
Abstract
Background:
Management of complicated intraabdominal infections (cIAIs) requires containment of the source and appropriate initial antimicrobial therapy. Identifying the local data is important to guide the empirical selection of antimicrobial therapy. In this study, we aimed to describe the pathogen distribution and antimicrobial resistance of cIAI.
Methods:
In two major tertiary care hospitals in Egypt, we enrolled patients who met the case definition of cIAI from October 2022 to September 2023. Blood cultures were performed using the BACTAlert system (BioMerieux, Marcy l’Etoile, France). A culture of aspirated fluid, resected material, or debridement of the infection site was performed. Identification of pathogens and antimicrobial susceptibility testing were conducted by the VITEK-2 system (BioMerieux, Marcy l’Etoile, France). Gram-negative resistance genes were identified by PCR and confirmed by whole bacterial genome sequencing using the Nextera XT DNA Library Preparation Kit and sequencing with the MiSeq Reagent Kit 600 v3 (Illumina, USA) on the Illumina MiSeq.
Results:
We enrolled 423 patients, 275 (65.01%) males. The median age was 61.35 (range 25–72 years). We studied 452 recovered bacterial isolates. Gram-negative bacteria were the vast majority, dominated by E. coli, followed by Klebsiella pneumoniae, Pseudomonas aeruginosa, Acinetobacter baumannii, and Proteus mirabilis (33.6%, 30.5%, 13.7%, 13%, and 5.4%, respectively). High rates of resistance were detected to third- and fourth-generation cephalosporins and fluoroquinolones. No resistance was detected to colistin. Resistance to amikacin and tigecycline was low among all isolates. Resistance to meropenem and ceftazidime/avibactam was moderate. ESBL genes were common in E. coli and K. pneumoniae. CTX-M15 gene was the most frequent. Among Enterobacterales, blaOXA-48 and blaNDM were the most prevalent carbapenemase genes. Pseudomonas aeruginosa isolates harbored a wide variety of carbapenemase genes (OXA, NDM, VIM, SIM, GIM, SPM, IMP, AIM), dominated by metallo-beta-lactamases. In 20.6% of isolates, we identified two or more resistance genes.
Conclusion:
High resistance rates were detected to third- and fourth-generation cephalosporins and fluoroquinolones. Amikacin and tigecyclines were the most active antimicrobials. Our data call for urgent implementation of antimicrobial stewardship programs and reinforcement of infection control.
Introduction
Intraabdominal infections (IAIs) are a major cause of morbidity and mortality and are among the most common causes of severe sepsis in the intensive care unit (ICU). 1 In addition to significant morbidity and mortality for patients, they consume substantial hospital resources. IAIs encompass uncomplicated intramural infection of the gastrointestinal tract and complicated IAIs (cIAIs), where the infectious process extends beyond the source organ and causes either localized peritonitis or diffuse peritonitis.
The cIAIs are also classified into community-acquired infections (CAIs), which include infections present on admission or detected less than 48 hours after admission, and healthcare-associated infections (HAIs), which manifest more than 48 hours after admission or after surgical or invasive procedures. 2 For surveillance purposes, a recent classification by the Centers for Disease Control National Healthcare Safety (CDC/NHSN) has been used depending on whether infection is evident at the time of surgery. 3
Management of cIAI depends on early diagnosis, source control, and proper selection of antimicrobials.4–6 Misuse of antimicrobial agents may result in suboptimal treatment and encourage the selection and spread of antibiotic-resistant microorganisms in the healthcare setting. 6
The most common causative agents of IAIs are gram-negative bacteria (GNB), in particular Escherichia coli (E. coli) and Klebsiella species. 7 These bacteria can produce extended-spectrum beta-lactamases (ESBLs), which can confer resistance to a wide range of antibiotics. 8 ESBL-producing Enterobacterales are a major cause of healthcare-associated infections.9,10 Recent cases of IAI caused by ESBL-producing E. coli have been reported.9,10
The enhanced widespread resistance of microorganisms causing cIAI infections highlights the importance of monitoring the antimicrobial susceptibility patterns of these bacteria.11,12
To our knowledge, publications on cIAI from Egypt are sparse, and no studies have identified the pathogens causing cIAI and their resistance pattern. Identifying the local data is important to guide the empirical selection of antimicrobial therapy, especially for patients with cIAI with sepsis.
