
Abstract
Background:
Post-partum infection is a major contributor to maternal mortality and is responsible for approximately 10% of maternal fatalities worldwide. The risk of infection is substantially higher in cesarean section procedures. Approximately 8% of women who undergo cesarean sections are susceptible to infection. Although the body of evidence supporting the regular pre-operative utilization of prophylactic antibiotic treatment is steadily expanding, its usefulness in cesarean sections has not yet been standardized, and post-partum infection is still a serious medical challenge. We aimed to retrospectively assess the prophylactic effectiveness of cefazolin in combination with other antibiotic agents in cesarean sections.
Materials and Methods:
Both uni-variable and multi-variable analyses were conducted to identify factors that may affect cefazolin pre-operative antibiotic prophylaxis in elective cesarean section operations. The uni-variable analysis included timing of administration, operation duration, body mass index (BMI), and wound type. A multi-variable logistic regression model was then created to determine which variables provide independent information in the context of other variables.
Results:
Time of administration did not affect prophylactic cefazolin efficacy. However, prophylactic cefazolin was 1.43 and 1.77 times more effective when the operation lasted for 45 minutes or more, compared with operations that were shorter than 45 minutes. Patients with a BMI ranging from 18 to 29 kg/m2 showed increased efficacy of prophylactic cefazolin compared with obese patients with a BMI exceeding 30 kg/m2. The effectiveness of prophylactic cefazolin decreased by 95% in patients with clean-contaminated surgical incisions compared with those with clean surgical incisions.
Conclusions:
Our findings demonstrate that administering pre-operative prophylactic antibiotic agents to women undergoing cesarean section resulted in a reduction in post-partum infections, thereby reducing maternal mortality. Furthermore, optimal timing of administration, re-dosing if necessary, length of prophylactic medication, and dosing adjustments for obese patients are crucial factors in preventing surgical site infections and promoting antimicrobial stewardship.
Introduction
Cesarean section is one of the most common surgical procedures accomplished in obstetric departments worldwide. 1 Cesarean section and vaginal delivery are both associated with a post-partum infection, which is defined as infections that occur after vaginal and cesarean section delivery or during breastfeeding. Endometritis, surgical site infection, urinary tract, and mastitis are the most common infections after delivery. Many risk factors contribute to developing post-partum infections—for example, the history of cesarean section, pre-mature rupture of the membrane, repeated cervical examination, pre-existing pelvic infection, obesity, diabetes mellitus, and nutritional condition. 2
Hygienic procedures and aseptic techniques are crucial in controlling the microbial contamination of surgical incisions. Gynecologic and obstetric surgeons have consistently aimed to prevent infection at surgical sites. Infections following surgical procedures are a major contributor to post-operative morbidity. These infections can lead to severe complications such as bacteremia, wound abscess, pelvic abscess, septic shock, septic pelvic thrombophlebitis, and fascial dehiscence, resulting in serious adverse outcomes. 3
Many procedures in obstetric and gynecologic operations, the typical cesarean section in labor, and total vaginal or abdominal hysterectomy are associated with a major problem, which is post-operative surgical site infection. 4 The use of antimicrobial prophylaxis for cesarean section and other gynecologic surgical procedures is effective in reducing post-operative morbidity, costs, and duration of hospitalization. Proper antimicrobial prophylaxis has dual benefits; it enhances faster cure and shortens antimicrobial use.5–7
Post-partum infections are caused by the vagina’s normal flora. Factors such as labor duration and membrane rupture also contribute to amniotic fluid colonization and post-partum infections. The uterus can be ruptured during cesarean section operations, leading to infections. 8 Early and late post-partum infections occur within 48 hours and three to six weeks, respectively. 9 Endogenous flora in the skin, mucosal membranes, and hollow organs is the main source of pathogens in cesarean sections. Incisions in these tissues are prone to contamination. 10 Air in the operating room, surgical instruments, prostheses, and contact with the surgical team can also cause infections. 11
Antimicrobial prophylaxis can be used efficiently to prevent infection; however, its use has to be limited to precise, well-accepted indications to avoid excess cost, toxicity, and antimicrobial resistance. Prophylaxis is indicated for cesarean section and abdominal and vaginal hysterectomy.12–14 For cesarean delivery, administration of antibiotic agents within 30 minutes of operation has been shown to reduce the colonization of bacteria, and prior studies have not demonstrated a superior result with broad-spectrum antibiotic agents compared with cefazolin. Therefore, cefazolin is the recommended agent.15–18 This study aimed to describe the antimicrobial prophylaxis regimens prescribed before the elective cesarean section, compare the used prophylactic regimen and the national prophylaxis guidelines, and describe whether they interfere with antimicrobial stewardship. It also investigated the effect of weight, chronic diseases, age, and type of wound on the dose of used antibiotic agents. It aimed to develop the most appropriate antibiotic prophylactic regimen, which can be tailored and used as a guideline for cesarean section operations according to global guidelines.
