
Abstract
Background:
The diagnosis of brain tuberculoma (BT) is sometimes challenging. Herein, we presented a case series to evaluate the combined-diagnostic methods, including acid-fast bacilli (AFB) stain, polymerase chain reaction (PCR), Gene Xpert, and histopathology, of tuberculoma tissue specimens (TTSs).
Patients and Methods:
A total of 16 patients (11 human immunodeficiency virus [HIV]-positive, 5 HIV-negative) with BT confirmed by combined-diagnostic methods of TTS were included in this study. Clinical data, including clinical symptoms, laboratory tests, neuroimaging features, histopathology, treatment, and prognosis, were assessed in all patients.
Results:
There were 10 male and 6 female patients (range, 18–73 years). Acid-fast bacilli stain and PCR of TTSs were positive in 11 and 10 patients, respectively. The sensitivity of Gene Xpert of TTSs was (80.0%; 8/10). Nine (56.3%; 9/16) patients were diagnosed with BT by histopathology. After receiving antituberculosis treatment, 12 (75.0%; 12/16) patients improved clinically to a considerable extent.
Conclusions:
The combined-diagnostic methods of TTS may improve the diagnostic efficiency of BT.
M
The diagnosis of BT is sometimes challenging not only because lack of specific clinical 3 and imaging 4 characteristics, but also because of the wide range of sensitivity and specificity of test methods.5–8 Seeking useful and efficient diagnostic methods is always of crucial importance. Over recent years, although various diagnostic methods have been used for BT such as Mycobacterium tuberculosis culture identification, interferon-γ release assays (IGRAs), acid-fast bacilli (AFB) stain, polymerase chain reaction (PCR), Gene Xpert, and histopathology,9,10 there does not seem to be a single diagnostic method to make a definitive diagnosis. 5
In the present study, we recruited 16 patients with BT confirmed by combined-diagnostic methods (AFB stain, PCR, Gene Xpert, and histopathology) of TTS. Clinical characteristics, including clinical symptoms, laboratory tests, neuroimaging features, histopathology, treatment, and prognosis were analyzed in all patients to assess the diagnostic value of the combined-diagnostic methods of TTSs.
Patients and Methods
Study design and population
Participants were recruited between September 2013 and February 2022, at the Department of Neurosurgery of Beijing Ditan Hospital. Sixteen participants with combined-diagnostic methods (AFB stain, PCR, Gene Xpert, and histopathology) of TTSs positive for Mycobacterium tuberculosis were enrolled in this study. Their clinical data, including clinical symptoms, blood examination (included routine blood test, IGRA, erythrocyte sedimentation rate [ESR], CD4+ T lymphocyte count, human immunodeficiency virus [HIV] viral load), cerebrospinal fluid (CSF) routine tests, CSF-PCR, neuroimaging features, histopathological characteristics, results of AFB stain, PCR, and Gene Xpert of TTSs, treatment regime, prognosis were retrospectively analyzed.
The institutional ethics committee of Beijing Ditan Hospital approved the study. All patients or their proxies provided written informed consent before inclusion in the study. Patient information was anonymized and de-identified. All methods were performed in accordance with the relevant guidelines and regulations.
Treatment administered and evaluations in participants
According to the results of combined-diagnostic methods of TTSs, all patients received standard doses of first-line antituberculosis treatment (ATT), which includes isoniazid, rifampicin, pyrazinamide, ethambutol, or streptomycin given in the first two months, followed by isoniazid and rifampicin for 16 months. Dexamethasone was given to relieve patients' symptoms for six weeks or until patients made an obvious clinical recovery. The patients who were HIV-positive also received combined antiretroviral treatment (cART) at the proper time. All patients were followed up by telephone or outpatient service to inquire about survival status; overall survival (OS) was the period from operation to follow-up or death. Brain magnetic resonance imaging (MRI) was re-examined during hospitalization or in outpatient service to regularly assess the progress. Two trained senior residents collected clinical data. Senior radiologists were also invited to assist in making the diagnosis.
