
Abstract
Objective:
This study aims to evaluate the predictive value of neutrophil−lymphocyte ratio (NLR) in determining infection after orthopedic surgery.
Methods:
A comprehensive search was conducted in PubMed, EBASE, CNKI, and Wanfang databases to identify relevant studies. The quality of the included studies was assessed using QUADAS-2. Data extraction was performed to calculate sensitivity, specificity, and other indicators. Bivariate mixed-effects meta-analysis was conducted using Stata software. The sources of heterogeneity were evaluated, and a summary receiver operating characteristic curve was generated.
Results:
A total of 16 literatures comprising 18 studies involving 3737 patients were included in this analysis. NLR demonstrated moderate sensitivity (0.77) and specificity (0.69) in diagnosing orthopedic post-operative infection, with an area under the curve of 0.80 and diagnostic odds ratio of 7.76. Significant heterogeneity was observed among the studies, primarily due to variations in surgical type, infection type, blood test timing, and NLR cutoff value. Fagan nomogram indicated that NLR could increase the positive posterior probability to 72% and decrease the negative posterior probability to 25%. The pooled effect of the likelihood ratio dot plot for diagnosis fell in the lower right quadrant. Deek funnel plot suggested no publication bias in this study.
Conclusion:
NLR holds certain value in diagnosing infection after orthopedic surgery and can provide additional information to assess the risk of infection. However, its predictive performance is influenced by various factors, and it cannot be used as a sole criterion for confirming the diagnosis. Prospective studies should be conducted in the future to optimize the diagnostic threshold and explore its combination with other indicators.
Orthopedic surgery is a common and important treatment for bone diseases. Although modern orthopedic surgical techniques and anti-infection measures have made significant progress, orthopedic post-operative infection is still one of the most common complications. Epidemiological survey showed that the incidence of post-operative infection accounted for 36% of the total incidence of nosocomial infection, of which orthopedic post-operative infection accounted for 1%−3%. 1 Different types of orthopedic surgery have different post-operative infection rates. The post-operative infection rate of closed internal fixation surgery is 5%−20%, whereas the post-operative infection rate of open fracture can reach more than 30%. 2 Post-operative infection increases the labor volume and work intensity of medical staff, threatens the physical health and life safety of patients, resulting in poor effect in the later stage of rehabilitation treatment, prolonged hospitalization, and greater economic pressure on patients, as well as a waste of precious medical resources. 3 Therefore, timely and accurate diagnosis and treatment of infection after orthopedic surgery are essential for the rehabilitation of patients. 4 Currently, although several diagnostic criteria and guidelines have been proposed for infection after orthopedic surgery, the accuracy of diagnosis and early detection remain a challenge. Therefore, it is of great clinical significance to find a simple and reliable index to assist the diagnosis of infection after orthopedic surgery.
In recent years, inflammatory markers have been widely studied and applied in the diagnosis of infection.5,6 Neutrophil−lymphocyte ratio (NLR) is one of the simple and easily available indicators. Neutrophils and lymphocytes are one of the most common types of white blood cells in the blood, which play an important role in the body’s immune response. Neutrophils are increased during infection and inflammation, whereas lymphocytes play a key role in anti-inflammation and immune regulation. Therefore, the neutrophil−lymphocyte ratio (NLR) is considered to be an indicator of inflammatory state and immune function. 7 NLR has been widely used in the diagnosis and evaluation of a variety of diseases, such as cancer, cardiovascular disease, and infection.8–12 The rationale is the pattern of changes in neutrophils and lymphocytes during the inflammatory response. Neutrophils are increased during inflammation, whereas lymphocytes are decreased, resulting in an increase in NLR.13,14 Therefore, post-operative NLR is considered to be possibly related to the occurrence and development of infection after orthopedic surgery.
In the past few years, studies on the diagnostic value of NLR in predicting infection after orthopedic surgery have gradually increased.15–30 However, the results of different studies are not consistent, and the sample size is relatively small, which lacks unified conclusions. Therefore, a meta-analysis was necessary to evaluate the true value and clinical application prospects of NLR as a diagnostic indicator of infection after orthopedic surgery by pooling and analyzing the results of existing studies.
Materials and Methods
The search databases included PubMed, EBASE, CNKI, and Wanfang database
English search terms were “NLR, Neutrophil to lymphocyte ratio, Infection, Postoperative.” To avoid missing literature as much as possible, a combination of online and manual retrieval was used to conduct a secondary search of the references provided in the retrieved literature.
Literature inclusion and exclusion criteria
Inclusion criteria
(1) The purpose of literature research included the evaluation of diagnostic value of NLR in predicting infection after orthopedic surgery. (2) NLR samples obtained from peripheral venous blood of patients. (3) The diagnostic criterion was pathogenic examination. (4) Standard and complete four-grid table data (TP, true positive number; FP, false positive number; FN, false negative number; TN true negative number) could be obtained.
Exclusion criteria
(1) Case reports, conference abstracts, letters, reviews, systematic reviews, animal experiments, guidelines; (2) repeated publications with incomplete data; (3) literature with sample size less than 10 cases.
Literature screening and data extraction
Two researchers independently conducted literature search and screening, collected data, and cross-checked results. In case of disagreement, the third researcher was invited to arbitrate. The data extracted included: (1) author, year, country, race, research method, infection site, diagnostic criteria, blood test time, number of cases, male/female ratio, average age and type of surgery; (2) complete four-fold table diagnostic test data, sensitivity, specificity, etc.
Literature quality evaluation
The diagnostic test evaluation tool QUADAS-2 31 was used to evaluate the quality of the literature, and RevMan 5.4.1 software (The Nordic Cochrane Center, The Cochrane Collaboration, London, UK) was used to analyze the risk of bias of the literature. Two researchers independently evaluated and cross-checked the quality of the literature, and a third researcher was invited to arbitrate in case of disagreement.