In this study, we aimed to describe the pathogen distribution of cIAIs and their antimicrobial resistance.
Materials and Methods
Methods
This study was conducted in two major tertiary care hospitals in Egypt from October 2022 to September 2023. One of the participating institutions was a teaching hospital with 400 bed capacity and the second was a tertiary general hospital with 250 bed capacity. Both hospitals included active General Surgery, Oncology Surgery, and Emergency Surgery departments. Both are in Cairo, Egypt. The Ethics Committee of the Faculty of Medicine, Cairo University approved the study. All patient data and specimens were de-identified to maintain patient privacy.
Inclusion criteria and case definition
We enrolled patients who met the National Healthcare Safety Network (CDC/NHSN) Case definitions of cIAI, 2023,
13
which meet at least one of the following criteria:
Patients have organism(s) identified from an abscess or purulent material from the intraabdominal space by a diagnostic culture or nonculture-based microbiologic testing method. The patient has an abscess or other evidence of IAI on gross anatomic or histopathologic examination and an intraabdominal organism(s) identified by a diagnostic blood culture. The patient has at least two of the following clinical signs: fever (>38.0°C), hypotension, nausea, vomiting, abdominal pain or tenderness, elevated transaminase level(s), or jaundice, and at least one of the following:
Organisms seen on Gram stain and/or identified from intraabdominal fluid or tissue obtained during an invasive procedure or from an aseptically placed drain in the intraabdominal space by a diagnostic culture- or nonculture-based microbiologic testing method An intraabdominal organism(s) identified from a diagnostic blood culture and imaging test is definitive for infection or equivocal but supported by clinical correlation, specifically, physician documentation of antimicrobial treatment for IAI. Postoperative IAI refers to the clinical manifestations of IAI within 30 days of surgery, with laboratory tests and imaging confirming IAI or drainage fluid confirming the presence of an intraabdominal abscess.
14
We excluded patients with incomplete data and patients who had an alternative diagnosis.
Patient evaluation and resuscitation
Initial evaluation by routine history, physical examination, imaging, and laboratory investigations was performed. On clinical examination, a risk assessment was done on patients according to the Surgical Infection Society (SIS) guidelines 4 to identify them as being at either lower or higher risk for treatment failure or death and as having either a community-acquired IAI or a healthcare or hospital-associated IAI for purposes of planning source control and empirical antimicrobial therapy. Managing sepsis started early, with fluid resuscitation.
According to published guidelines of the Surgical Infection Society revised guidelines on the management of IAIs (2017), the WSES/GAIS/SIS-E/WSIS/AAST global clinical pathways for patients with IAI (2021) and the Canadian practice guidelines for surgical IAIs, a source control procedure to drain infected foci, control ongoing peritoneal contamination, and restore anatomical and physiological function was performed for all patients.4–6
Diagnosis
The diagnosis was performed clinically and by imaging according to the routine standard of care. The laboratory specimens were collected from all patients enrolled in the study intraoperatively, for epidemiological purposes,4,5 and the specimens were classified according to the time and place of the infection acquisition into healthcare associated (healthcare-associated, manifests after more than 48 hours of hospitalization, or after surgical or invasive procedures) and community acquired (present on admission or detected less than 48 hours of admission).
Laboratory methods
Routine laboratory tests were performed in the hospital’s clinical laboratory service. Microbiological culture methods were performed using the Clinical Laboratory Standards Institute methods. 15
Aerobic and anaerobic blood cultures were performed using BACTAlert blood culture bottles and systems (BioMerieux, Marcy l’Etoile, France). A culture of aspirated fluid or resected material or debridement of the infection site was performed on blood agar, chocolate agar, MacConkey agar, and Sabouraud Dextrose agar. Resected tissues were additionally incubated with enrichment broth to enrich pathogens. Potassium hydroxide preparations were used with excised tissues to identify fungal elements. Identification of pathogens and antimicrobial susceptibility testing were performed by the VITEK-2 system (BioMerieux, Marcy l’Etoile, France) and interpreted according to the CLSI guidelines, 2023. 15 Susceptibility to colistin was tested by broth microdilution according to CLSI, 2023 methods. 15
Molecular analysis and characterization
Identification of the resistance genes was performed by molecular methods in the Kasr Alainy Molecular Microbiology and Sequencing Reference Laboratory using PCR, 16 and the results were further confirmed by DNA sequence analysis, whole bacterial genome sequencing using the Nextera XT DNA Library Preparation Kit and sequencing with the MiSeq Reagent Kit 600 v3 (Illumina, USA) on the Illumina MiSeq, generating, on average, 301 base pair paired-end reads. 17 Molecular characterization detected most ESBL, carbapenemases, and AmpC genes. We identified ESBLs (class A), blaTEM, blaSHV, blaCTX-M, blaVEB, blaPER, and blaGES; and blaAmpC β-lactamase genes (class C), including blaCMY-II, blaDHA, and blaACT-Type. blaMOX; and carbapenemases (class A)—blaKPC; (class B)—blaNDM, and blaVIM; and (class D)—blaOXA-48-like.