Combined-diagnostic methods in TTSs
All samples were examined by PCR, GeneXpert MTB/RIF assay, AFB stain, and histopathology. Microscopic smear microscopy with Ziehl-Neelsen staining was performed by two trained laboratory physicians and the results were diagnosed on the laboratory rules. The DNA for PCR were extracted from 500 mcg brain tissue using QIAamp Fast DNA Tissue Kit (catalog #51404) according to the manufacturer's protocol. Total extracted DNA samples were stored at −80℃ for testing for TB. Tuberculosis was detected with a real-time PCR commercial kit. Polymerase-chain reaction results were positive when the cycle threshold (Ct value) ≤38 cycles. GeneXpert MTB/RIF assay with 500 mcg brain tissue were operated strictly in accordance with the instructions of the GeneXpert MTB/RIF system and the results were automatically given by the built-in algorithm. Tuberculoma tissue specimens were stained with hematoxylin and eosin stain and were examined under a microscope for AFB and epithelioid cell granuloma and Langerhans cell with or without caseation. All reports were confirmed by the senior laboratory physician or pathologist.
Results
Clinical characteristics of participants
Among 16 cases, 11 patients were HIV-positive and five were HIV-negative, with 10 males and six females. The average age of 16 cases was 41.88 ± 16.19 years (median age, 40.5 years; range, 18–73 years), wherein 43.36 ± 16.82 years (median age, 41 years; range, 18–73 years) in patients who were HIV-positive and 38.6 ± 14.18 years (median age, 33 years; range, 19–59 years) in patients who were HIV-negative.
The main two symptoms were headache (62.5%, 10/16) and seizures (56.3%; 9/16), followed by hemiplegia (31.3%; 5/16), fever (25.0%; 4/16), nausea and vomiting (25.0%; 4/16), dizziness (18.8%; 3/16), dysphasia (12.5%; 2/16), paraesthesia (12.5%; 2/16), homonymous hemianopia (6.25%; 1/16), and diplopia (6.25%; 1/16; Table 1). Fever occurred mainly in patients combined with TBM or extracranial TB. The duration of symptoms at presentation ranged from approximately seven to 210 days; nine patients presented within 30 days of onset, among them, seven were HIV positive. Extracranial TB was detected in seven patients (43.8%; 7/16) in the form of pulmonary tuberculosis (PT; 6 patients), lymph node tuberculosis (LNT; 1 patient), abdominal tuberculosis (AT; 1 patient), and pleural tuberculosis (PLT; 1 patient).
Symptoms and Signs in Sixteen Patients With BT
BT = brain tuberculoma; L = left; R = right.
The course of HIV, which was defined as the time between HIV-positive and first symptoms of BT, was 0 to 1,090 days; seven patients were found to be HIV-positive at or after the time of first symptoms of BT. In addition, nine of the 11 HIV-positive patients had never received cART at the time of first symptoms of BT (Table 2).
Demographic and Clinical Characteristics in Sixteen Patients With BT
M = male; F = female; cART = combined anti-retroviral treatment; Y = yes; N = no; CD4 = cluster of differentiation 4; VL = HIV viral loads in serum; BT = brain tuberculoma; S = supratentorial; I = infratentorial; Sin = single; Mul = multiple; TBM = tuberculosis meningitis; TB = tuberculous; PT = pulmonary tuberculosis; LNT = lymph node tuberculosis; AT = abdominal tuberculosis; PLT = pleural tuberculosis; WBC = white blood cell; ESR = erythrocyte sedimentation rate; R = resection; B = biopsy; IGRA = interferon-γ release assay; PCR = polymerase chain reaction; TTS = tuberculoma tissue specimen; AFB = acid-fast bacilli; GX = Gene Xpert; PD = pathologic diagnosis; IL = inflammatory lesions; OS = overall survival; NA = not available; HIV = human immunodeficiency virus; CSF = cerebrospinal fluid.
Time in days between first symptoms and admission.
Time in days between HIV-positive and first symptoms of BT.
Received cART before the first symptoms of BT for at least 2 weeks.
At time of admission because of BT.
The range of normal value is 0–15 mm/h.
The duration from operation to follow-up or death.
Patient was found HIV-positive at or after the time of first symptoms of BT.
The patient who died.
Laboratory investigations
The white blood cell (WBC) counts ranged from 1.99 to 11.27 × 109/L (median, 7.7 × 109/L) in blood and 0 to 155 × 106/L (median, 9 × 106/L) in the CSF of the 11 patients available for CSF routine test, eight patients' WBC counts were <20 × 106/L, and another three patients with TBM showed leukocytosis of 93 to 155 × 106/L in CSF. Erythrocyte sedimentation rate was elevated (14–101 mm/h) in most (92.9%; 13/14) patients. Interferon-γ release assays were positive in five patients, four combined with extracranial TB. Although 11 patients were available for CSF-PCR, only one was positive. In 11 HIV-positive patients, CD4+ count ranged from 2 to 195 cells per microliter (median, 43 cells per microliter), serologic HIV viral load ranged from 0 to 347,8226 copies per milliliter (median, 1,712 copies per milliliter).
