
Abstract
Background:
Although ultrasound is considered the gold standard for the evaluation of children with suspected appendicitis, there is still much debate about the most accurate ultrasound findings. The purpose of this study was to define the best ultrasound signs that could ultimately improve the diagnostic accuracy of ultrasound for diagnosing pediatric acute appendicitis, and to differentiate between simple appendicitis and complicated appendicitis.
Patients and Methods:
After approval by our Institutional Review Board, a prospective study was carried out from January 1, 2022, to July 31, 2023, in a pediatric emergency department. We included all patients aged under 14 years with suspected appendicitis and ultrasound-visualized appendix.
Results:
A total of 550 patients presented with suspected appendicitis during the study period. Of these children, 411 had an ultrasound-visualized appendix. Our patients' mean age was 9.4 years. The best positive predictive value of ultrasound was found for appendiceal diameter ≥7.5 mm. The combination of an appendiceal diameter <6 mm and the lack of peri-appendiceal free fluid on ultrasound rules out the diagnosis of appendicitis. The best diagnostic accuracy of ultrasound, which was 92%, was achieved for appendix diameters ≥6.5 mm. The sonographic sign giving the best ultrasound accuracy for diagnosing complicated appendicitis was an appendix diameter ≥9 mm.
Conclusions:
In conclusion, our present study demonstrated that appendiceal diameter ≥6.5 mm is the gold standard for diagnosing appendicitis in pediatric patients. The combination of an appendiceal diameter <6 mm and the lack of peri-appendiceal free fluid on ultrasound would rule out appendicitis.
Acute appendicitis (AA) ranks among the most common diseases that require urgent surgical care. 1 In the pediatric population, the diagnosis of appendicitis tends to be difficult, involving meticulous clinical, laboratory, and radiologic evaluation.2–7 The value and effectiveness of abdominal ultrasound for diagnosing pediatric AA has been widely recognized. Moreover, ultrasound is a radiation-free imaging modality. As a result, ultrasound is now the preferred imaging tool for the assessment of pediatric patients with suspected appendicitis in most university hospitals. Although ultrasound is commonly claimed to be less accurate than abdominal computed tomography (CT), sonographic findings usually play a crucial role in surgeon decision-making and lead to an improvement in negative appendectomy rate.8–12
Data from the literature suggest that the most reliable ultrasound feature for the diagnosis of pediatric AA is the appendiceal diameter, defined as the maximum outer diameter of the appendix. Thus, an appendiceal diameter at or above 6 mm is commonly accepted as an ultrasound sign of appendicitis.13–16 However, recent publications have shown that the cutoff value of 6 mm may not be the most accurate, and proposed the cutoff value of 7 mm as the most reliable appendix diameter for the diagnosis of AA in children.5,17–20 In addition, there is controversy as to the usefulness of the other ultrasonographic signs, including peri-appendiceal free fluid, increased peri-appendiceal fat echogenicity (PAFE), and appendicolith in diagnosing AA, and in differentiating between simple and complicated AA pre-operatively.5,18,21,22
The purpose of this study was to define the best ultrasound signs that could ultimately improve the diagnostic accuracy of ultrasound for diagnosing pediatric AA, and to differentiate between simple appendicitis (SA) and complicated appendicitis (CA).
Patients and Methods
After approval by our Institutional Review Board, a prospective study was carried out from January 1, 2022, to July 31, 2023, in a pediatric emergency department. We included all patients aged under 14 years with suspected appendicitis and ultrasound-visualized appendix.
Upon review of the patient's history and clinical examination findings, a consultant pediatric surgeon suspected AA. We performed abdominal ultrasound in all children with suspected AA. Ultrasounds were done by experienced pediatric radiologists during weekdays. During night hours (7:00
In our institution, every child has only one approved ultrasound report. The senior radiologist carries out the ultrasound on weekdays and signs off on the final report. A radiology resident performs the scan at night and on weekends and examines the images with the senior radiologist on duty, prior to signing the final report. This way, the surgeon receives only the final ultrasound report signed by the senior radiologist. We asked the radiologist to clarify if the whole appendix was visualized, to determine the appendiceal diameter, defined as the maximum outer diameter (MOD) of the appendix, and to indicate if there was evidence of secondary signs of AA, including appendicolith, peri-appendiceal free fluid, and increased PAFE. We considered partially visualized appendix on ultrasound with normal dimensions of the visualized portion as non-visualized. In our department, CT scans are not done on patients with visualized appendix on abdominal ultrasound. The decision to proceed with surgery is made by the consultant pediatric surgeon after considering the clinical, biologic, and ultrasound results.