Patients and Methods
A total of 336 female patients (of different ages) who underwent scheduled elective cesarean section operation were recruited at the Obstetrics and Gynecology Department, Khoula Hospital, Muscat, Sultanate of Oman. The elective cesarean section, also known as an elective C-section, is a planned surgical procedure and is scheduled in advance and not performed because of an emergency or immediate medical necessity. A retrospective study was conducted for nine months using the Al Shifa System, the recommended program in the Ministry of Health, Sultanate of Oman, to gather all patient-related data. The system tracks practice patterns associated with the use of prophylactic antibiotic agent in patients admitted for operation, and it records all orders for antibiotic drugs, the exact time of drug administration, the duration of antibiotic use, and the time when the prophylactic agent was discontinued. Moreover, the system tracks all aspects of surgical procedures, wound classification, surgical complications, and blood loss during the operation.
Furthermore, case records were retrieved to explore the relationship between obesity and chronic illness (e.g., diabetes mellitus, hypertension, and kidney patients) and the effectiveness of antibiotic prophylaxis. The type, name, frequency, and duration of used antibiotic agents were also recorded.
The number of cases (%) was recorded for categorical variables, and Pearson’s chi-square (χ2) test was used to compare them. Both uni-variable and multi-variable logistic regression models were applied to identify independent variables that could influence the efficacy of prophylactic cefazolin (2 g) in elective cesarean section operation. p-Values <0.05 were considered significant. Statistical analysis was performed using R (version 4.3.2), a Language and Environment for Statistical Computing (R Foundation for Statistical Computing, Vienna, Austria).
Results
Cesarean section statistics
This study included 4,239 female pregnant women; 18% of them were cesarean section and 8% (336 cases) were elective cesarean section, whereas natural delivery was about 74%, which takes the primary type of delivery (Fig. 1A). The age of the pregnant women who underwent elective cesarean section was between 20 years and more than 40 years. The majority fall in the category from 31 to 35 years of age, which is about 38%, and the lowest part was from 20 to 25 years of age, counted for 9%, and the age between 26 and 30 years was 20%, the age from 36 to 39 years was 22%, and the age more than 40 years counted for 11% (Fig. 1B).

Percentage of cesarean section to normal delivery and age of pregnant women.
Antibiotic prophylaxis
As recommended by the national surgical antimicrobial prophylaxis guidelines in Oman, the administration of antibiotic agents for surgical prophylaxis should be as near the incision time as possible. Also, infusion of antibiotic agents for surgical prophylaxis should begin within 1 hour before skin incision. Antibiotic agents to be administrated include cefazolin (2 gm or 3 gm for patients weighing >120kg or with blood loss >1.5 L), cefuroxime (1.5 gm), clindamycin (900 mg), vancomycin (15 mg/kg), gentamicin (5 mg/kg), and metronidazole (500 mg). For the cesarean section, cefazolin (2 gm IV pre-operation) and gentamicin (1.5 mg/kg IV + clindamycin 600 mg IV pre-operation) were administered.
In this study, cefazolin was prescribed for all elective cesarean sections at a dose of 2 gm. About 10% (33 out of 336 cases) did not follow the provided national guidelines owing to wrong prescriptions or prescriptions of additional antibiotic agents that are not required (Fig. 2A). Furthermore, the timing of cefazolin administration was recorded (Fig. 2B), where 62% of cases were administered cefazolin after the operation.
