
Abstract
Background:
No in vitro surgical study has evaluated the time-dependent contamination of surgical suction tips compared with controls. Our purpose was to determine the difference in suction tip bacterial contamination rates between suction-positive and suction-negative tips.
Materials and Methods:
A matched-pair analysis of the contamination of surgical suction tips over a six-hour period was performed in two clean operating rooms. One suction tip was connected to standard wall suction (suction-positive group), with a matched control tip not connected to wall suction (suction-negative group). At time zero and then at hourly intervals for six hours, the distal 3 cm of suction tips were removed, placed in nutrient broth for 48 hours, then plate cultured. One hundred tips were collected for each time interval.
Results:
Eighty-two of 700 (11.7%) suction tips had bacterial contamination. Sixty-three (18.0%) of 350 suction-positive tips were contaminated, with 19 (5.4%) of the 350 suction-negative tips contaminated (χ2 = 26.7, p < 0.001). Suction tip contamination was time-dependent with the first significant difference between groups occurring after two hours of continuous suction (χ2 = 4.0, p = 0.04). Contamination rate in the suction-positive group increased significantly after one hour compared with time-zero controls (χ2 = 7.1, p = 0.008). There was no significant difference in frequency of positive cultures over time in the suction-negative group compared with time-zero controls.
Conclusions:
This is the first controlled laboratory study suggesting a time-dependent increase in positive suction tip cultures. From our data, operating room staff should have an awareness that suction tips represent a potential source of bacterial concentration. We recommend that when not in use, suction tip valves be closed if this feature is available, that hosing be manipulated to cease suction when not needed, that suckers be disconnected from tubing, or that suckers be exchanged at frequent intervals. Doing so may reduce bacterial contamination on the suction tip.
Surgical site infections (SSIs) have a prevalence of 0.53% to 1.3%1,2 in the United States, with an estimated rate of 100,000 to 300,000 annually.3,4 Surgical site infections are believed to account for nearly 20% to 39% of all hospital-acquired infections, 5 and as many as 75% of deaths associated with SSIs are believed to be a direct result of the infection, with a significant historical annual economic burden of $1 to $10 billion and more recent data suggesting annual costs of $2.4 to $5.0 billion.4,6,7 Specifically for orthopedic surgery, the incidence of SSI ranges from 0.4% to 3.6%8,9 with an incidence of 0.39% to 1.2%10,11 after primary total knee arthroplasty, 3.1% in spine, 12 and between 1% and 18.6%13,14 for orthopedic trauma. Through improvements in patient selection, sterilization procedures, surgical techniques, operating room ventilation, and barriers such as drapes, gowns, and gloves, the rate of SSI has declined in recent decades.15,16 However, because the U.S. population is aging and increasing, the number of surgeries, and therefore SSIs, will eventually increase. 15
Although the cause of SSI is multifactorial, surgical suction tips have been theorized as a possible contributor,17,18 with tip contamination rates in the orthopedic literature ranging from 7.3% to 54%.18-26 The high contamination rate of suction tips is the result of airborne particles, some of which serve as vectors for microbes27-29 that carry with them an increased risk of SSI.25,28-31 These particles may originate from the skin of patients or personnel in the operating room or from operating room equipment.25,32,33 Indeed, a single staff member dressed in sterile garments sheds tens of thousands of particles greater than 5 mcm/min, nearly 200 of which may contain microbes. 27 Throughout the duration of a procedure, suction tips aspirate substantial quantities of air and airborne particles 19 and continuous suction is a necessity in many orthopedic surgeries, making them a nidus for bacterial growth and colonization.19,21 Despite this risk, the available literature about suction tip contamination and SSI is both conflicting and sparse.
A number of studies suggest time-dependent contamination of suction tips.18–20,26 Yet one study that examined suction tip contamination rates during aortic valve replacement surgery reported no evidence of time-dependent contamination but a contamination rate of nearly 50%. 32 Notwithstanding the conflicting data on time-dependent contamination of suction tips, their high contamination rate has led some to hypothesize that suction tips may serve as a reservoir for micro-organisms and pose a risk for SSI.17,23 However, the implications are not well understood. 21
Few studies have assessed the intra-operative contamination rate of suction tips regardless of surgical specialty. Additionally, many of the available studies are low power and were published decades ago when operative procedures, operating rooms, sterile technique, and air flow technology were different from today. Therefore, our purpose was to investigate the rate of time-dependent bacterial contamination of surgical suction tips on continuous suction compared to suction tips not on continuous suction in a sterile operative environment. We hypothesized that the rate of contamination of both suction tips would increase with time, with the suction tip on continuous suction having a higher contamination rate.