Imaging characteristics
Brain tuberculoma was located in the basal ganglia, thalamus, cerebellum, brain stem and every brain lobe, at the cortical/white matter border, with peri-focal edema and occupying effect. These lesions showed hypodensity in computed tomography (CT) and had isointense on T1-weighted images (T1WI), hyperintense on T2-weighted images (T2WI), and ill-defined or homogeneous or ring enhancement on contrast, but they all lacked specificity (Figs. 1 and 2). Seven (43.8%; 7/16) patients presented with multiple brain lesions, which were mainly located in the supratentorial area (81.3%; 13/16), evolving in the hemispheres either unilaterally or bilaterally.
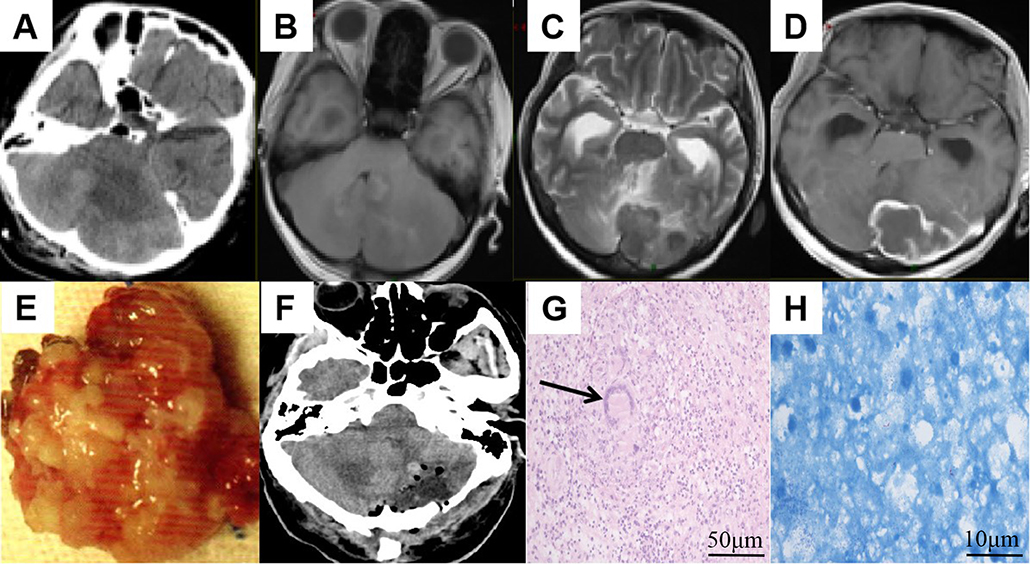
Imaging examination, shape of tuberculoma, and histopathology result of case 10.

Imaging examination, intraoperative findings and histopathology result of case 15.
Combined-diagnostic methods of TTSs
Tuberculoma tissue specimens were obtained from all cases. Fourteen were culture available, only six (42.9%; 6/14) were positive. All 16 TTSs were available for AFB stain and PCR; there were 11 and 10 positive specimens by AFB stain (68.8%; 11/16) and PCR (62.5%; 10/16), respectively. By different tissue staining techniques, two patients who were HIV-positive were indicated to have coinfections among TB and fungus, as well as TB and gram-positive cocci, respectively. Ten TTSs were available for Gene Xpert, with eight (80.0%; 8/10) positive; another two were also negative by culture and PCR, the diagnoses of BT were according to the histopathology.
Nine (56.3%; 9/16) patients were diagnosed with BT by histopathology with the characteristic features of caseating tuberculous granuloma. The other six patients only presented with non-specific glial cells and microvasculature hyperplasia, infiltration with inflammatory cells, with a diagnosis of inflammatory lesions (Figs. 1 and 2).
Treatment and prognosis
Nine patients underwent resection of BT; biopsy was performed in another seven patients. Eleven patients' clinical conditions improved to a considerable extent after receiving the ATT as previously described, and the BT on the MRI obviously shrunk and disappeared. Five patients died; one patient had fungal meningoencephalitis, the BT on the MRI shrunk after receiving the ATT, but the fungal infection was not well controlled and subsequently the patient died from malignant intracranial hypertension. The remaining four patients died due to advanced, extensively disseminated disease during treatment. The OS of the 16 patients was one to 111 months (median time, 42.5 months).