In our department, we perform open or laparoscopic appendectomy for all patients diagnosed pre-operatively with appendicitis. We do not use non-operative antibiotic treatment for appendicitis. Our institutional policy for prescribing post-operative antibiotic agents is to use intravenous combination of cefotaxime (3 times daily, 5 days) and metronidazole (3 times daily, 5 days) for children with CA. Thereafter, oral antibiotic therapy could be pursued for two to five days, depending on the surgeon's advice. Post-operative antibiotic agents are not routinely administered to patients with SA.
We defined the final diagnosis of no appendicitis as a discharge from hospital or emergency department without a diagnosis of appendicitis and with no subsequent return within 14 days. The final diagnosis of appendicitis was defined as the intra-operative recognition of an inflammation of the vermiform appendix with pathologic confirmation of appendicitis. We defined CA based on intra-operative findings. The definition of CA covered perforated appendicitis, intra-abdominal abscess, and generalized peritonitis. We defined perforated appendicitis as a hole in the appendix identified during surgery. We defined gangrenous appendicitis as any black or gray discoloration of the appendiceal wall, but without the features that would classify it as a CA. 23 Data on age and gender were collected in addition to the above-mentioned ultrasound findings.
We used SPSS Statistics, version 20.0 (IBM Corp, Armonk, NY) for statistical analysis. We performed the Kolmogorov-Smirnoff and Shapiro-Wilk tests for each variable to check for normal distribution. Continuous normally distributed variables were reported as mean and standard deviation. Asymmetric data were expressed as median and quartiles. For continuous normally distributed variables, a Student t-test was done on independent samples. For non-normally distributed continuous variables, we applied the Mann-Whitney test. We reported discrete variables as frequencies and percentages and analyzed them by means of the χ 2 test. Those p values of <0.05 were considered as significant differences. Multivariable logistic regression was used to assess the risk-adjusted impact of various variables on the diagnosis of pediatric AA. Ultrasound accuracy was calculated using the following formula:
Accuracy = (True negative + True positive)/(True negative + True positive + False negative + False positive).24,25
Results
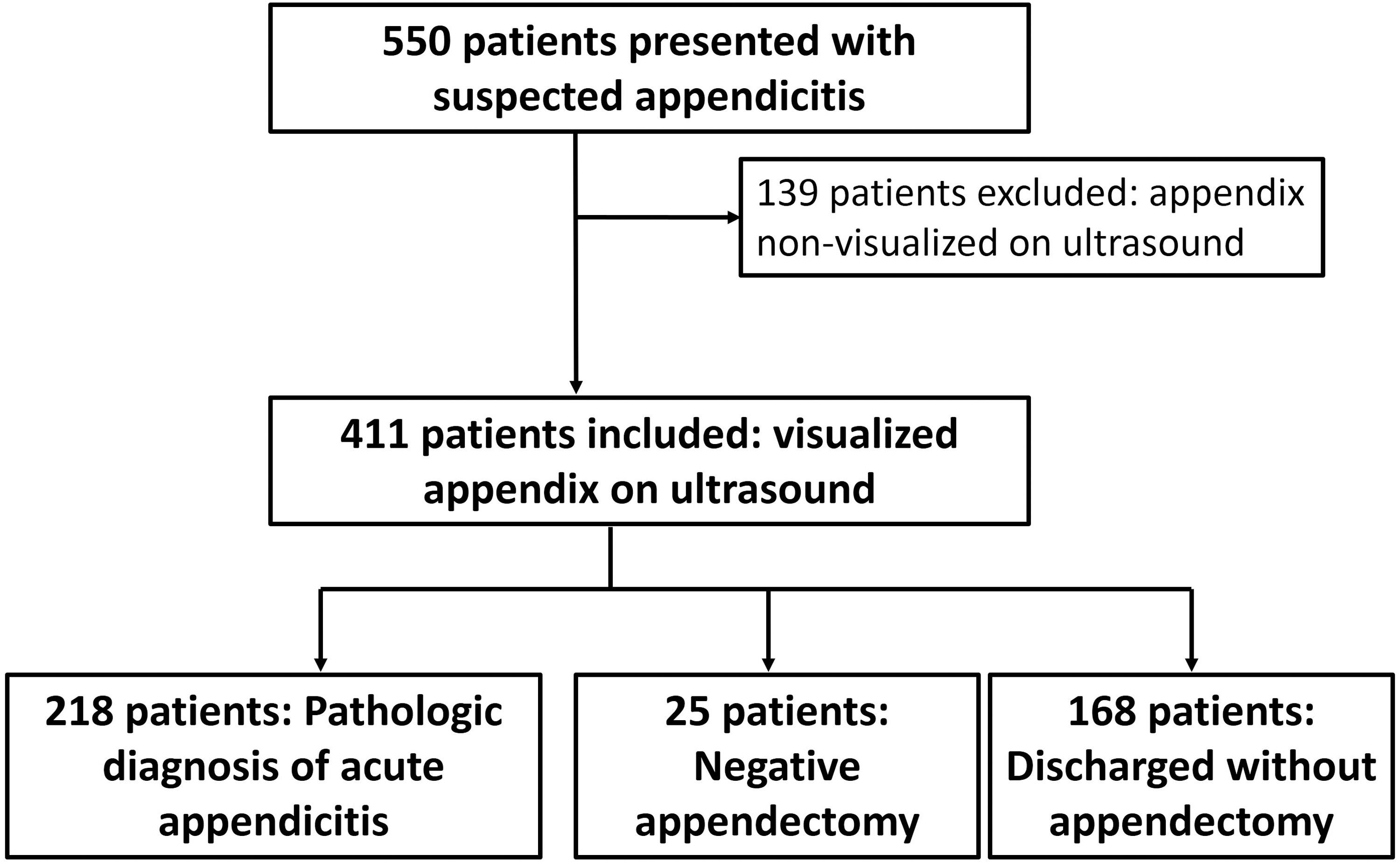