Results
Demographic criteria
We enrolled 423 patients, 275 (65.01%) males and 148 (34. 99%) females. The median age was 61.35 (range 25–72 years). Most infections were healthcare-associated (62.6%). Table 1 describes the main source of infection in the 423 patients. Some infections were polymicrobial, so the number of studied isolates was 452.
Frequency Distribution of Complicated Intraabdominal Infections According to the Source of Infection
The frequency distribution (%) of pathogens from 423 patients is presented in (Fig. 1):
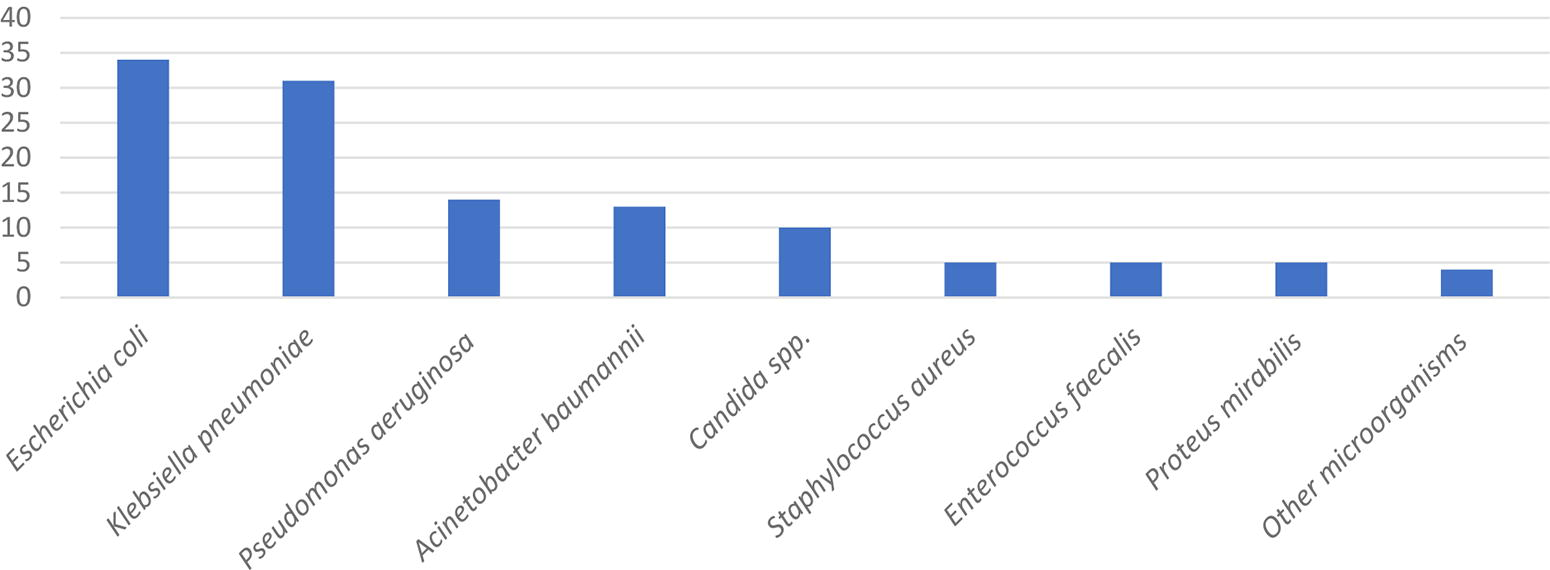
Frequency distribution % of pathogens from 423 patients.