Statistical methods
Meta-Disc 1.4 software was used to calculate the Spearman rank correlation coefficient between the logarithm of sensitivity and the logarithm of 1-specificity to analyze the threshold effect. Meta-analysis was performed using Stata 12.0 (StataCorp, College Station, TX, USA). Q test and I2 test were used to assess statistical heterogeneity. Meta-regression and subgroup analysis were performed to find the sources of heterogeneity. The pooled sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio, and diagnostic odds ratio (DOR) were calculated by bivariate mixed-effects model (essentially random-effects model), and forest plot, Fagan nomogram, and likelihood ratio dot plot were drawn. The area under the curve (AUC) was calculated and the summary receiver operating characteristic (SROC) curve was fitted and AUC was calculated. Deek’s funnel plot was drawn to visually analyze the publication bias, and sensitivity analysis was used to evaluate the stability of the study. P < 0.05 was considered statistically significant.
Results
Literature retrieval results
According to the abovementioned retrieval scheme and databases, 1924 literatures were initially retrieved, including 1529 literatures in CNKI, 40 literatures in Wanfang database, 180 literatures in PubMed, and 259 literatures in Embase. The titles and abstracts were read after the initial exclusion of 85 duplicate articles, and then 1848 articles that were obviously irrelevant were excluded, and the full texts of the remaining 42 articles were subsequently obtained. Two articles were excluded, and finally 40 articles were carefully read in full text. According to the exclusion criteria, the completeness and accuracy of the content and data were analyzed. Two articles did not use conference abstracts, one letter, one review, three studies that could not calculate relevant data, three and seven studies that were not related to orthopedic post-operative infection and NLR, respectively, and six non-diagnostic studies were excluded. Finally, a total of 16 studies were included in the meta-analysis.15–30 For the literature search and screening process, see Figure 1.
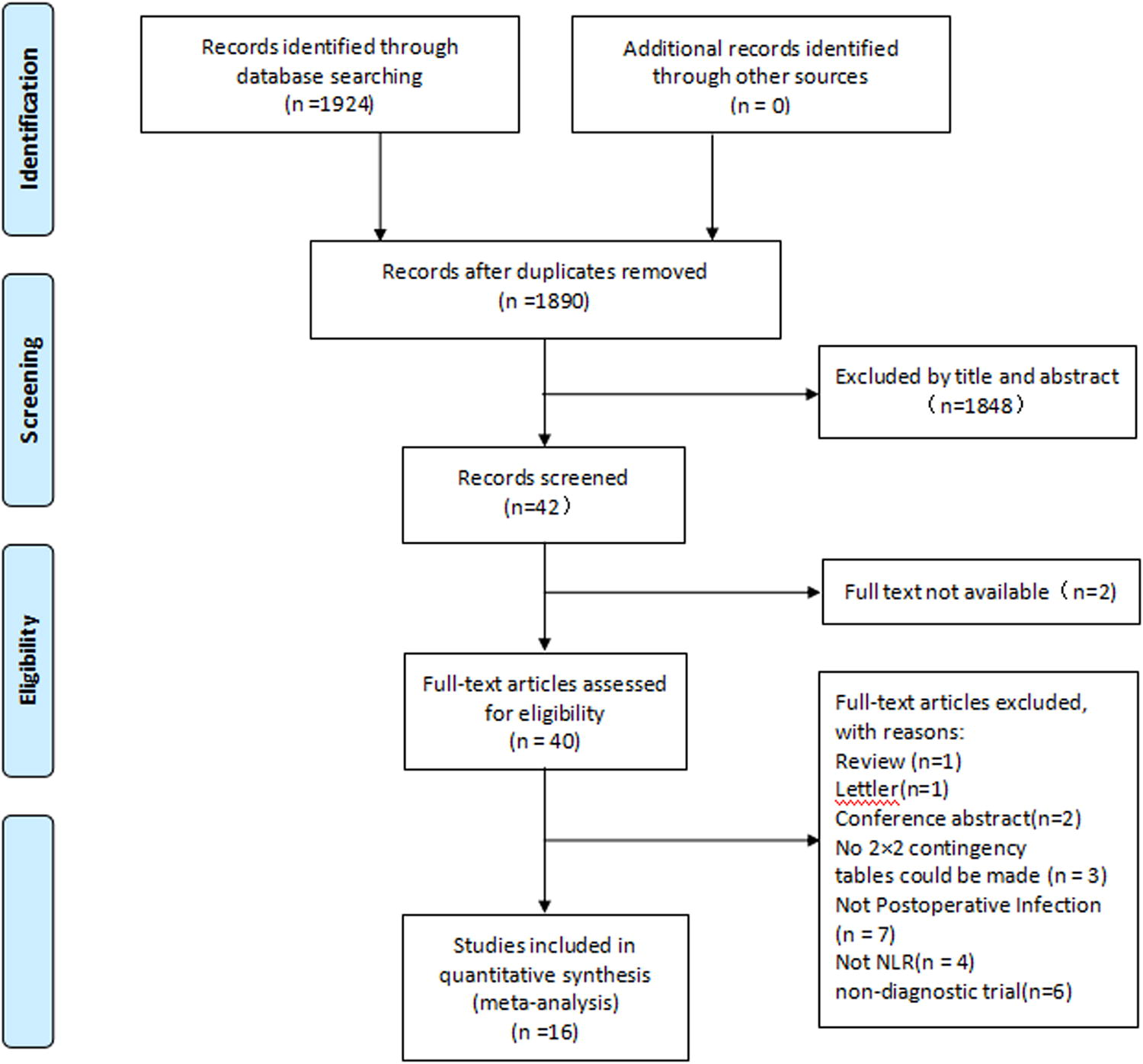
Flow diagram of the study selection for the present meta-analysis.