Materials and Methods
This was an in vitro experiment performed over the course of nine weekend days. Institutional Review Board approval was granted by the main institution and funding was obtained from the principal investigator's affiliated department. All procedures and testing for this study were performed at 47.0% to 50.0% humidity in two unoccupied, negative pressure operating rooms with 26 to 28 air changes per hour through a HEPA filter evacuated to the external atmosphere. The operating rooms were connected by an anteroom that contained an autoclave and incubator. Traffic entering and leaving the operating rooms was limited to two personnel who entered and exited through the anteroom at each hourly time interval investigated.
The primary endpoint of the study was bacterial contamination of sterile, disposable Yankauer suction tips with a secondary end point of contaminating organism identified on culture. A matched-pair analysis of time-dependent contamination of surgical suction tips was performed, comparing suction tips connected to continuous suction (suction-positive group) to suction tips that were not connected to continuous suction (suction-negative group). The rate of contamination among suction-positive tips was compared across all timepoints. Similarly, the rate of contamination among suction-negative tips was compared across all timepoints. To achieve time-dependent testing, suction tips were collected at time zero to serve as controls and suction tips were then collected hourly starting after one hour of testing and ending after six hours. This yielded seven total timepoints that were examined (time zero, one hour, two hours, three hours, four hours, five hours, and six hours). At the conclusion of six hours, in one operating room, there were two sets of seven time-dependent data points: one set from continuously aspirating suction tips and one from the non-suctioning matched controls.
Using two operating rooms, the six-hour process was completed 25 times in each room. After all rounds of testing were complete, there were 350 suction tips in the suction-positive group and 350 in the suction-negative group for a total of 700 suction tips. Across all seven timepoints, 50 suction tips were in each group for a total of 100 suction tips in each of the seven timepoints.
The operating rooms were prepared for testing first by placing a sterile drape across the operating table in the center of the operating room where the patient would typically be positioned. The sets of suction tips were evenly spaced from the head to the foot of the operating table. One suction tip was connected to its own wall suction apparatus using an intervening suction canister. The associated control tip was not connected to suction (Fig. 1).
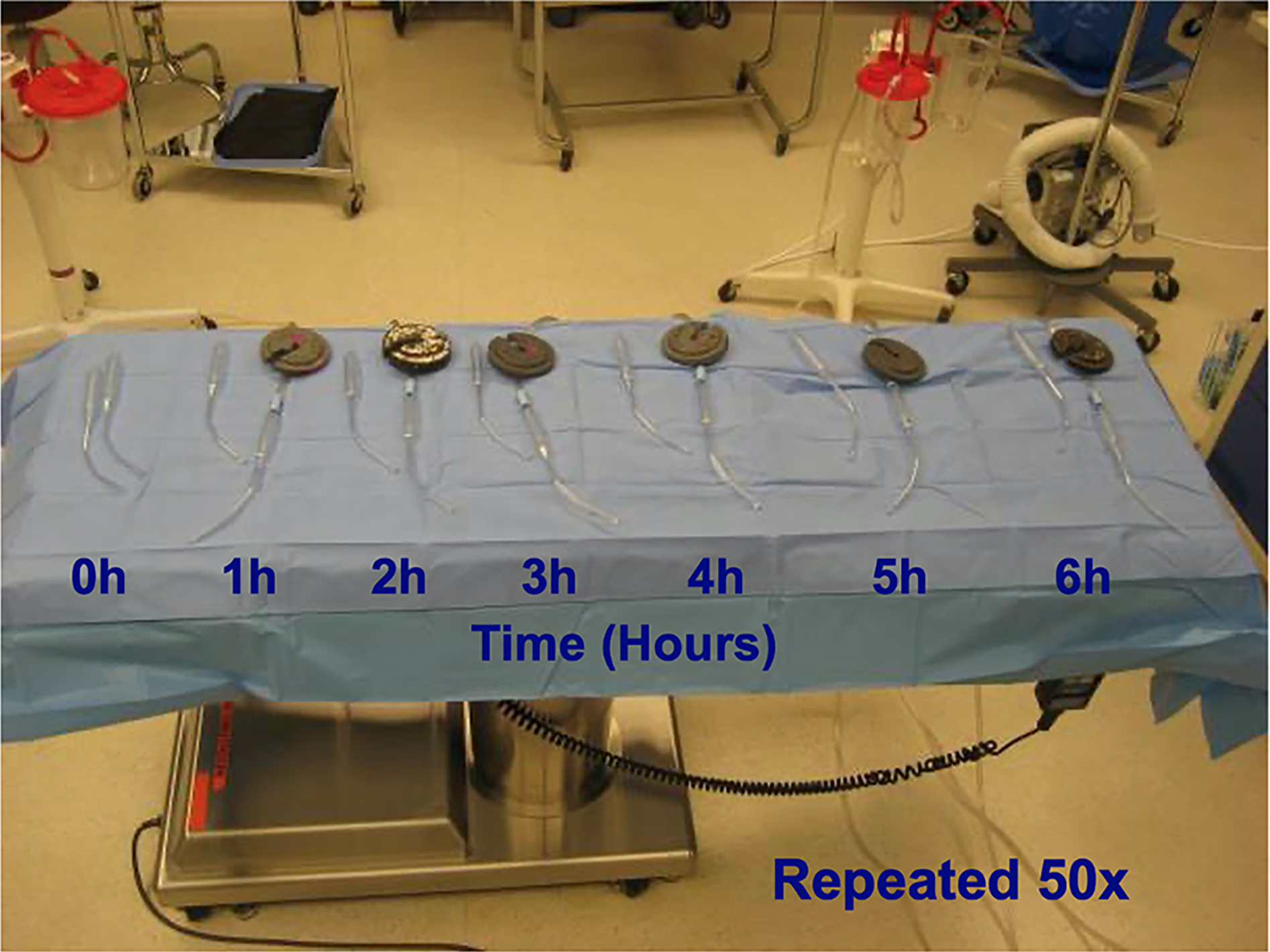
Testing set-up. h, hours. Color image is available online.