Out of the 452 bacterial isolates recovered from 423 patients, gram-negative bacteria were the vast majority; the most frequently identified pathogens were E. coli, followed by Klebsiella pneumoniae, Pseudomonas aeruginosa, Acinetobacter baumannii, and Proteus mirabilis (33.6%, 30.5%, 13.7%, 13%, and 5.4%, respectively). Gram-positive cocci included Staphylococcus aureus and Enterococcus faecalis (5.4% each). Candida species were isolated in 9.5%. Ninety percent of Staphylococcus aureus were methicillin resistant. All Enterococcus faecalis isolates were vancomycin sensitive. Candida species were dominated by C. albicans (74.4% of the Candida isolates). Streptococcus spp. and Bacteroides spp. were isolated from a small number of patients and were reported under other bacteria. Blood culture was used to diagnose secondary bacterial infections and identify the pathogens and their susceptibility. Blood culture was positive in 43 patients, and the blood isolates were the same as the cIAI isolates of the corresponding patients.
Antimicrobial resistance of isolated gram-negative bacteria
The antimicrobial resistance profile of the cIAI pathogens is shown in Table 2. Colistin susceptibility was tested by broth microdilution according to CLSI, 2023. 15 Our study did not identify colistin-resistant isolates with MIC >4 µg/mL. 15 All isolates had MIC less than 2 µg/mL and were reported as intermediate in Table 2. Resistance to amikacin and tigecycline was low among all isolates. Resistance to meropenem and ceftazidime/avibactam was moderate among most microorganisms, except for high resistance by Acinetobacter baumannii. In contrast, high rates of resistance were detected in third-generation cephalosporins (ceftazidime and ceftriaxone), fourth-generation cephalosporins (cefepime), and fluoroquinolones (ciprofloxacin and levofloxacin).
Antimicrobial Resistance % of Common Complicated Intraabdominal Isolates
In the study, the level of resistance was determined as low when from 0to 30% (green color), moderate from 31 to 45% (yellow color), and high when more than 45% (red color).
Ak, amikacin; AZT, aztreonam; FEP, cefepime; CAZ, ceftazidime; CRO, ceftriaxone; CIP, ciprofloxacin; CST, colistin; C/T, ceftolozane/tazobactam; CZA, ceftazidime/avibactam; IMP, imipenem; LEV, levofloxacin; MEM, meropenem; TGC, Tigecycline.
Molecular identification of resistance genes
Table 3 shows the distribution of ESBL genes of the TEM, SHV, and CTX-M types. E. coli and K. pneumoniae were the most common ESBL-producing isolates. CTX-M15 was the most frequent.
Types and Frequency Distribution % of ESBL Genes among Common cIAI Pathogens
cIAI, complicated intraabdominal infections; ESBL, extended-spectrum beta-lactamases.
Table 4 shows the genes encoding carbapenem resistance. Among Enterobacterales, blaOXA-48 and NDM were the most prevalent. Pseudomonas aeruginosa isolates harbored a wide variety of carbapenemase genes (OXA, NDM, VIM, SIM, GIM, SPM, IMP, AIM), dominated by metallo-β-lactamases.
Types and Frequency Distribution % of Carbapenemase Genes among Common cIAI Pathogens
cIAI, complicated intraabdominal infections.
Table 5 shows that AmpC genes were detected in 16% of E. coli (CMY-II, 15% and DHA-1, 1%), in 4% of Klebsiella pneumoniae (1% CMY-II and 3% DHA-1), and 33% of Proteus isolates (all CMY-II).
Types and Frequency Distribution % of AmpC Genes among Common cIAI Pathogens
cIAI, complicated intraabdominal infections.
The coexistence of multiple genes among IAI isolates
Among 452 isolates, we detected 20.6% coidentification of two or more resistance genes (Fig. 2).

Bar graphs summarizing the percentages of coexistence of resistance genes among all the studied isolates.