Basic characteristics of the included literatures
Sixteen relevant literatures were finally included,15–30 including 18 studies with 3737 patients. Among them, there were eight articles in Chinese18–20,24–26,29,30 and eight in English.15–17,21–23,27,28 Thirteen studies focused on Asians16–26,29,30 and three on Caucasians.15,27,28 Except for three articles that did not mention the study type,18,25,30 the rest were retrospective studies. Eight studies focused on artificial joint replacement, including knee replacement and hip replacement,15,19,20,22,23,27,29,30 and three studies focused on spinal surgery.16,17,21 Five studies studied patients who underwent fracture surgery,18,24–26 and one study studied patients who underwent stenosing tenosynovitis, carpal tunnel syndrome, hallux valgus, arthroscopy (shoulder and knee), and severe (fracture reduction). 28 The blood samples were collected after initial surgery, mostly within 1 week after surgery.16–19,21,24–26,28,30 Among them, three studies were collected within 1 day after surgery,18,25,30 two were collected after 1 week after surgery,22,23 and three did not mention the specific collection time point.15,20,27 Most of the studies used medical history combined with etiological examination as the gold standard,15–17,19–23,26,27,29,30 only two studies only relied on etiological examination,24,28 and two studies did not mention the gold standard.18,25 True positive, false negative, false positive, true negative, specificity, sensitivity, and other indicators could be directly obtained or calculated from the included literatures. The basic characteristics of the included literature are detailed in Table 1.
Characteristics of the Included Studies
NA, not available; retro, retrospective; PJI, peri-prosthetic joint infection; SSI, surgical-site infection; FRI, fixation-related infection; MH&EE, medical history combined with etiological examination; EE, etiological examination; Ortho Surg, orthopedic surgery; FX surg, fracture surgery; CRANI, cranioplasty; AP, arthroplasty; SS, spinal surgery; NLR, neutrophil−lymphocyte ratio; Sen, sensitivity; Spe, specificity; AUC, area under the receiver operating characteristic curve.
The results of QUADAS-2
The results of QUADAS-2 showed that there was a certain risk of bias in the 16 included studies in four aspects: case selection, gold standard, trial to be evaluated, case process and progress. Subsequently, we made a bar chart for quality evaluation (Fig. 2A) and a summary chart for applicability of risk bias (Fig. 2B). It can be seen from the figure that most of the included literatures answered “yes,” followed by “unclear” and “no.” The answers of “not clear” and “no” mainly focused on three aspects: case selection, threshold determination, and implementation of the gold standard.
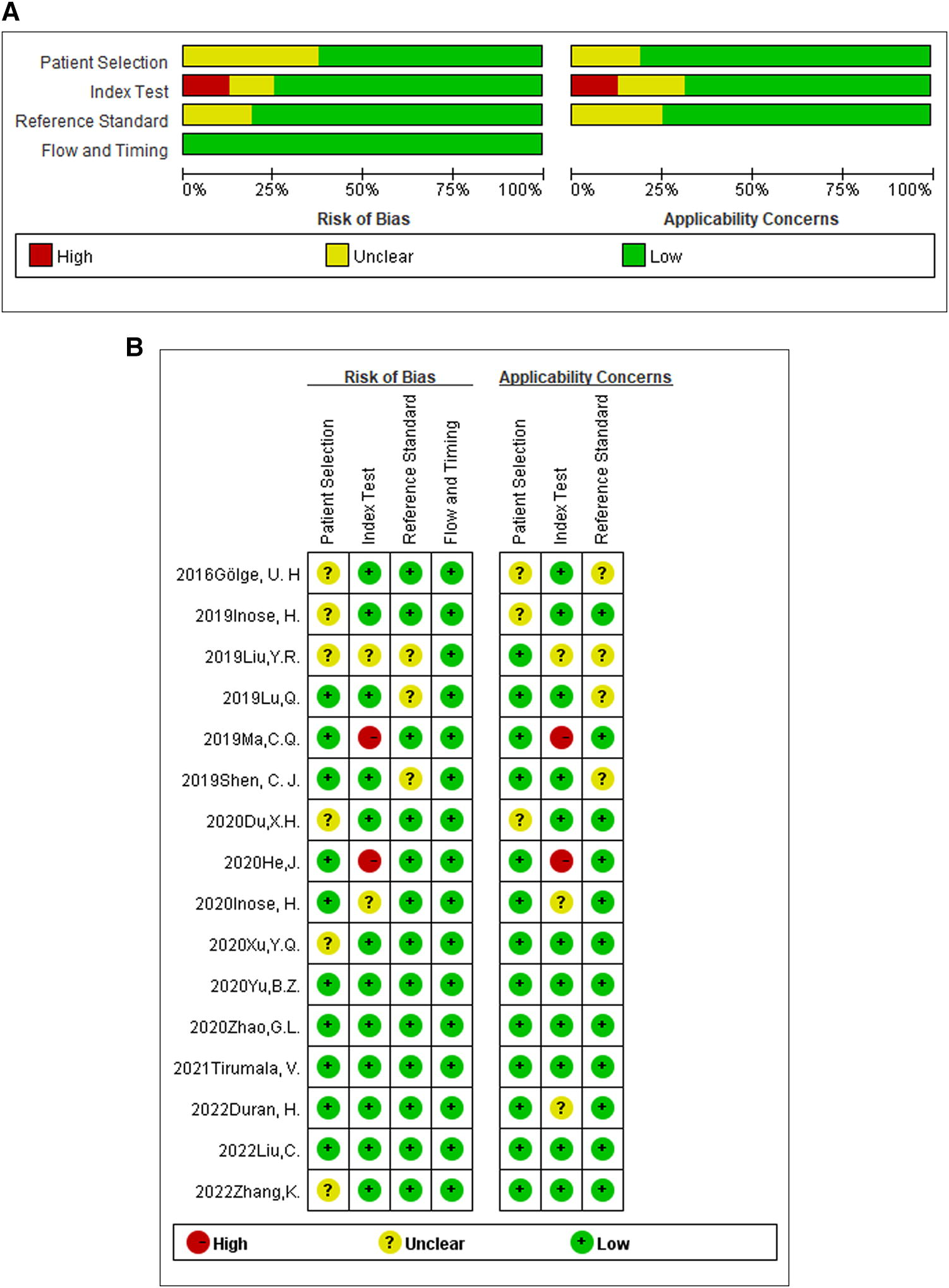
The quality assessment of the included studies by QUADAS-2.