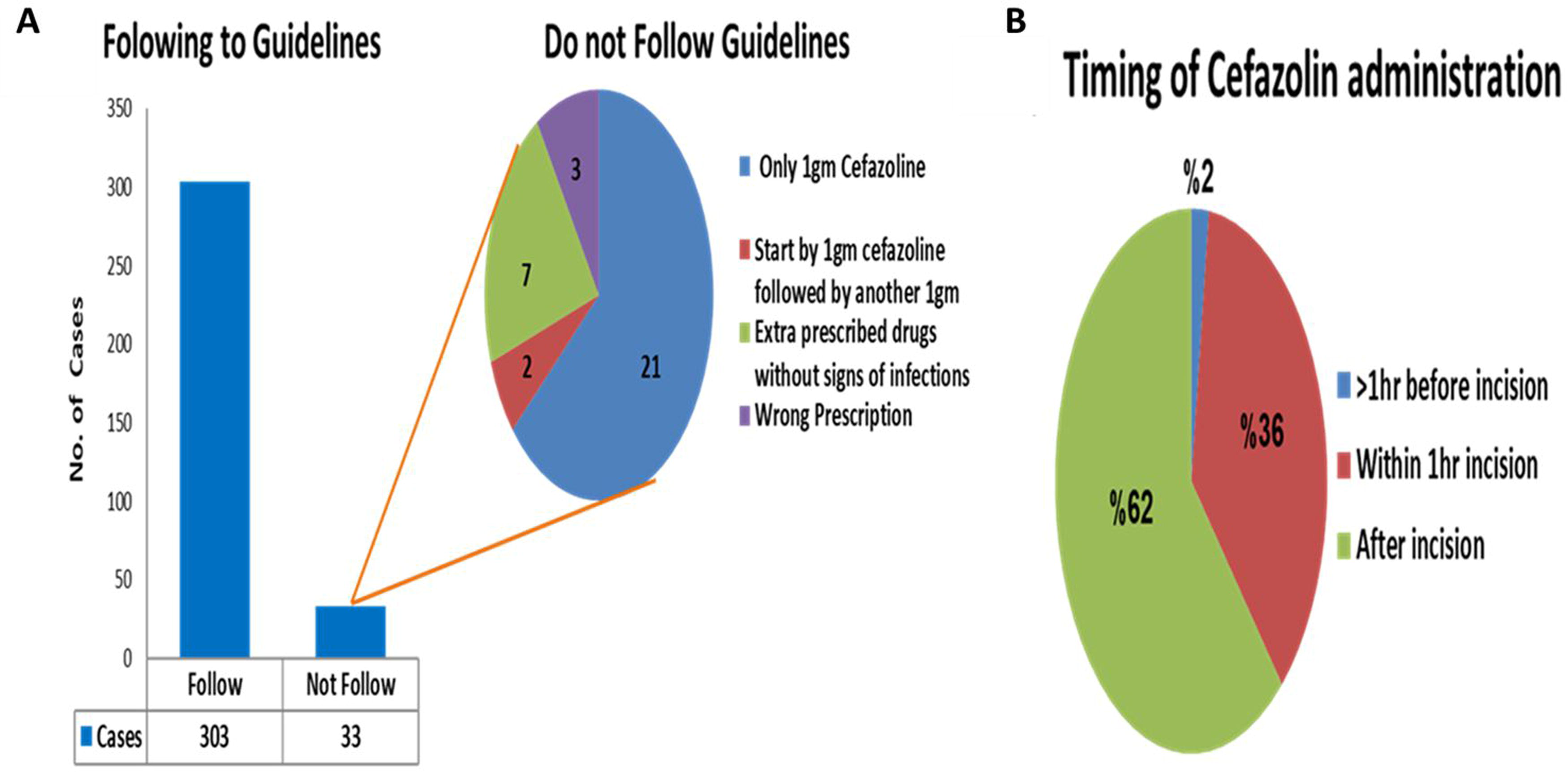
Adherence to national guidelines for administering cefazolin as prophylaxis in elective cesarean section.
Excess cefazolin dose
Most cases did not require an increase in cefazolin dose to more than 2 gm; however, 23% of cases that followed the national guidelines were required to exceed the dose of more than 2 gm. The dose increase was decided on the basis of the clinical situation of each case. It was observed that the cefazolin dose was not increased in the case of pregnant women who were diabetic, obese (body mass index [BMI] >30), or hypertensive. Several factors were evaluated to be correlated to the increase in cefazolin dose. There was no real correlation between age and increase in dose, as shown in Figure 3.