This set-up was repeated in the second operating room. Suction was then turned on for the seven suction-positive tips. The positioning of suction tips proceeded from time zero, corresponding to the foot of the operating table, and progressed to the head of the table where time-six-hour tips were located. At appropriate time intervals, the distal 3 cm of suction tips were cut off using sterile technique with freshly sterilized trauma scissors. There were two scissors for each operating room, one for suction-positive specimens and one for suction-negative specimens. The four sterile trauma scissors were run through a 12-minute cycle in the anteroom autoclave between each hourly use. Tips were incubated for a minimum of 48 hours by the microbiology laboratory, then plated for culture.
The first 224 samples were all incubated and plated after 48 hours. All plated cultures from cloudy-appearing test tubes yielded bacteria. None of the clear test tubes yielded bacteria after being plated by standard microbiologic lab methods. At this point it was determined that plating clear tubes would not be a good use of resources after proving 224 times that test tube cloudiness was a reliable indicator of culture positivity. The following 476 test tubes were plated if they were deemed turbid after a minimum of 48 hours of incubation.
All non-graphical data were analyzed with SPSS Statistics, version 25.0 (IBM Corp, Armonk, NY). Significance was set at 5%. Descriptive statistics were used to assess frequencies and percentages. The χ 2 test was used to observe any difference between groups for frequency of positive culture. Odds ratios and likelihood ratios were calculated using the crosstabs feature. GraphPad Prism 9.0 (GraphPad Software Inc., San Diego, CA) was used to create all graphical representation of data.
Results
Seven hundred suction tips were included in the final analysis, with 350 suction tips in the suction-positive group and 350 in the suction-negative group, yielding 50 tips from each group to compare at different timepoints. The overall suction tip contamination rate was 11.7% (87/700). Across all timepoints combined, the suction-positive group had a higher frequency of bacterial contamination (63/350; 18.0%) than the suction-negative group (19/350; 5.4%; χ 2 = 26.7, p < 0.001). There was no significant difference in contamination rate between time-zero control suction-positive tips and the suction-negative group at any of the seven timepoints tested. The first group-matched timepoint at which the rate of contamination in the suction-positive group exceeded that of the suction-negative group was after two hours of continuous suction (n = 8 [16.0%] vs. n = 2 [4.0%], respectively; χ 2 = 4.0, p = 0.04). In addition, the rate of contamination in the suction-positive group at one hour also exceeded that of the suction-negative group at two hours (n = 9 [18.0%] vs. n = 2 [4.9%], respectively; χ 2 = 5.0, p = 0.03). There was a relative time-dependent increase in the frequency of positive culture results with continuous suction compared with the suction-negative group, with the six-hour group having the greatest difference (n = 20 [40.0%] for suction-positive vs. n = 3 [6.0%] for suction-negative, χ 2 = 16.3, p < 0.001) (Table 1 and Fig. 2).