Heterogeneity detection and NLR diagnostic accuracy evaluation
Spearman correlation coefficient in threshold effect analysis was −0.104, P = 0.681 > 0.05, suggesting that the threshold effect was not significant and the data could be combined (Supplementary Fig. S1). In this study, there was heterogeneity in the combined sensitivity and specificity (I2 = 80.31%, I2 = 94.24%), so the random-effects model was selected. Pooled sensitivity was 0.77 (95% confidence interval [CI]: 0.69–0.84), the pooled specificity was 0.69 (95% CI: 0.61–0.77), and the pooled PLR was 2.52 (95% CI: 1.89–3.37). The pooled negative likelihood ratio was 0.32 (95% CI: 0.22–0.47). The DOR was 7.76 (95% CI: 4.20–14.36), and the AUC was 0.80 (95% CI: 0.76–0.83). The forest plots of NLR diagnostic accuracy and SROC are shown in Figure 3 and 4, Supplementary Figures S2 and Supplementary Figure S3.
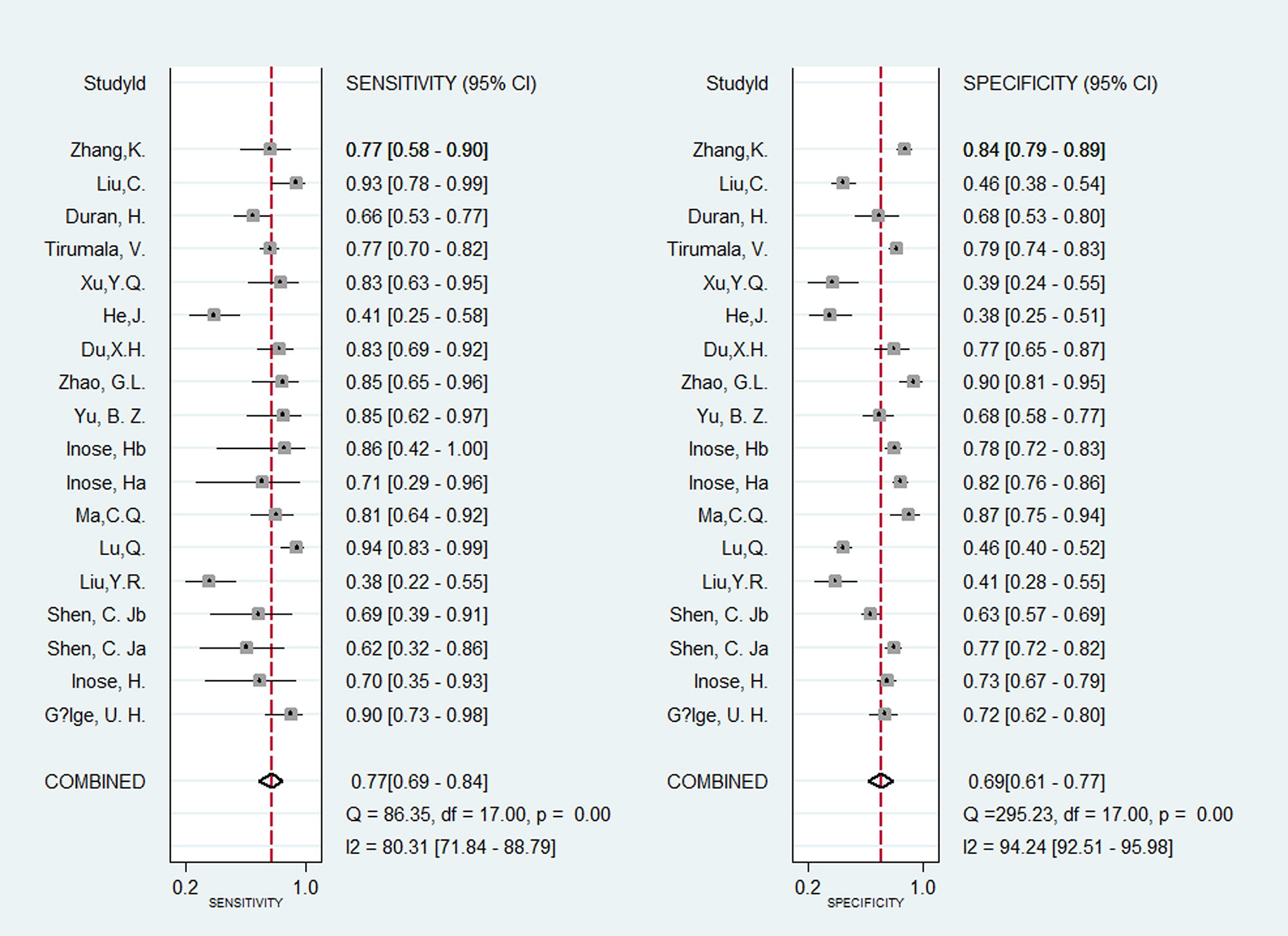
Forest plots of sensitivities and specificities of neutrophil to lymphocyte ratio in the diagnosis of orthopedic post-operative infection.
