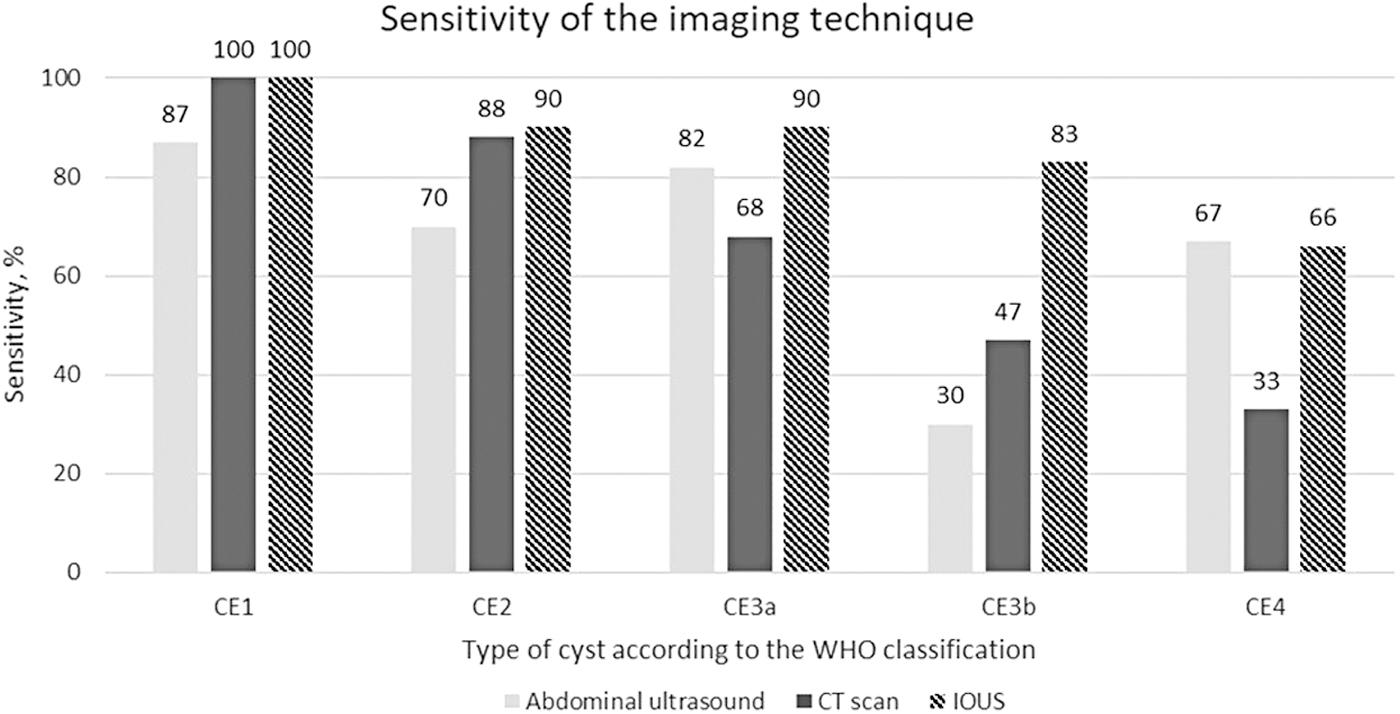
Sensitivity of different imaging techniques to classify the cysts.

Specificity of different imaging techniques to classify the cysts.
Discussion
Management of hydatid disease is multidisciplinary, requiring essential collaboration between radiologists and surgeons. Conservative treatment, although widely used, carries a risk of recurrence and morbidity. To prevent these problems, we studied the correlation between pre-operative ultrasound, abdominal CT scans, and IOUS to demonstrate the importance of IOUS in morphologic and topographical analysis of cysts, the identification of daughter cysts (a major source of post-operative recurrence), and in detecting CBFs.
Based on our statistical study, we observed the following:
In cyst counting, CT scans and IOUS outperformed abdominal ultrasound. For peri-cyst evaluation, IOUS was more reliable compared with CT scans, especially in detecting exocysts, a major source of post-operative recurrence; however, IOUS was less effective in identifying calcifications and the laminated layer. These results could be explained by the optimal sensitivity of IOUS in detecting small hepatic lesions compared to other pre-operative imaging methods, such as subcentimeter hepatic metastases. 6 Thus, IOUS could enhance post-operative outcomes by better detecting exocyts.
In detecting vascular relationships of hepatic hydatid cysts, IOUS was the most effective. This technique is highly sensitive in detecting vascular relations of hepatic tumors compared with pre-operative imaging and can tailor the surgical management of these lesions.6,7 Hence, the relevance of IOUS in treating cysts located at the hepatic hilum and dome.
Given its superior performance in peri-cyst evaluation, especially in exocyst detection, and in studying vascular relations of hepatic hydatid cysts compared with abdominal CT scans, we recommend systematic IOUS for all hepatic hydatid cysts to prevent post-operative recurrences and reduce morbidity after conservative treatment. However, ultrasound, CT scans, and IOUS had a modest agreement in detecting complications, especially suppuration. Still, IOUS offers better performance in detecting CBFs.
Regarding the Gharbi and WHO classifications, abdominal ultrasound, CT scans, and IOUS showed good concordance in defining WHO cyst types, particularly IOUS, which demonstrated strong agreement. However, distinguishing between CE3b and CE4 types was unreliable with abdominal ultrasound and CT scans, whereas IOUS had good concordance in differentiating between these two types.
The treatment of CE3b type hepatic hydatid cysts is often surgical management. A good understanding of the natural history of hydatid disease suggests surveillance for CE4 type, adopting a watch-and-wait approach. 8 Hence, the relevance of IOUS in multiple hydatidosis: when surgical intervention is indicated, IOUS could potentially prevent the treatment of CE4 type cysts, especially those with challenging access (hepatic dome). This approach might reduce post-operative morbidity. Pre-operative MRI could be valuable in distinguishing between CE3b and CE4 types. It could guide surgical indications in managing hepatic hydatid cysts, potentially avoiding surgery for patients with CE4 type cysts.
Although our prospective study gave valuable insights into the imaging modalities of HCE, our results remain hypothetical, given the sample size of the studied cysts. The subgroup of patients having CE3b and CE4 is even smaller, which hinders the generalization of our conclusions in this regard. Our study evaluated many parameters simultaneously and no primary end points to the study were designated and thus may not have sufficient statistical power to draw meaningful conclusions. Thus, further studies will be necessary to affirm our results.
Conclusions
Compared with pre-operative ultrasound and CT scans, IOUS was the most effective in detecting exocysts and vascular relations of HCE. Therefore, the systematic use of IOUS for all HCE is essential. This approach could prevent recurrences and reduce post-operative morbidity.
Footnotes
Acknowledgments
The authors thank all the members who have contributed to this study and appreciate this group for their dedication and collective effort over the course of five years.
Authors' Contributions
Writing—original draft: Toumi. Zribi. Writing—review and editing: Trigui, Dziri. Methodology: Trigui, Fendri, Saumtally. Conceptualization: Trigui, Mzali. Supervision: Trigui. Visualization: Fendri, Akrout. Formal analysis: Saumtally, Ketata. Supervision: Mzali. Investigation: Dziri. Project administration: Ben Amar, Boujelbene.
Funding Information
All authors declare that we do not have any relevant or material financial interests that relate to the research described in this article.
Author Disclosure Statement
All authors declare that we do not have any conflicts of interest.