
Abstract

To the Editor:
A
A 28-year-old female sought treatment due to redness, swelling, and pus discharge from her right thigh. Prior to admission, she had undergone an incision and drainage procedure for an abscess at a local hospital, describing the drainage as white, curd-like material. But she did not undergo further examinations outside the hospital. She denied any history of trauma, other surgeries, or contact with tuberculosis. Physical examination revealed a limp, with significant redness and swelling on the outer aspect of the right thigh near the hip, accompanied by elevated skin temperature and marked tenderness. Laboratory tests indicated a serum amyloid A (SAA) level of 155.32 mg/L, and interferon-γ release assay (IGRA) was positive. Doppler ultrasound of the lower extremities and chest computed tomography (CT; Fig. 1) showed no apparent abnormalities. A right femur anteroposterior radiograph (Fig. 2) revealed rough cortical margins and localized reduction in bone density at the greater trochanter. Thigh magnetic resonance imaging (MRI; Fig. 3) demonstrated bone marrow edema at the right femoral greater trochanter with adjacent muscle swelling, raising suspicion of a possible sinus tract. Bone scintigraphy (ECT; Fig. 4) indicated the possibility of osteomyelitis.
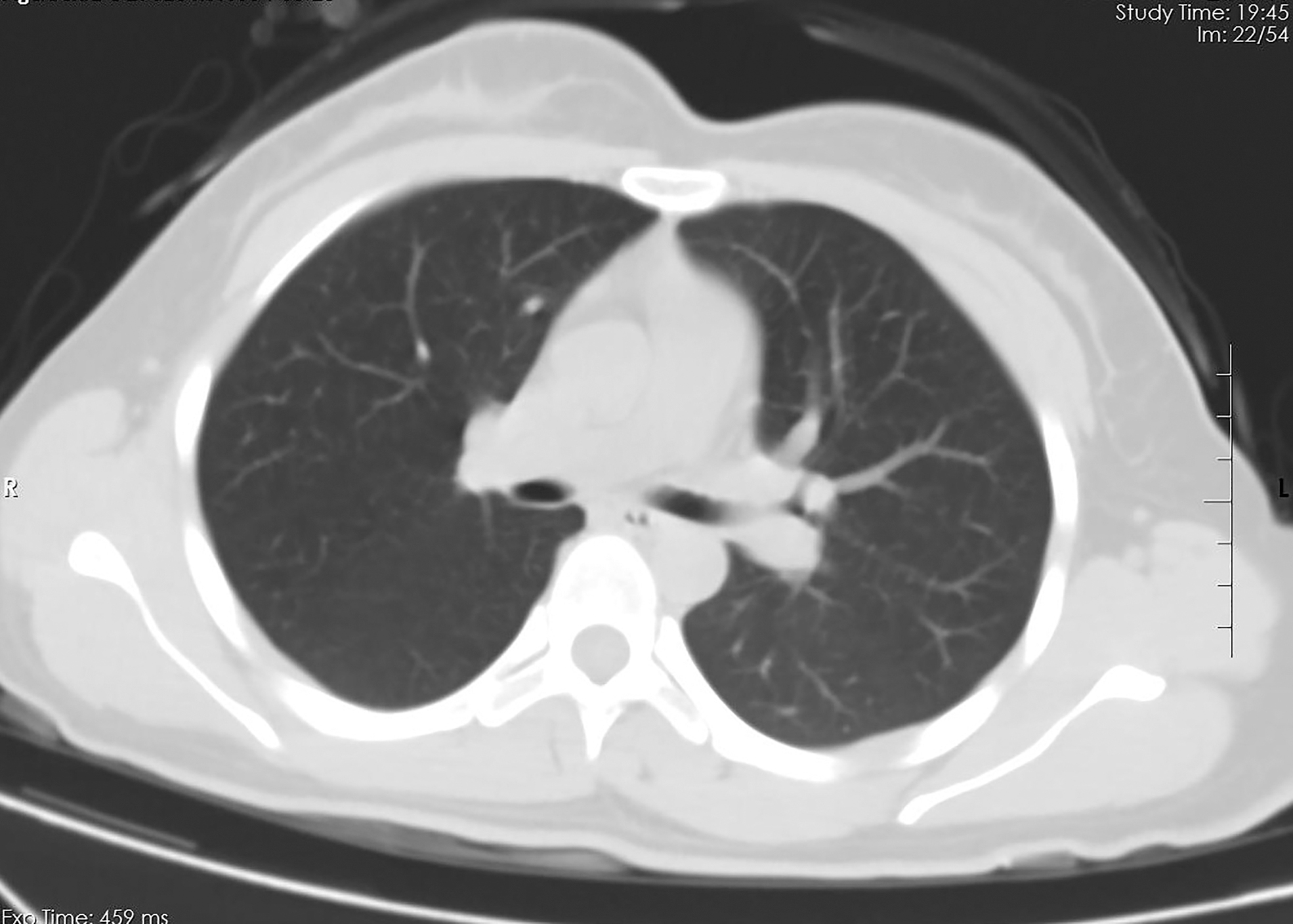
Chest computed tomography (CT) showed no apparent abnormalities.
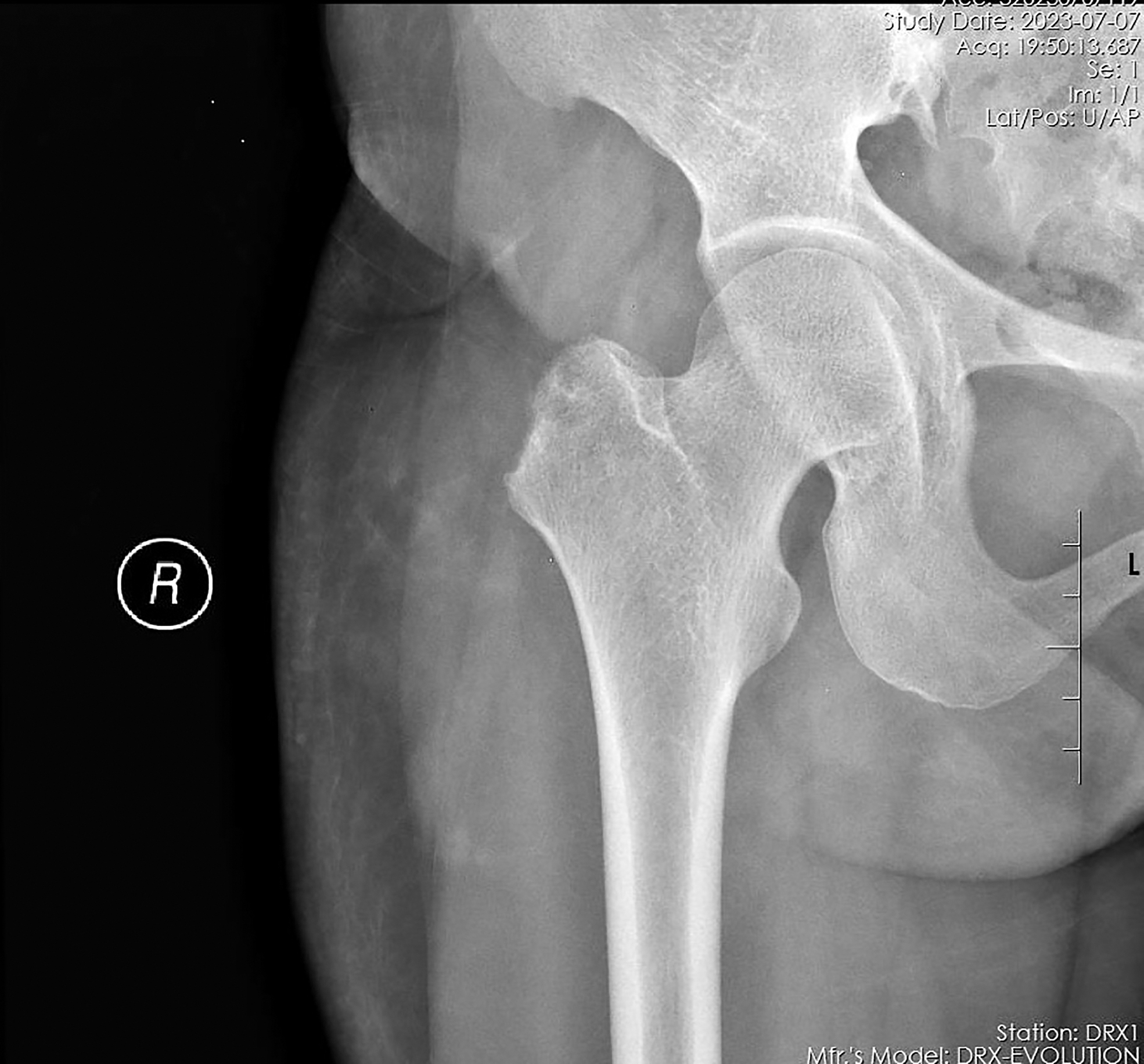
Right femur anteroposterior radiogram revealed rough cortical margins and localized reduction in bone density at the greater trochanter.