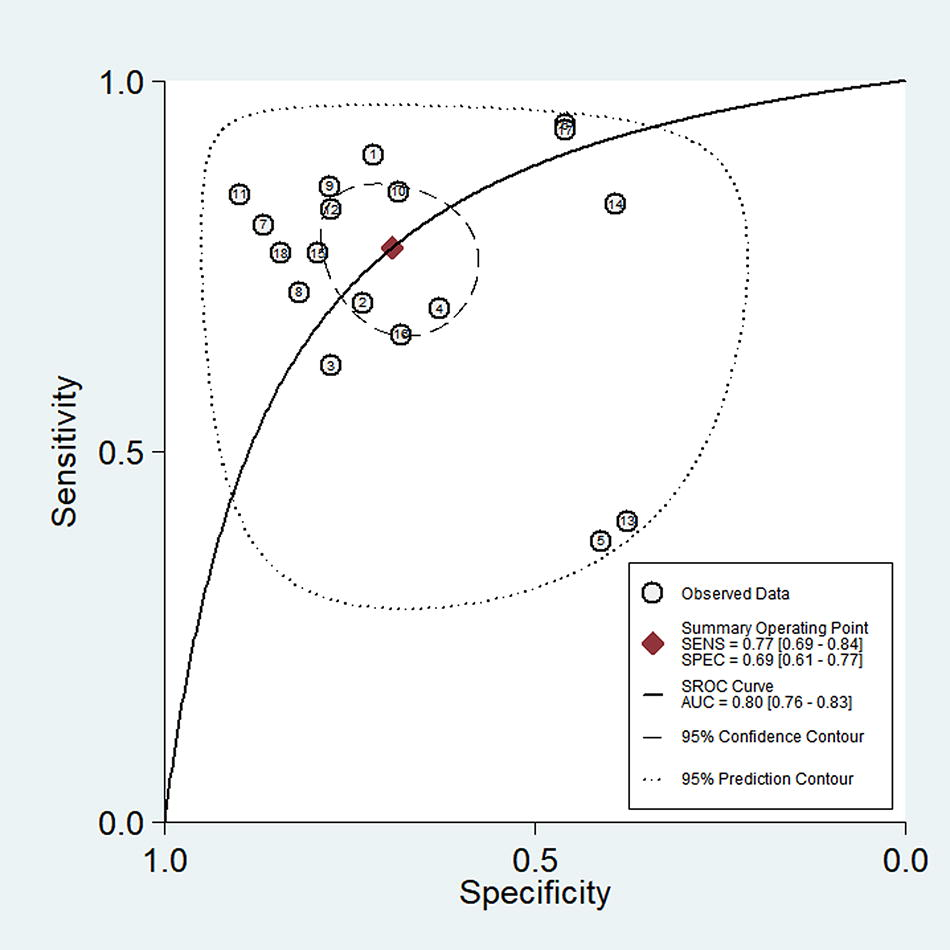
Summary receiver operator characteristic (SROC) showing average sensitivity and specificity estimate of the study results with 95% confidence region. The 95% prediction region represents the confidence region for a forecast of the true sensitivity (SENS) and specificity (SPEC) in a future study. AUC, area under the curve; SROC, summary receiver operating characteristic.
Meta regression and subgroup analysis
Meta regression and subgroup analysis were conducted according to race, study type, infection type, surgery type, gold standard selection, post-operative blood collection time, sample size, gender ratio, and age of patients, and threshold selection. The results showed that the sources of heterogeneity were infection type, surgery type, blood test time, and threshold selection. Further subgroup analysis showed that the sensitivity of NLR in the diagnosis of post-operative infection was significantly reduced when the infection site was SSI and the cutoff value was greater than or equal to 3. Pre-operative detection can improve the specificity of NLR in the diagnosis of post-operative infection. In contrast, the sensitivity and specificity of NLR in the diagnosis of infection after fracture surgery decreased significantly when the NLR was measured before 1 week after surgery. See Supplementary Figure S4 and Supplementary Table S1 for details.
Clinical application evaluation
Fagan’s nomogram was used to evaluate the pre-test probability and post-test probability of NLR in the clinical diagnosis of orthopedic post-operative infection. Fagan nomogram showed that the PLR of the upper slash line was 3, the pre-test probability was set at 50%, and the post-test probability was 72%. The lower slash had a negative likelihood ratio of 0.35; the pre-test probability was set at 50% and the post-test probability at 25%. See Figure 5A for details. The likelihood ratio dot plot can be used to evaluate the clinical application value of diagnostic methods. The results in Figure 5B show that the combined effect of NLR in the diagnosis of infection after orthopedic surgery falls in the lower right quadrant, that is, +LR < 10, −LR > 0.1, indicating that SECT has neither diagnostic nor exclusional capabilities.