A total of 550 patients presented with suspected AA during the study period. Among these children, 139 (25.3%) with non-visualized appendix on ultrasound were excluded from this study. Based on clinical, biologic, and ultrasonographic findings, 243 of the 411 patients with visualized appendices underwent appendectomy. This resulted in 218 patients with pathologically confirmed appendicitis, giving a 10.3% negative appendectomy rate. In 168 of 411 children who did not require surgery, AA was ruled out because of the lack of clinical, biologic, and radiologic features consistent with appendicitis. These children were discharged and did not need further surgery.
Two hundred eighteen (53%) of the 411 patients with an ultrasound visualized appendix were finally diagnosed with AA on the basis of pathologic findings (Fig. 1). Other diagnoses included pyelonephritis (n = 5; these patients received suitable antibiotic agents), ovarian cyst (n = 7; spontaneous regression of these cysts was the main outcome), constipation (n = 24; these patients received lactulose with positive outcome), gastroenteritis (n = 60; antiemetics and oral rehydration solutions were the mainstays of treatment for these patients), and mesenteric lymphadenitis (n = 97; treatment was based on pain medication).
Study cohort assembly
Our patients' mean age was 9.4 years (standard deviation [SD], 2.6 years), with 60.1% (n = 247) of children being male. Appendix mean diameter on ultrasound was 7 mm (SD, 2.5 mm). Abdominal ultrasonography revealed a peri-appendiceal free fluid in 125 (30.4%) patients, an appendicolith in 37 (9%) patients, and an increased PAFE in 222 (54%) patients. None of our patients had an abdominal CT scan.
Comparison of ultrasound findings of children with AA and those without showed that patients with proven appendicitis had larger appendiceal diameters and higher incidence of appendicoliths, peri-appendiceal free fluid, and increased PAFE on ultrasound (Table 1). Table 2 illustrates the specificity, sensitivity, positive predictive value (PPV), and negative predictive value (NPV) of each of the variables detected by the univariable analysis. The best PPV (95%) was found for appendiceal diameter ≥7.5 mm. The best NPV was 100%. Therefore, the combination of an appendiceal diameter <6 mm and the lack of peri-appendiceal free fluid on ultrasound rules out the diagnosis of appendicitis. The best diagnostic accuracy of ultrasound was achieved for appendix diameters ≥6.5 mm. On multivariable logistic regression analysis, appendiceal diameter ≥6.5 mm and increased PAFE were found to be the sole independent risk factors for appendicitis. In contrast, male gender, appendicolith and peri-appendiceal free fluid did not appear to influence the diagnosis of appendicitis in our children (Table 3).