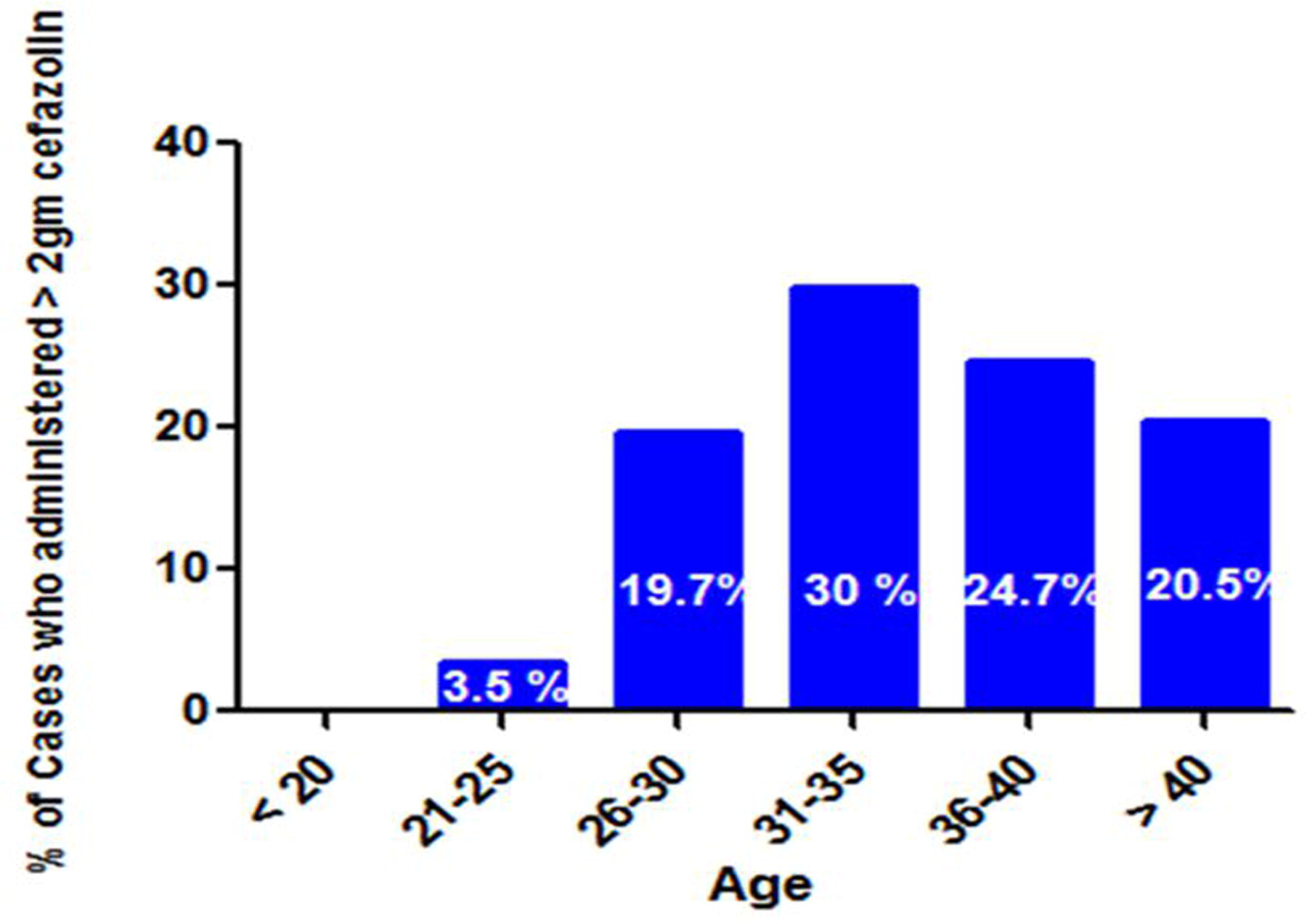
Cefazolin dose increases at different ages.
Furthermore, the relationship between the duration of the operation and the increase in cefazolin dose was documented. There was a clear increment of cefazolin dose in the prolonged duration of the procedure, as the cefazolin dose has been increased by more than 2 gm in the prolonged duration of the operation that exceeded 1 hour (20.5%) in comparison to short operation duration, <45 min (7%) (Fig. 4A). Another critical factor, the wound type, was observed to explain its effect on cefazolin dose increments. The percentage of cases requiring an increase in cefazolin dose in clean and clean-contaminated surgical incisions was similar (Fig. 4B).