Graph of percent contamination by hour.
Time Comparison of Contamination in Suction-Positive and Suction-Negative Groups
n = sample size.
Comparing the contamination rate of suction-positive tips to other suction-positive tips across all timepoints, one hour of continuous suction was the first time interval that differed compared with time zero suction-positive tips (n = 9 [18.0%] vs. n = 1 [2.0%]; χ 2 = 7.11, p = 0.008). This comparison showed a relative time-dependent increase in the frequency of positive culture results (Table 2). The comparison of suction-negative at time zero to suction-negative at all other timepoints showed no difference in positive cultures and no time-dependent change in positive culture results. There was no significant difference in frequency of positive culture results at any compared time points within the suction-negative group. The odds ratio of contamination after one hour or more of continuous suction was 12.77 (95% confidence interval [CI], 1.73–94.27) with a likelihood ratio of 14.47 (p < 0.001).
Time Comparison of Suction-Positive to Suction-Positive Groups
n = sample size
Analysis of bacterial contamination revealed that 87.3% (n = 76) of cultured bacteria were Staphylococcus species with Staphylococcus hominis (44.0%) and Staphylococcus epidermidis (34.0%) making up the majority. coryneform bacilli, or diphtheroids, were also identified (n = 5; 6.1%) as were Bacillus spp. (n = 5; 6.1%; Table 3).
Bacterial Contamination Related to Presence of Suction
n = sample size.
χ 2 = 26.74, p < 0.001.
Discussion
Lower infection rates directly correlate with decreased morbidity and mortality, length of stay, and cost of care.34,35 Despite major peri-operative procedural improvements that address the most common risk factors of bacterial colonization and infection, surgical instruments are often considered sterile for the duration of the case. However, this assumption should be questioned because there is a time-dependent increased risk of infection with longer surgical times. A clinical risk model in pediatric spine deformity showed that surgery time of greater or equal to seven hours was associated with greater risk of deep SSI. 36 Although several studies have assessed the sterility of surgical instruments and equipment throughout the duration of an operation, fewer have focused on the sterility of suction tips.
Comparison of time zero suction-positive group to all other suction-positive timepoints in this analysis demonstrates that continuous suction greater than one hour increases bacterial contamination of the suction tip in a time-dependent manner. The comparison of suction-negative at time zero to suction-negative at all other timepoints showed no difference in frequency of contamination and no time-dependent change in frequency of contamination. Additionally, there was no significant difference in frequency of positive culture results in any of the suction-negative vs. suction-negative comparisons performed, suggesting that bacterial contamination of a clean suction tip does not change when suction is inactive. Last, a difference between suction-positive and suction-negative groups was found after one to two hours of continuous suction, with a relative time-dependent increase in frequency of positive culture results with continuous suction compared with the suction-negative group. The likelihood ratio of contamination with one hour or more of continuous suction was 14.47, which is a large and conclusive increase in the likelihood of contamination. 37 In total, these data represent the first controlled laboratory study to corroborate the results of previous intra-operative studies suggesting a time-dependent increase in positive suction tip cultures with continuous suction.18-20,26
Similar findings that frequently support the notion of time-dependent contamination of suction tips have been reported in the orthopedic literature. Of 546 suction tips used for orthopedic trauma surgery, González Edery et al. 20 found evidence of time-dependent contamination after one hour with an overall contamination rate of 7.3%. Another report on 50 orthopedic patients found 27 (54%) contaminated tips with most contamination occurring after one hour of continuous suction. 19 Greenough 18 found evidence of time-dependent contamination in 61 patients undergoing hip replacement. In 30 tips that underwent continuous suction, there was a 37% (11/30) incidence of contamination compared to a 3.2% (1/31) incidence (p = 0.002) in the group that had replacement of suction tips before and after preparing the femoral canal for stem placement. 18 Fuchs et al. 26 evaluated suction tip contamination in 100 total knee procedures, finding a 22% incidence of contamination, and recommended that suction tips be replaced every 30 minutes. In the only study that suggests no time-dependent contamination of suction tips, Larsson et al. 32 assessed the rate of suction-tip contamination in aortic valve replacement surgery. However, this was a small study with several confounders and flaws in how the procedures were divided into short and long duration of continuous suction. 32 The available literature on suction tip contamination suggests that approximately one hour of continuous suction is the timepoint at which contamination rates increase,19,20 with our results suggesting a time between one and two hours.