Univariable Analysis Comparing Demographic and Ultrasound Findings Between Acute Appendicitis and No Appendicitis Patients
AA = acute appendicitis; NA = no appendicitis; SD = standard deviation; PAFE = peri-appendiceal fat echogenicity.
p value has been bolded if p < 0.05.
Diameter = maximal outer diameter of the appendix.
Sensitivity, Specificity, and Predictive Values of Potential Predictors of Acute Appendicitis
CI = confidence interval; PPV = positive predictive value; NPV = negative predictive value; PAFE = peri-appendiceal fat echogenicity.
The best PPV, NPV, and accuracy were bolded.
Diameter = maximal outer diameter of the appendix.
Multivariable Logistic Regression Analysis: Predictors of AA
AA = acute appendicitis; OR = odds ratio; CI = confidence interval; PAFE = peri-appendiceal fat echogenicity.
p Value and odds ratio have been bolded if p < 0.05.
Children with a final diagnosis of appendicitis were split into two groups according to whether the appendicitis was simple or complicated. The univariable analysis comparing these two groups showed that the appendiceal diameter was higher in children with CA. Among the secondary ultrasound signs, only the presence of peri-appendiceal free fluid was predictive of CA (Table 4). Table 5 shows the predictive values, sensitivity, and specificity of possible risk factors for CA. The sonographic sign giving the best ultrasound accuracy, which was 68%, was an appendix diameter ≥9 mm.
Univariable Analysis Comparing Demographic and Ultrasound Findings Between Complicated Appendicitis and Simple Appendicitis Patients
CA = complicated appendicitis; SA = simple appendicitis; SD = standard deviation; PAFE = peri-appendiceal fat echogenicity.
p value has been bolded if p < 0.05.
Diameter = maximal outer diameter of the appendix.
Sensitivity, Specificity, and Predictive Values of Potential Risk Factors of Complicated Appendicitis
CI = confidence interval; PPV = positive predictive value; NPV = negative predictive value; PAFE = peri-appendiceal fat echogenicity.
The best PPV, NPV, and accuracy were bolded.
Diameter = Maximal outer diameter of the appendix.
Discussion
Thanks to the rapid advances in imaging technology and the increasing expertise of pediatric radiologists, pre-operative diagnosis of AA is now possible in most cases, thanks to ultrasound visualization of the appendix. Accordingly, secondary ultrasound signs including increased PAFE and peri-appendiceal free fluid, or direct signs primarily a MOD of the appendix exceeding 6 mm, have been accepted by most authors as being radiologic signs suggesting appendicitis.26–32 Ultrasonography has gained increasing importance, and is now the reference examination method for investigating children's right lower quadrant pain. Ultrasound is a simple, radiation-free, non-invasive diagnostic tool that may be repeatedly used without distress to the child.
Our study demonstrated that a diagnostic accuracy of 92% for acute appendicitis was achieved using ultrasound. Our results are consistent with literature data confirming the outstanding accuracy of ultrasound for the diagnosis of AA in children, with sensitivities ranging from 85% to 100% and specificities ranging from 89% to 98%.14,21,33,34 In our study, ultrasound accuracy was similar to those reported by Tong et al., 18 Goldin et al., 35 and Binkovitz et al., 33 which were 89%, 92.2%, and 96%, respectively.
The ultrasound diagnostic accuracy of 92% was achieved for appendix diameter of ≥6.5mm. The 7 mm cutoff value for appendiceal MOD on ultrasound also provided a high accuracy of 91%. Nevertheless, we preferred the 6.5 mm cutoff value not only because of its slightly higher accuracy, but also because of its higher NPV, allowing an additional 3% reduction in negative appendectomies. These results are in agreement with previous findings, underlining the need to revise the sonographic criteria previously used to diagnose AA in children.17–20
In their study including 320 pediatric patients with suspected AA, Chicaiza et al. 17 concluded that the optimal MOD of the appendix should be 7 mm rather than 6 mm as currently accepted. In an interesting study including 304 consecutive pediatric patients, Goldin et al. 35 compared the effectiveness of ultrasound versus CT for diagnosing appendicitis in the pediatric population. The authors reported lower sensitivity and specificity of ultrasound compared with CT, when using MOD of the appendix greater than 6mm as the diagnostic criterion. The authors concluded that, with a better definition of sonographic criteria, ultrasound would have a diagnostic accuracy similar to CT for the diagnosis of AA in children. Goldin et al. 35 proposed the use of a MOD of the appendix at or above 7.5 mm associated with at least one secondary sign on ultrasound to make the diagnosis of appendicitis. These results, in line with our own, are bound to have major implications in our day-to-day practice. Indeed, improving ultrasound accuracy for diagnosing appendicitis would decrease the negative appendectomy rate and reduce the need for CT scans, sparing our patients unnecessary radiation.