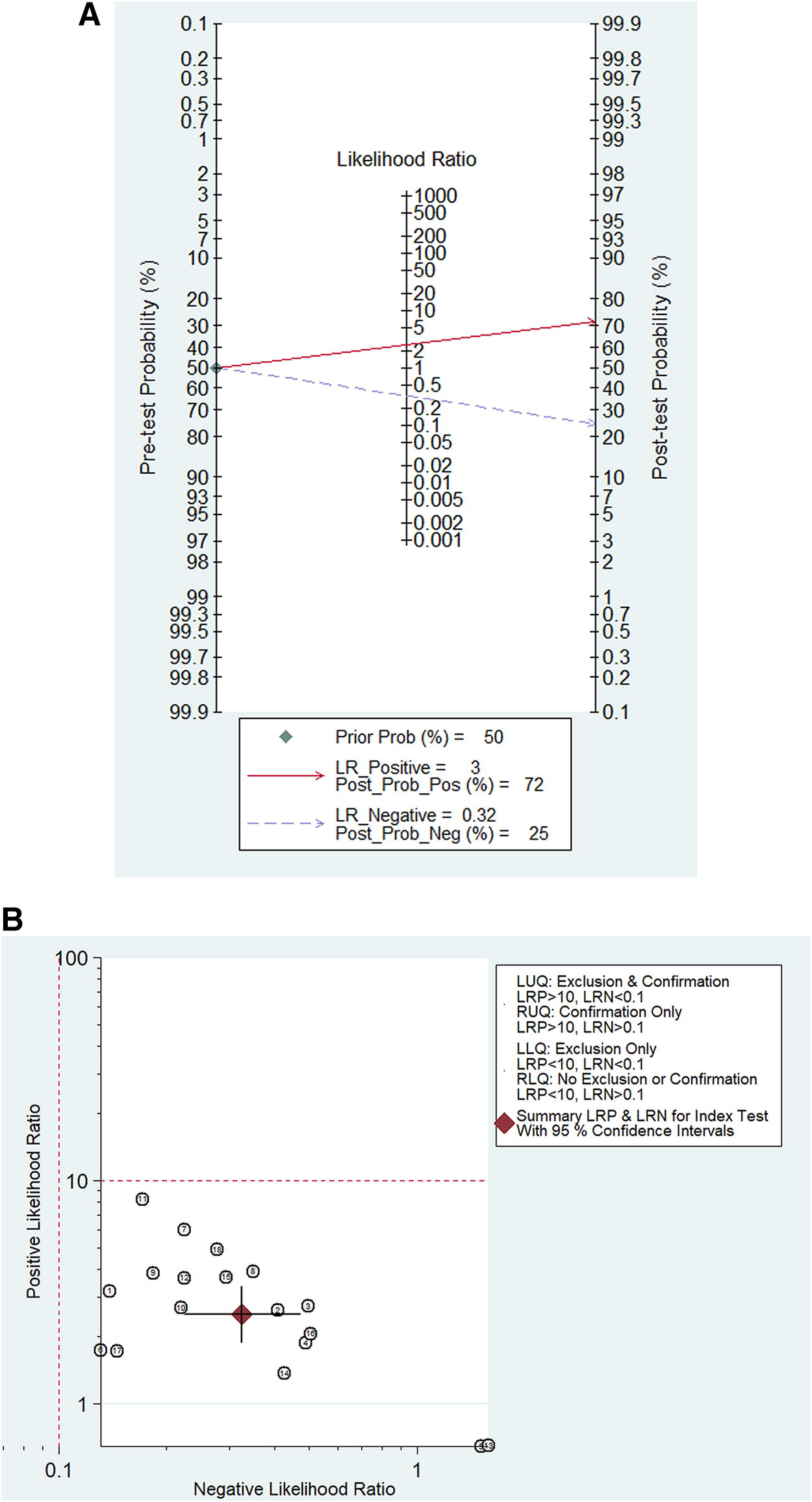
Assessment of the clinical applicability of neutrophil to lymphocyte ratio for diagnosis of orthopedic post-operative infection.
Sensitivity analysis and publication bias
The results of sensitivity analysis (Fig. 6) showed that the goodness-of-fit and bivariate normality indicated that the random-effects bivariate model was appropriate for the analysis (Fig. 6A, B). The impact analysis found that four studies had a large weight (Fig. 6C).18,19,25,29 Outlier detection implied that one of the studies could be the cause of heterogeneity (Fig. 6D). 