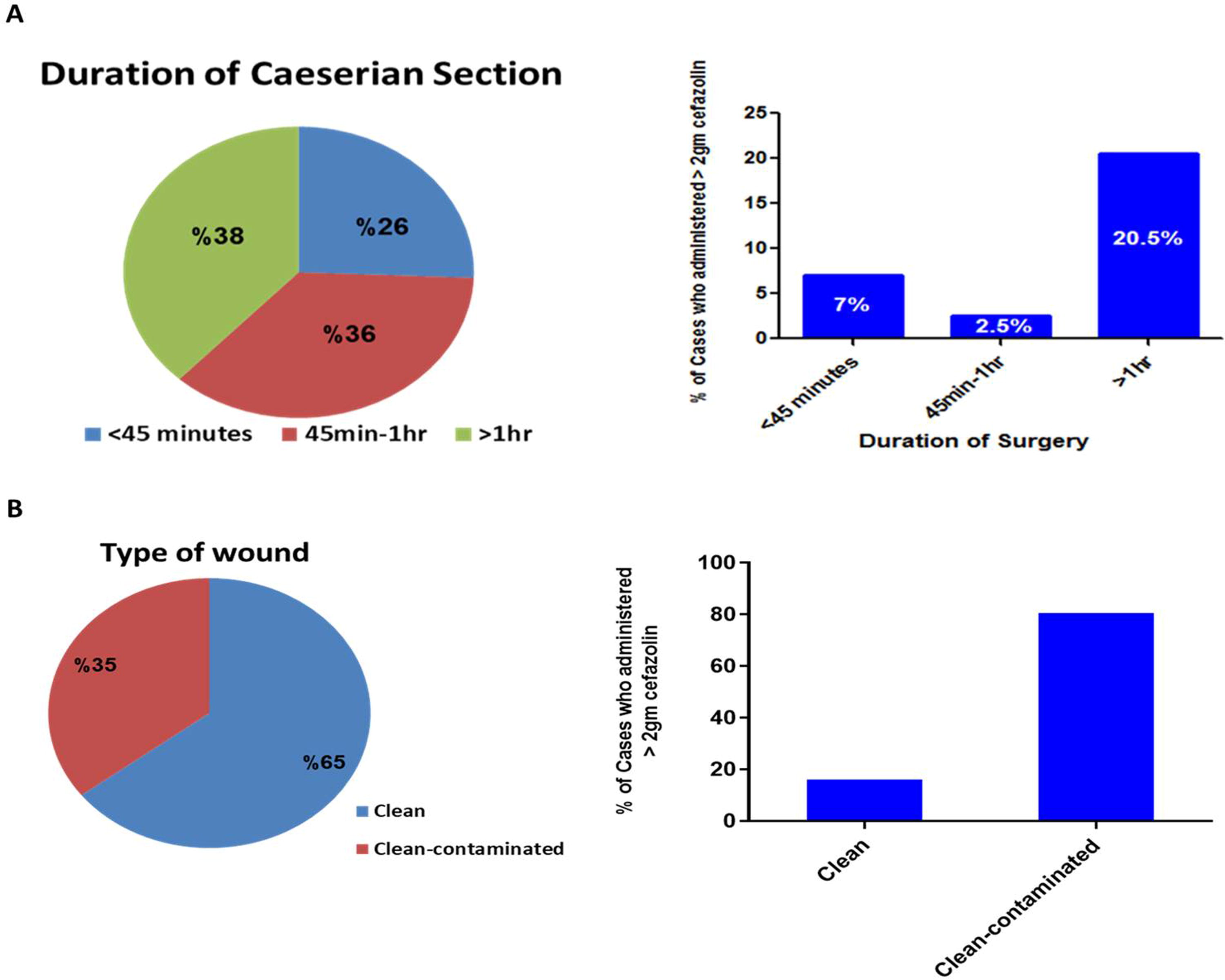
Effect of operation duration
Cefuroxime and metronidazole were prescribed, in addition to cefazolin, as pre-operative prophylaxis in the case of pregnant women who had higher BMI and/or suffered from urinary tract infections. The cefuroxime and metronidazole were prescribed in 9% of total cases, whereas the cefuroxime was prescribed alone in 4.2% of cases (Fig. 5).