Discussion
Although only 1% of TB cases involve the CNS, these cases represent the most severe form of the disease, leads to serious permanent neurological damage, even lethal complications,11–13 particularly in patients who were HIV-positive. Therefore, efficient diagnostic strategy of BT is imperative in minimizing the risk of complications and improving overall outcomes by virtue of timely diagnosis and treatment.
In terms of clinical features, similar to other occupied lesions in the brain, BT might exert local mass effect on brain tissue, leading to headache, vomiting, decreased consciousness, focal neurological signs, and seizures. 14 Therefore, there is no specificity of the clinical features in BT.
The diagnosis of BT is often with the help of imaging techniques such as CT and MRI. 4 Brain imaging of BT frequently manifests clinically silent single or multiple CNS granulomata with or without meningitis. On CT, the characteristic appearance is a nodular enhancing lesion with a central hypodense region; on MRI, the early focal cerebritis stage is marked by edema and ill-defined enhancement, the later mature stage by central hypointensity and peripheral enhancement.3,15,16 However, several diseases are also capable of producing similar imaging features, such as cysticercosis, toxoplasmosis, fungal granuloma, bacterial abscesses, brain neoplasms (gliomas, lymphomas and brain metastases). 16 In our study, merely according to imaging features, three patients (case 10, 13, and 15) treated with antitoxoplasma, two patients (case 3 and 12) treated as cerebral infarction prior to hospitalization. Thus, relying solely on neuroimaging, which is difficult to differentiate BT from other brain parenchymal lesions, even harmful.
Interferon-γ release assays are among the commonly used Mycobacterium tuberculosis tests available. Interferon-γ is released by CD4+ T-cells, which induce macrophage activation and promote destruction of mycobacteria. 17 Advantages of IGRAs include latent tuberculosis infection detection and specificity that is relatively unaffected by the TB vaccine. Simmons et al. 18 reported IGRAs-positive rate of 50% among culture-confirmed cases of TBM. Nevertheless, these assays do not differentiate between latent and active Mycobacterium tuberculosis infection, 19 also the diagnostic sensitivity of IGRAs will be reduced in immunocompromised persons. Hence, in this study of patients who were mainly HIV-positive, the sensitivity of IGRAs is 35.7% (5/14).
Culture identification for Mycobacterium tuberculosis is always the gold standard for diagnosing BT, allowing for drug sensitivity testing, which is essential for appropriate treatment. However, it has low sensitivity, 15 which is affected by various factors such as paucibacillary as nature of disease, 20 type of species, experience of the technical person, and so on. 5 In addition, Mycobacterium tuberculosis is particularly slow growing with a time period of approximately four to eight weeks. 21 The indolence hinders MTB culture detection within a clinically relevant time frame, because immediate treatment is vital for the diagnosis of BT. In our study, only six (42.9%; 6/14) TTSs for culture positive, in addition to the reasons mentioned above, six of the eight culture-negative patients were HIV positive, which may be due to the statement that bacillary load of Mycobacterium tuberculosis is usually low in HIV-positive patients, 22 compromising sensitivity of bacteriologic tests.
Polymerase chain reaction is an effective method for the rapid detection of specific bacterial DNA in clinical specimens, which can be useful to improve the speed and accuracy in detecting Mycobacterium tuberculosis. However, the reliability of PCR testing for Mycobacterium tuberculosis DNA is not well established, primarily because of variability in sensitivity and specificity across multiple laboratories. A meta-analysis of PCR of CSF for TBM showed a pooled sensitivity of 56% and specificity of 98%. 6 Another article has proven high specificity (80%–100%), a wider sensitivity range (30%–100%) has been shown. 23 The low sensitivity of PCR is due to the PCR inhibitors such as host proteins, blood, and even eukaryotic DNA in extrapulmonary specimens. 24 The sensitivity of PCR of TTSs was 62.5% (10/16) in this study, the six negative TTSs were also negative by culture, which may also attribute to low bacillary load of Mycobacterium tuberculosis in HIV-positive patients 22 (4/6 negative patients were HIV-positive).