18 After removing the abnormal data study, the AUC was 0.82 [0.79–0.85]. The results did not change significantly, suggesting that the stability of this study was good. Deek’s funnel plot (Fig. 7) was basically symmetrical, P = 0.48 > 0.05, and no significant publication bias was found in this study.
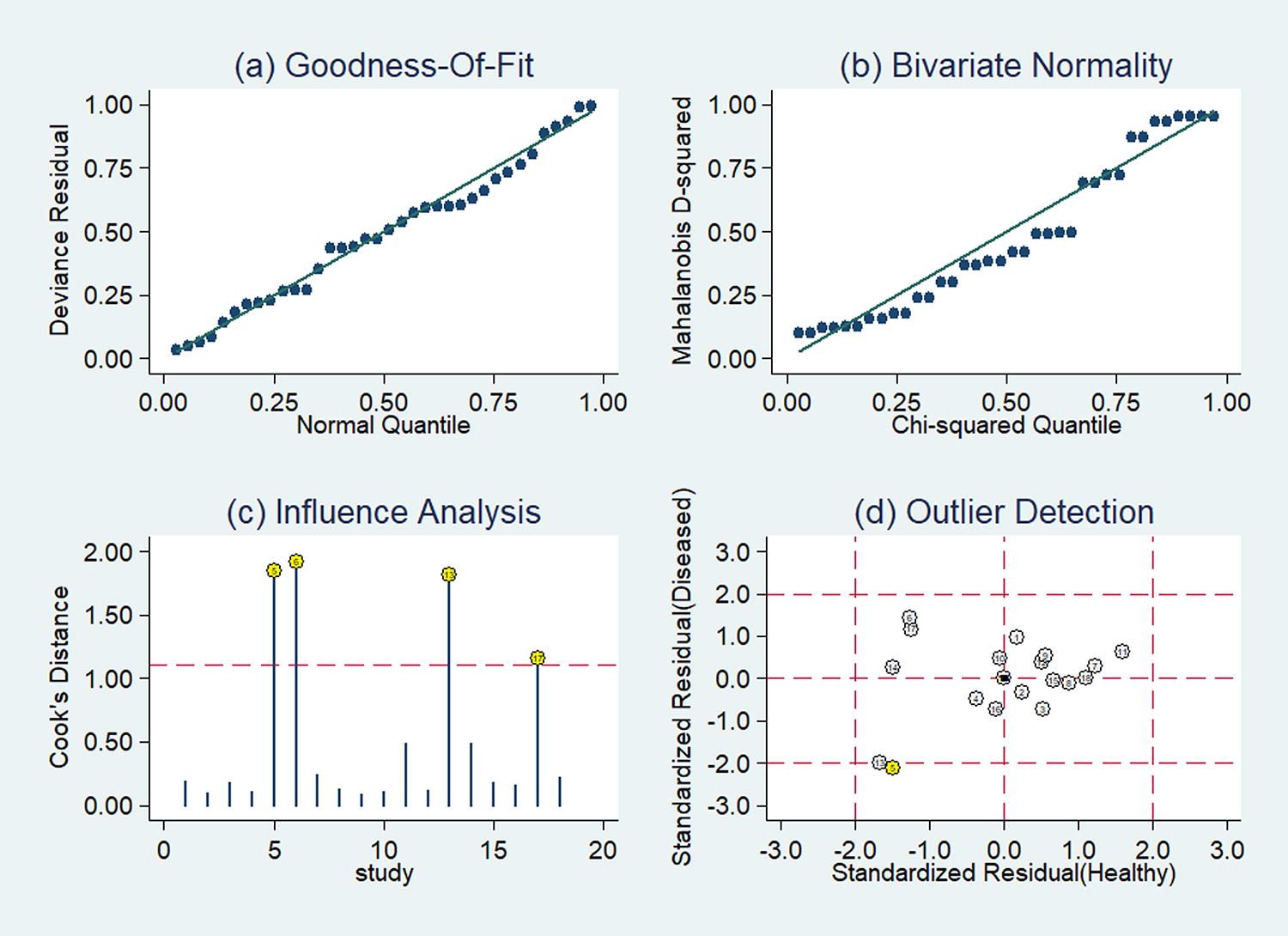
Sensitivity analysis of neutrophil to lymphocyte ratio in the diagnosis of orthopedic post-operative infection:
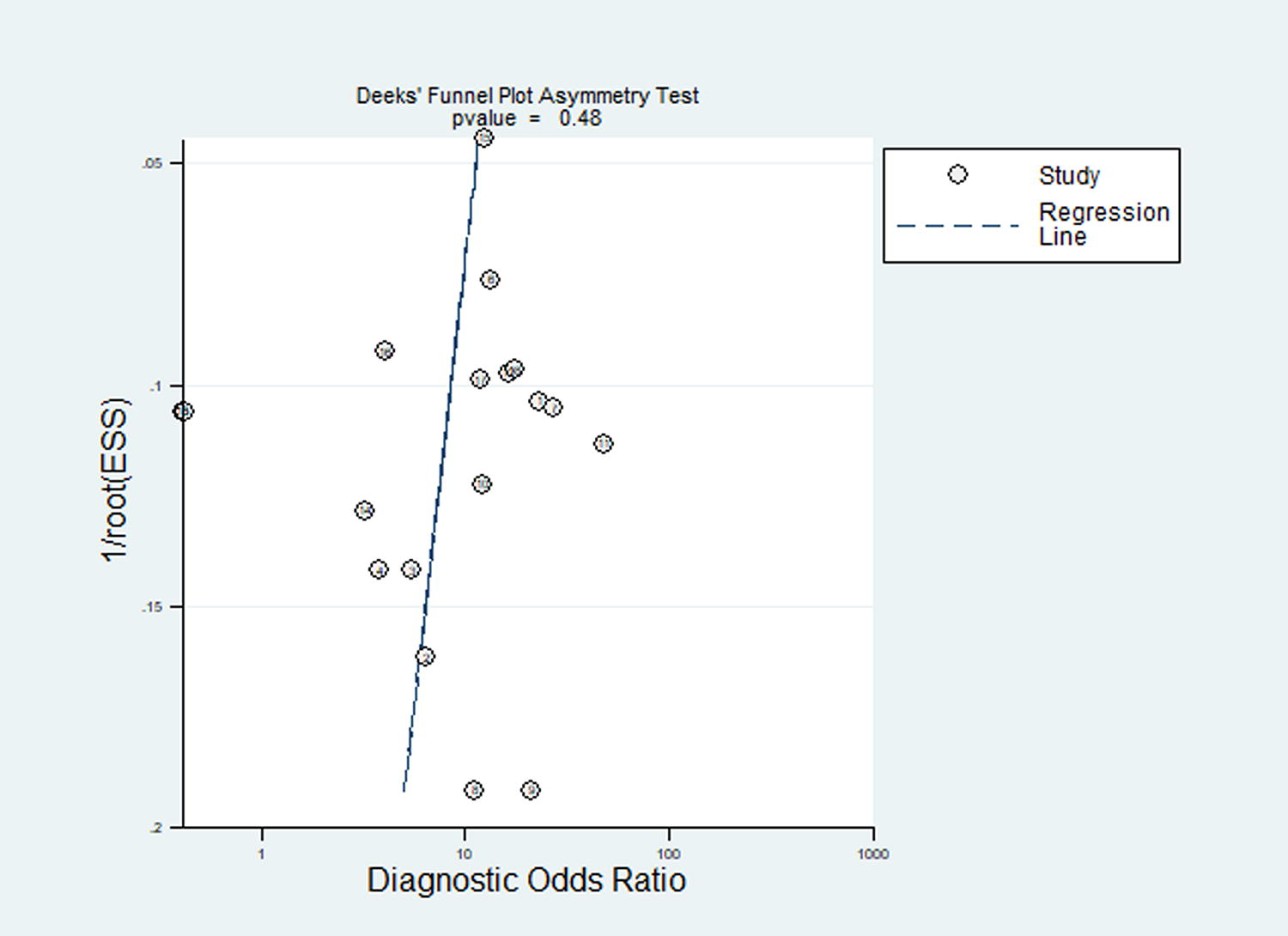
Deek’s funnel plot asymmetry test to explore publication bias. ESS, effective sample size.