Prescribed antibiotic agents other than cefazolin.
Factors influencing pre-operative antibiotic prophylaxis with cefazolin
Uni-variable and multi-variable analyses were performed to identify factors that might influence the effectiveness of pre-operative antibiotic prophylaxis with cefazolin in elective cesarean section operation. Established variables, including timing of administration, duration of operation, BMI, and wound type, were considered for inclusion and assessment in the uni-variable analysis; subsequently, a multi-variable logistic regression model was constructed to evaluate which of these variables provides independent information in the context of other established variables (Table 1).
Uni-variable and Multi-variable Analyses of the Various Factors Influencing Pre-operative Antibiotic Prophylaxis with Cefazolin in Elective Cesarean Section Operations
Indicates a statistically significant difference.
BMI, body mass index; OR, odds ratio; CI, confidence interval.
The timing of the administration was not associated with the effectiveness of prophylactic cefazolin (odds ratio [OR] = 1.01, 95% confidence interval [CI] = 0.53–1.95, p = 0.971). In contrast, the efficacy of prophylactic cefazolin was 1.43 and 1.77 times greater when the duration of operation was 45 minutes or longer compared with a shorter operation period of less than 45 minutes; however, the differences did not reach statistical significance (p = 0.369 and 0.151, respectively).
In addition, patients with a BMI between 25 and 29 kg/m2 exhibited superior effectiveness of prophylactic cefazolin compared with obese patients having a BMI greater than 30 kg/m2 (OR = 2.50, 95% CI = 1.33–4.75, p = 0.005). Patients with a BMI of 18–24 kg/m2 also showed higher effectiveness of prophylactic cefazolin when compared with those with a BMI greater than 30 kg/m2; nevertheless, the difference did not meet the criteria for statistical significance (OR = 2.12, 95% CI = 0.83–5.82, p = 0.128).
The odds of prophylactic cefazolin efficacy decreased by 95% in patients who had clean-contaminated surgical incisions compared with those having clean surgical incisions (OR = 0.05, 95% CI = 0.03–0.10, p < 0.001).
It is worth mentioning that the binned residual plot indicated poor model fit, which suggests that other important predictors were not included in the model, which could be attributed to the limited data and the retrospective nature of the study.
Discussion
Surgical site infection is an infection that occurs in patients who have undergone surgical procedures. These infections typically develop in the superficial or deep layers of the incision, as well as in the manipulated or traumatized organ or area, such as the peritoneal region. They are considered severe and costly, leading to increased morbidity, mortality, and extended hospital stays. Surgical site infections are often preceded by microbial contamination during the surgical process. Although bacteria contaminate most surgical incisions, only a small proportion progress to clinical infection because some patients’ innate host defense mechanisms efficiently eliminate the contaminants at the surgical site. Several important factors determine the likelihood of surgical site infection. These include the bacterial contamination dose, the bacteria’s virulence, and the patient’s resistance to infection. Because the number and virulence of bacteria increase, the chances of infection also increase, proportionally. 19 Specific local characteristics of the wound, such as drains, sutures, residual dead tissue, or other foreign materials, can amplify the impact of the bacterial inoculum. In addition, contamination is common during operations involving body structures that are typically colonized by bacteria, such as the bowel. Quantitatively, when the surgical site is contaminated with more than 105 microorganisms per gram of tissue, the risk of surgical site infection is substantially increased. However, foreign materials at the surgical site can lower the threshold for infection, requiring a smaller quantity of contaminating microorganisms to cause an infection. 20
Cesarean section worldwide has increased in the last few years. In the statistics that covered 169 countries, the percentage of cesarean section is 21.1. The highest cesarean section rate was in the Dominican Republic, about 58.1%. The lower cesarean section rate was 0.6% in South Sudan. This increase can be attributed to various factors, including those mentioned earlier. There is a noticeable increase in the prevalence of obesity among pregnant women, which reflects a global trend attributed to a sedentary lifestyle. Obesity contributes to the risk of challenging labor, and personal beliefs may also influence the preference for cesarean section over vaginal delivery. Unfortunately, women who undergo cesarean section face a substantially higher risk of infection, ranging from 5 to 20 times greater than those who have a vaginal delivery. Rates of surgical site infection and severe infectious complications can be as high as 25%. 21 The World Health Organization has suggested 15% as the ideal cesarean section rate for decades. Yet, rates around the world keep climbing because of many factors, such as breech presentation of babies, obesity, safety, and others. 22 These findings showed that 26% of total delivered babies in this period were delivered by the cesarean section, divided into 18% emergent cesarean cuts and 8% elective cuts.