Thigh magnetic resonance imaging (MRI) demonstrated bone marrow edema at the right femoral greater trochanter with adjacent muscle swelling, raising suspicion of a possible sinus tract.

Bone scintigraphy (ECT) indicated the possibility of osteomyelitis.
On the basis of the patient's relevant data, it was considered to be osteomyelitis of the right femur, but tuberculosis infection cannot be ruled out. After consultation, the patient and her family requested surgical treatment. Subsequently, the patient underwent a right femoral lesion excision surgery. Soft tissue pathology of the lesion at the distal end of the right femur showed granulomatous inflammation, morphologically consistent with tuberculous changes (Fig. 5), negative acid-fast staining, and positive detection of Mycobacterium tuberculosis by polymerase chain reaction (PCR). Bone tissue from the lesion at the distal end of the right femur revealed a small amount of fragmented and necrotic bone, with a minimal amount of chronic inflammatory cell infiltration in the bone marrow. The final diagnosis was tuberculosis osteomyelitis of the right femur. The patient received post-operative antituberculosis treatment and recovered well after surgery.

Soft tissue pathology of the lesion at the distal end of the right femur showed granulomatous inflammation, morphologically consistent with tuberculous changes.
Tuberculous osteomyelitis can cause extensive local bone destruction. Therefore, timely detection and treatment are necessary to prevent permanent damage and disability. Because of the low prevalence and potential for atypical presentations, diagnosing tuberculous osteomyelitis is challenging even for experienced clinicians. A needle aspiration or excisional biopsy is mandatory for histopathologic diagnosis of femur osteomyelitis because radiologic findings cannot differentiate the cause of osteomyelitis, and sometimes may even appear neoplastic. In conclusion, tuberculous osteomyelitis of the femur is a serious condition that can cause morbidity and mortality if left untreated. Early diagnosis and prompt treatment with antitubercular chemotherapy or antibiotic agents can be effective in many cases, but surgical intervention may be necessary in some cases, particularly when complications arise.