Discussion
The results of meta-analysis showed that NLR had moderate diagnostic value for predicting infection after orthopedic surgery, with a pooled sensitivity of 0.77, a specificity of 0.69, and an AUC of 0.80. The DOR was 7.76, indicating that the probability of elevated NLR was approximately 7 times higher in patients with post-operative infection than in those without infection. Fagan’s nomogram analysis suggests that the use of NLR modestly increases the post-test probability of infection, from a pre-test probability of 50% for a positive test to a post-test probability of 72%, or reduces the post-test probability of a negative test to 25%. The likelihood ratio dot plots show that NLR has a limited ability to rule out infection, consistent with its modest sensitivity and specificity. Although these results do not prove that NLR is a perfect predictive tool, they do show that NLR is able to reflect the likelihood of infection to some extent. What this means for clinical practice is that while NLR cannot completely replace other more direct infection detection methods, such as bacterial culture and pathological examination, it can be used as a complementary tool to provide additional information to help physicians determine whether a patient is at risk for infection.
Notably, we found significant inter-study heterogeneity in sensitivity and specificity among the included studies. Meta-regression and subgroup analysis revealed possible sources of heterogeneity as infection site, type of surgery, time of blood test, and NLR cutoff value. NLR is less accurate in diagnosing surgical site infections (SSIs) than prosthesis or other deep infections. This may be because SSI tends to be more superficial and milder, resulting in less inflammation throughout the body and less variation in NLR. Regarding the type of surgery, NLR is less accurate in diagnosing post-fracture infections. Fracture surgery is often trauma surgery, and the trauma itself can cause post-operative stress responses and elevated NLR, which may mask changes in NLR caused by infection.
The timing of blood sampling also affects the accuracy of diagnosis. Compared with post-operative sampling, NLR measured before surgery had slightly less sensitivity but greater specificity for predicting post-operative infection. This may be attributed to a mixed baseline inflammatory profile in the pre-operative population. Most studies analyzed NLR within 1 week of surgery, but several extended beyond 2 weeks. The time range of this delay may contribute to heterogeneity, as NLR normalizes over time after surgery. In the early post-operative period, surgical trauma induced neutrophilia and lymphocytopenia and increased NLR, independent of infection. Over time, these trauma-induced NLR changes subsided, while persistently elevated NLR was more indicative of a possible infection. The best NLR cutoff values included in the study ranged from 0.83 to 5.17. Analysis of subgroups showed that higher cutoff values (≥3) reduced sensitivity without improving specificity. As NLR is affected by population characteristics, detection methods, and dynamics after surgical stimulation, the standardization of cutoff values is challenging. Defining appropriate cutoff values requires assessing the dynamics of NLR over multiple post-operative time periods.
This study has several strengths. First, to the best of our knowledge, this is the first systematic review and meta-analysis to comprehensively evaluate the accuracy of NLR in the diagnosis of infection after various types of orthopedic surgery. Second, we conducted a comprehensive literature search across multiple databases, with no restrictions on language or publication date, ensuring that all relevant studies were included. Third, we used a standardized QUADAS-2 tool to assess the methodological quality of the included studies, and only studies with high quality and low risk of bias were combined. Fourth, we used a bivariate mixed-effects model for meta-analysis, which provided reliable estimation results taking into account the heterogeneity among studies. Fifth, we performed a stratified analysis to explore potential sources of heterogeneity according to surgical factors and study characteristics, which led to a deeper understanding of the performance of the NLR assay. Sixth, in addition to sensitivity, specificity, and AUC, we also evaluated the clinical utility of NLR by Fagan’s plot analysis and likelihood ratio. Finally, we found no significant evidence of publication bias, which ensures the reliability of our included studies.
However, there are some limitations in this study: first, the included studies showed significant heterogeneity, which may be related to differences in the type of orthopedic surgery, the type of infection, the cutoff value of NLR, and the timing of NLR measurement. Although we performed meta-regression and subgroup analyses, our detailed exploration of these factors was limited by the relatively small number of studies in each subgroup. Second, most of the included studies were retrospective, and there were relatively few prospective cohort studies. Third, some of the included studies had small sample sizes, which are susceptible to selection bias and random error. Fourth, some studies may have had validation bias because cultures were not obtained in all patients to establish a diagnosis of infection. Fifth, the geographical distribution of the included studies was unbalanced, mainly from Asia, and only a few from Europe and America. Therefore, the applicability of the results still needs to be further verified in different populations. Finally, although we did our best to rule out publication bias, we cannot completely rule out the possibility of difficulties in publishing studies with negative results.
This meta-analysis has revealed several revelatory results. First, we need to interpret the results of NLR in a clinical context, considering factors such as the type of surgery, the purpose of the test, and the appropriate cutoff. An elevated NLR may not be particularly indicative in the context of early trauma or minor SSI, whereas a high NLR in the weeks following surgery is more likely to be associated with infection. Second, to improve the accuracy of diagnosis, it is better to use NLR together with other biomarkers, such as CRP, PCT, and ESR, as a comprehensive indicator. The limitations of a single test can be compensated for by synthesizing multiple imperfect tests. Third, more research should be conducted on the dynamic changes in NLR, because sustained changes may be more important than transient changes. Finally, we need more research data on the value of NLR on prognostic indicators such as treatment response and mortality after diagnosis of infection.
Conclusion
This study summarizes the diagnostic value of NLR in predicting infection after orthopedic surgery. NLR has moderate sensitivity and specificity. At the same time, the index is affected by the type of infection, type of surgery, detection time, and other factors. Although NLR can increase or decrease the degree of clinical suspicion of infection, it cannot be used as a single criterion to definitively diagnose infection. Therefore, prospective studies combined with other indicators should be conducted in the future to further clarify the clinical application value of NLR in infection after orthopedic surgery.
Footnotes
Acknowledgment
The authors would like to express their appreciation to all the members who participated in the study.
Ethics Approval
Institutional Review Board approval was not required because we only performed data analysis on the basis of published studies.
Informed Consent
Written informed consent was not required for this study because it is a meta-analysis on the basis of studies that have already been published.
Funding Information
This work was supported by grants from Medical and Health Research Project in Baoan District, Shenzhen (BA202200754203X027202211170045)
Author Disclosure Statement
The authors declare that there are no conflicts of interest that could be perceived as prejudicing the impartiality of this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.