Discussion
Initial source control and appropriate antimicrobial therapy are predictors of survival and microbiological cure. In contrast, initial inappropriate antimicrobial therapy and inadequate source control are confirmed predictors of mortality in patients with complicated IAIs.18–20 If safe, shorter antibiotic duration after source control is preferred to minimize drug-related adverse events, the selection of antibiotic-resistant mutants, and costs. In the Study to Optimize Peritoneal Infection Therapy (STOP-IT) short-course antimicrobial therapy for abdominal infection after source control proved to be both safe and effective. 21
The microbiology of cIAI is well described in the literature. It consists mainly of Enterobacterales, with E. coli being the leading organism, followed by Klebsiella spp., other Enterobacterales, Pseudomonas spp., Enterococci, anaerobes, and Candida species. 22 As the rate and mechanism of antimicrobial resistance among these organisms differ from one geographic area to the other, we studied the local pathogen distribution and antimicrobial resistance of 423 cIAI patients to provide data that guide the empirical selection of antimicrobials.
Peritoneal abscesses accounted for 20.8% of cIAIs, which is less than previous reports,20,23 which identified peritoneal abscesses in more than 50% of their patients. The reason for the diversity of the results is likely due to differences in patient inclusion criteria.
Gastrointestinal cancers were among the most common sources of cIAI in our patients. Despite unremitting enhancement in surgical techniques, anastomotic leaks and intraabdominal abscesses are still among the serious complications of colorectal cancer operations. Moreover, postoperative IAI after colorectal cancer resection was identified as an independent prognostic factor for local recurrence-free survival. 24
Postoperative IAI is an important type of cIAI, accounting for approximately 8.5% of total IAIs, and its mortality rate is as high as 22%−55%.16,25,26 In our patients, this group accounted for 16.3%. As healthcare-associated infections, they are commonly caused by resistant organisms especially in endemic areas and hospitals. This may reduce the chance of prompting an effective primary antimicrobial regimen, thereby increasing both mortality and costs. 25
Hepatocellular carcinoma was among the sources of cIAI in our patients. This is in keeping with a recent report of positive blood culture in 20% after ablation therapy for hepatocellular carcinoma. Twenty-four out of 100 patients had abnormally high procalcitonin levels. 27
cIAIs caused by appendicitis were relatively uncommon, accounting for 6.9%, in keeping with the 5.6% report by Yoon et al. (2019). 28 However, it was lower than several studies reporting complicated appendicitis in 50% or more of IAIs.29–32
Although the sources of cIAI were variable, gram-negative bacteria were by far the most prevalent, and they showed high rates of resistance to antimicrobials. The most common pathogens isolated from cIAI were E. coli (33.6%), Klebsiella pneumoniae (30.5%), Pseudomonas aeruginosa (13.7%), Acinetobacter baumannii (13%), and Proteus mirabilis (5.4%). Reports of IAI from Egypt are sparse. One retrospective study identified IAI complicating cesarean section at a rate of 2.87%, without the identification of pathogens. 33
Our results are in broad agreement with reports from Lebanon and Jordan, derived from the Study for Monitoring Antimicrobial Resistance Trends (SMART), in which prospective data were collected from IAI in different medical centers across Jordan and Lebanon between 2011 and 2013. 34 E. coli, K. pneumoniae, and Pseudomonas aeruginosa were the most frequent species among the 527 IAI-associated isolates (46%, 14%, and 12%, respectively). ESBL rates were 49% and 56% among their E. coli and Klebsiella pneumoniae IAI isolates, respectively.
Our results are in accordance with international reports that Enterobacterales were the major pathogens involved in cIAI.12,28,35,36
The resistance rates to antimicrobial agents commonly used for perioperative antibiotic prophylaxis and the treatment of cIAI were extremely high, limiting the effectiveness of cephalosporins and fluoroquinolones. The most active antimicrobials were amikacin, tigecycline, and colistin, followed by meropenem, ceftolozane/tazobactam, and ceftazidime/avibactam.