This study suggests that the cutoff value for appendiceal MOD on ultrasound should be 6.5 mm rather than the currently accepted 6 mm. These data highlight an important concept, namely the need to find the best way to use healthcare dollars while maximizing patient care. Although there are costs related to imaging, most authors agree that ultrasound helps saving hospital resources in terms of reduced hospital days, thanks to fewer negative appendectomies and fewer patients admitted for observation. Indeed, ultrasound is favorably comparable to in-hospital observation, CT scanning, and anesthesia regarding cost-effectiveness, risk of a negative appendectomy, diagnostic delay leading to perforation, and radiation exposure.21,28,35–37
Interestingly, none of our patients with appendiceal diameter <6 mm and lack of peri-appendiceal free fluid on ultrasound was found to have AA. Our findings are consistent with those of previously published research highlighting the important contribution of secondary ultrasound features, including peri-appendiceal free fluid, probe sensitivity, and increased PAFE, in enhancing the accuracy of ultrasonography for diagnosing appendicitis in children.18–22 The healthy appendix is a structure that is tubular, compressible, and blind ending. The normal appendix is usually defined as having a MOD of no more than 6 mm, which is the key criterion for ruling out AA. 27 We believe that our results are crucial in providing a definitive diagnosis, especially in patients with low clinical suspicion of AA, and in those under five years of age. In daily practice, we are often asked to rule out appendicitis in pre-school children, which can be challenging. Pre-school children cannot readily locate their pain, and their physical examination is often challenging. Moreover, AA is quite rare at this age. 38
This study showed that the sonographic sign giving the best ultrasound accuracy for diagnosing CA, which was 68%, was an appendix diameter ≥9 mm. In their study including 934 pediatric patients with suspected AA, Tong et al.18 found that the presence of specific sonographic signs, including appendicolith, appendiceal diameter >10.1 mm, and peri-appendiceal fluid can aid diagnosis and differentiation of SA and CA. Unlike these data, Gonzalez et al., 39 in a large series of 1,027 children undergoing appendectomy for suspected AA, concluded that ultrasound is not a reliable tool for assessing the presence of appendicolith, CA, or abscess. Based on our results and data from the literature, we believe that the accuracy of ultrasound for the diagnosis of complicated appendicitis in children is moderate.
Although this study has its strengths, it does have some limitations. First, our study was monocentric and conducted in a tertiary care hospital, which may restrict the generalizability of our findings. Second, ultrasound scans were performed and analyzed by radiologists of varying skill levels, including five seniors and five residents. To minimize any variability in interpretation, we specified in the ultrasound order what data should be included in the final ultrasound report. In addition, we ensured that all ultrasound examinations performed during nights and weekends were reviewed and approved by the senior radiologist before the final report was written. Another limitation of our study was that some patients with suspected appendicitis may have been referred to other institutions. Last, the diagnosis of non-appendicitis in non-operated patients was reached without pathologic evidence.
Conclusions
In conclusion, our present study demonstrated that appendiceal MOD ≥6.5 mm is the gold standard for diagnosing AA in pediatric patients. The combination of an appendiceal diameter <6 mm and the lack of peri-appendiceal free fluid on ultrasound would rule out AA. We believe that these findings would be of great value in establishing a more accurate diagnosis of AA in children, minimizing the need for abdominal CT scans and, ultimately, decreasing the negative appendectomy rate.
Footnotes
Authors' Contributions
Conceptualization: Zouari. Project administration: Zouari. Writing—original draft: Zouari. Writing—review: Zouari. Data curation: Hbaieb, Issaoui, Krichen.
Methodology: Hbaieb, Issaoui, Krichen. Supervision: Safi, Ben Dhaou, Mhiri.
Validation: Safi, Ben Dhaou, Mhiri. Guarantor: Zouari.
Funding Information
The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Author Disclosure Statement
We, the authors, have no financial or personal relations with other people or organizations that could potentially and inappropriately influence our work and conclusions.