Our data on the time-dependent contamination of suction tips are corroborated by four different intra-operative orthopedic studies.18–20,26 Similarly, there is significant agreement between our culture data and that found in the literature. Staphylococcus hominis and epidermidis were the most common bacteria isolated in our analysis, which aligns with the most common bacteria isolated from suction tips in the intra-operative literature.18–20,22–24 Although contamination does not equal infection, 19 the most common causal organisms of SSI are very similar to those that tend to contaminate suction tips.8,13,18,19,22–25,38,39 In line with this, some data suggest that airborne particles are the primary source of SSI,28,29 with as many as 80% of infections after total hip arthroplasty being caused by airborne bacteria. 23
Additional data suggest that up to 98% of bacteria in wounds after an operation are due to airborne particulate matter. Only 30% of these bacteria are believed to have fallen directly into the surgical site with the rest being transferred into the surgical site by other routes. 40 The implications of suction tip contamination are not well understood, 21 with one report describing only a single case of deep wound infection after 27 (54%) suction tips were determined to be contaminated on culture. 19 However, definitive conclusions cannot be drawn from one study with relatively low power. Suction tips represent a means of concentrating airborne bacteria, 18 and the culture speciation similarities between SSI and suction tips justify concerns around the association between the two.
To the best of our knowledge, this study represents the only controlled, in vitro study evaluating the time-dependent contamination of surgical suction tips. Even so, several limitations are present. Our testing environment did not mimic an active operating room with a patient, surgeon, anesthesia personnel, other ancillary staff, or blood on the suction tip that may increase the risk of contamination. Likewise, continuous sucking of blood and irrigation in an operative field could wash the tip and have less resulting contamination in vivo. Although we had 700 samples with 100 samples at each timepoint, a power analysis was not performed, and we only tested one type of suction tip. Furthermore, to decrease resource use, we did not culture 476 of the tips. Although tube turbidity appeared to be a reliable indicator of culture positivity, there may have been error in its estimation. Last, because patients were not studied, we cannot comment on the association between suction tip contamination and SSI. A comparison of suction tip culture, surgical site culture at the time of surgery, and wound culture in the case of SSI is necessary and would shed more light on the relationship between suction tip contamination, wound contamination, and SSI. Future in vitro studies of bacterial contamination of surgical suction tips should include suction tips that have been in contact with fluid capable of hosting bacteria (sterile water or agar-dipped suction tips), suction at varying rates, and different suction tip devices.
Conclusions
A difference between suction-positive and suction-negative groups was found after one to two hours of continuous suction with a relative time-dependent increase in frequency of positive culture results with the suction-positive group. This is the first controlled laboratory study to corroborate the results of previous intra-operative studies suggesting a time-dependent increase in positive suction tip cultures. From our data, operating room staff should have an awareness that suction tips represent a potential source of bacterial concentration. We recommend that when not in use, suction tip valves be closed if this feature is available, that hosing be manipulated to cease suction when not needed, that suckers be disconnected from tubing, or that suckers be exchanged at frequent intervals. Doing so may reduce bacterial contamination on the suction tip.
Footnotes
Acknowledgments
We acknowledge the Medical Writing Center at Children's Mercy Kansas City for review and editing of this manuscript.
Authors' Contributions
Data curation (lead): Warren. Formal analysis (lead): Warren. Formal analysis (equal): Noe. Investigation (equal): Warren, Noe, Stock, Juelson, Hotchkiss. Writing—original draft (lead): Warren. Writing—review and editing (lead): Warren. Writing—review and editing (equal): Noe, Stock, Juelson, Hotchkiss, Schwend. Conceptualization (lead): Schwend. Conceptualization (equal): Stock, Juelson, Hotchkiss. Methodology (lead): Schwend. Methodology (equal): Stock, Juelson, Hotchkiss. Project administration (lead): Schwend.
Resources (lead): Schwend. Funding acquisition (lead): Schwend. Supervision (lead): Schwend. Visualization (lead): Schwend.
Funding Information
The Rex and Lillian Diveley Research and Education Endowment provided all funding for this project.
Author Disclosure Statement
Dr. Juelson has no conflicts of interest pertaining to the subject matter of this study but has the following disclosures: common stock in Johnson & Johnson as well as Pfizer. Dr. Hotchkiss has no conflicts of interest pertaining to the subject matter of this study but has the following disclosures: Consulting fees from Medtronic, Ulrich Medical, Sanara Med Tech. The remaining authors report that they, their immediate family, and any research foundation with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article.