Tigecycline, alone and in combination, achieved favorable clinical response rates in patients with cIAI with high severity of illness. 37 Our results confirm previous publications on the high rates of antimicrobial resistance in Egypt38,39 and other countries.40–42
Interestingly, multidrug-resistant (MDR) bacteria, including methicillin-resistant Staphylococcus aureus, extended-spectrum beta-lactamase-producing Enterobacterales, carbapenemase-producing Klebsiella pneumoniae, and carbapenem-resistant Acinetobacter baumannii (CRAB), are common in IAIs.43–45 The escalating spread of ESBLs and carbapenemase-mediated resistance has been reported globally in both hospital and community infections. 46
In our study, ESBL-producing isolates carrying CTX-M15 accounted for 73.3% of Klebsiella and 75.3% of E. coli, while CTX-M14 was detected in 24.4% of Klebsiella and 5.5% of E. coli. Among the CRE, carbapenemase genes of blaOXA-48 and MBL were the most prevalent carbapenemase genes, especially in K. pneumoniae isolates. In contrast, AmpC genes were less frequently detected. Our results are in keeping with results from the SMART study, which revealed global high resistance rates among cIAI isolates.11,34,47
We confirmed previous reports from Egypt by El-Kholy et al. (2020) 38 that showed a high prevalence of ESBL and carbapenem resistance in Egypt, representing 54% and 13.8% of E. coli isolates compared with 42.5% and 48.1% in K. pneumoniae isolates, respectively.
Previous studies showed that TEM-type and SHV-type enzymes and CTX-M-type enzymes were widely disseminated worldwide and that blaCTX-M-15 and blaCTX-M-14 were the most commonly identified genes encoding CTX-M enzymes and can be horizontally mobilized by various genetic elements.34,38,42,48,49
Coharboring of multiple ESBL genes was reported previously in Egypt46,50,51 and some other countries, including Burkina Faso, 52 Qatar, 53 and Iran. 54
The variations in antimicrobial use in human beings and animals and adherence to infection control guidelines may explain the differences in the rates of antimicrobial resistance and predominant types of resistance genes among healthcare facilities within the same country, as well as between institutions from different countries. Selection of empirical antibiotics for the treatment of cIAI is a challenge in settings with high rates of AMR and a high prevalence of multidrug-resistant pathogens. Hence, empirical antimicrobial therapy should be on the basis of local epidemiology, individual patient risk factors for MDR pathogens, clinical severity of infection, and the infection source. The most important factor in predicting the presence of resistant pathogens in cIAIs is acquisition in a healthcare setting, in patients with a history of hospitalization, comorbidities, corticosteroid use, and previous antimicrobial therapy.4,5
Initial antimicrobial regimens with a broad spectrum of activity are recommended in settings with high rates of AMR because adequate empirical therapy is important to reduce mortality. 25
Rapid diagnostics for identification of the pathogens and their AMR profile will allow early de-escalation of antimicrobial therapy, and the earlier transitions from empirical to pathogen-specific regimens. The enhanced utilization of rapid diagnostic testing, and the implementation of antimicrobial stewardship programs will optimize antimicrobial drug prescription and control antimicrobial resistance. 55
One limitation of our study is that the participating hospitals were major tertiary hospitals receiving complicated cases, and referrals from other hospitals, which could explain the high rates of AMR.
Conclusion
The gram-negative pathogens were the most frequent pathogens of cIAI in our institutions. The pathogens showed high rates of resistance to commonly used antimicrobials for perioperative prophylaxis and treatment of cIAI. We identified amikacin, tigecycline, and colistin as the most active in our institutions, followed by meropenem and ceftazidime/avibactam. The study underscores the need to address the current empirical antibiotic options to cover the predominant antimicrobial-resistant pathogens, until culture results are available. We recommend the use of rapid diagnostics for the timely identification of pathogens and their susceptibility to antimicrobials and provide timely results to support the management of patients with cIAI. The high rate of ESΒLs and CRE in our institutions and Egypt calls for urgent control of antimicrobial use in human and animal health and in the environment, along with reinforcement of infection prevention and control.
Footnotes
Authors’ Contributions
A.A.E., A.R.E., and M.S.S. carried out the microbiological work on the samples, conducted data analysis, and wrote the article. A.A.H., T.M., and J.A.E. carried out the data analysis, clinical diagnosis, and article writing. I.S.H. and A.S.S. oversaw the clinical diagnosis of the patients and the collection of clinical specimens. All authors read and approved the final article.
Availability of Data and Material
Not applicable
Ethics Approval and Consent to Participate
This research was conducted in accordance with the Ethics Committee of the Faculty of Medicine, Cairo University approved the study. All patient data and specimens were de-identified to maintain patient privacy.
Consent for Publication
Not applicable
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
No specific funding has been provided for this research and the authors receive no financial support for the research, authorship, and/or publication of this article.