Gene Xpert is a rapid automated molecular test with high accuracy, reduces hands-on time, decreased risk of cross contamination and the ability to identify rifampicin resistance for pulmonary 25 and various extrapulmonary samples of TB such as CSF, urine, lymph node, and other tissues,7,26 which is recommended by the World Health Organization (WHO) for TB detection. A meta-analysis of 30 studies indicated that Xpert MTB/RIF pooled sensitivity and specificity against culture were 71.1% (62.8 to 79.1) and 96.9% (95.4 to 98.0), respectively. 7 In another meta-analysis of 13 studies in which Gene Xpert was evaluated against culture, the pooled sensitivity was 80.5% and specificity 97.8%. 27 In our series, eight positives in 10 Gene Xpert of TTSs were found, with a sensitivity of 80.0%. Nevertheless, despite Gene Xpert being more sensitive than other coexisting conventional methods, 28 it still cannot absolutely identify all cases of CNS-TB.
There are few studies reported on GeneXpert or PCR for the detection of Mycobacterium tuberculosis in TTS, especially in patients who were HIV-positive thus far. However, when BT is the only lesion, not complicated by meningitis, definite diagnosis of BT using CSF remains difficult, because Mycobacterium tuberculosis may be encapsulated by fibrous of the caseous granulomas.3,16 A study performed by Dil-Afroze et al. 29 showed CSF-PCR was positive for 21 of 27 patients (77.7% sensitivity) of TBM patients, only six of 20 patients (30% sensitivity) with BT were positive. In our study, of the 11 patients available for CSF-PCR, only one patient was positive. This limitation of diagnostic strategy led to missed diagnosis of BT. 30
Histopathologic analysis combined with culture identification, remains the gold standard for diagnosis of BT. Tuberculomas are granulomatous mass lesions composed of a central zone of caseation surrounded by a collagenous tissue capsule. 31 Although histopathology is technically demanding and time consuming, 8 the sensitivity reported ranges from 50% to 60%.8,32 There are times when the pathology simply indicates that chronic inflammatory granuloma, which is insufficient for the diagnosis of tuberculosis, because this pathologic feature may also be found in other infectious and non-infectious disease. In our series, there were seven patients who only presented with non-specific glial cells hyperplasia and infiltration with inflammatory cells. In addition, histopathology does not distinguish between BT and other granulomatous diseases such as sarcoidosis, leprosy, and systemic lupus erythematosus. 33 Research from India, including only histopathologically verified cases of BT, revealed a lower rate of 54% complete resolution by 24 months of ATT, 34 which is mainly attributed to the failure of pathologic verification.
The sensitivity of AFB stain in various published studies was reported in the range of 20% to 60%, 5 which can be increased to a small extent using special physical and or or chemical methods of sample processing and special equipment such as fluorescent microscopy. 35 More than that, at times, we also need to distinguish between Mycobacterium tuberculosis and Mycobacterium leprae, which was also positive by AFB stain. The AFB stain of the sensitivity of TTSs in our study was 68.8% (11/16). Because these test methods above cannot offer sufficient sensitivity to confidently detect Mycobacterium tuberculosis alone, 5 however, combined-diagnostic methods of TTS, may be considered superior in diagnosing of BT. 11
Conclusions
In this study, 16 patients were diagnosed with BT by analyzing TTSs using a combined-diagnostic methods, all patients have been treated accordingly (ATT), 12 of 16 patients showing significant clinical improvement of BT. This not only demonstrated timely treatment of BT is effective but also proved the excellent diagnostic performance and necessity of combined-diagnostic methods when detecting Mycobacterium tuberculosis in TTSs.
Footnotes
Acknowledgements
We are grateful for the participants of this study; the study team; Beijing Ditan Hospital Affiliated to Capital Medical University staff permission and support to conduct this study.
Authors' Contributions
Design: B. Liang. Supervision: B. Liang, Feng, Zhao. Primary author: B. Liang. Conceptualization: Yang. Methodology: Yang, Li, Zhou, Gao. Writing—review and editing: Yang, Li, Zhou, Gao, Feng, Zhao. Documentation of demographic and clinical data of patients: T. Liang, Ding. Investigation: Li, Zhou, Gao, Feng, Zhao. Project administration: Feng, Zhao. All authors approved the final version submitted.
Data Availability
All data generated and analyzed during this study are included in this published article.
Funding Information
This work was funded by a grant to the Beijing Municipal Administration of Hospitals Incubating Program (Grant Number: PX2020071), “Bridge project” of Beijing Ditan Hospital Affiliated to Capital Medical University (Grant Number: DTQL202101), Beijing Municipal Administration of Hospitals' Ascent Plan (Grant Number: DFL20191802) and Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding Support (Grant Number: ZYLX202126).
Author Disclosure Statement
The authors report no conflicts of interest relevant to this article.