In this study, the age of women who underwent elective cesarean section was relatively high: 30%, 24.7%, and 20.5% of all cases were 31–35 years, 36–40 years, and older than 40 years, respectively. In contrast, the percentage of cesarean sections in younger ages was as low as 3.5% in 21–25 years of age. That may be owed to delivery complications increasing with age, which could be why the percentage of cesarean sections in older ages is higher than that in younger females.23,24
Unfortunately, women who undergo cesarean section have a 5- to 20-fold risk of infection than women having vaginal delivery. Rates of surgical site infection and infectious severe complications can be as high as 25%. Cesarean section contamination and predicted infections can occur owing to various causes. The surgical site can become contaminated during the C-section procedure, leading to an increased risk of infection. Factors contributing to contamination include inadequate sterilization of instruments, improper handling of surgical equipment, or poor adherence to aseptic techniques. Furthermore, bacteria in the genital tract, such as Group B Streptococcus, can increase the risk of infection during a C-section. If proper preventive measures, such as administration of antibiotic agents, are not taken, these bacteria can enter the surgical site and cause infections. Prolonged rupture of membranes—when the amniotic sac ruptures and there is a delay in delivering the baby—can increase the risk of contamination and infection. Prolonged rupture of membranes provides a pathway for bacteria to enter the uterus and potentially cause infections. In emergencies, time for proper preparation and adherence to strict aseptic techniques may be limited, increasing the risk of contamination and subsequent infections. In addition, certain maternal factors can predispose individuals to an increased risk of C-section infections. These factors may include obesity, diabetes mellitus, immune system disorders, or other underlying medical conditions impairing wound healing and increasing susceptibility to infections. C-section infections include surgical site infections, endometritis, urinary tract infections, and, less commonly, infections in other organs such as the bladder or lungs. 25
Antimicrobial prophylaxis measures are essential in every operation, including the cesarean section. The aim is to prevent infections and severe sequelae at the operation site. Antibiotic prophylaxis aims not to sterilize tissues but to decrease the colonization pressure of microorganisms introduced at the time of operation to a level that the patient’s immune system can overcome. The chosen antibiotic must be safe, inexpensive, and effective against organisms likely to be encountered in the surgical procedure. This retrospective study sheds light on the efficacy of cefazolin as antibiotic prophylaxis in cesarean sections. Cephalosporins are used to treat a wide range of infections, but some are also effective for treating more severe infections, such as septicemia and meningitis. Cephalosporins act by inhibiting the formation of bacterial cell walls, and their activity varies according to their generation.26–28 Cefazolin is a first-generation cephalosporin antibiotic; it was the most common antibiotic prescribed as prophylaxis pre-operatively as a 2 gm intravenous injection. It is active against gram-positive bacteria such as coagulase-negative Staphylococci, methicillin-susceptible Staphylococcus aureus (MSSA), Streptococci spp., particularly penicillin-susceptible Streptococcus pneumoniae, and gram-negative bacteria such as Escherichia coli, Proteus mirabilis, Moraxella catarrhalis, and Klebsiella pneumoniae. Cefazolin must be administered in a way that ensures serum and tissue levels are adequate before an incision is made.29,30 It was mainly given within 1 hour of incision in 36% of cases. The typical average duration of operation is 44.3 minutes. In this study, 38% of women stayed in the operation for more than 1 hour, which was explained in some cases by the physician, who remarked that the patient was obese, which made it difficult for the surgeon to cut the many skin layers. This prolonged duration will have an impact on the dose of cefazolin administered. There was a clear increment of cefazolin dose during the prolonged duration of the procedure. When the patients are exposed to the environment, they are exposed to microorganisms. Therefore, they needed a larger dose of antibiotic agents, and additive doses were mostly given after the operation when the procedure was prolonged. It was noticed that 20.5% of all cases administered more than 2 gm of cefazolin were for this reason, which is because the half-life of cefazolin is 1.8 hours, so extra doses are recommended if the operation is prolonged to ensure the coverage of the antimicrobial effect along the duration of operation when blood loss is average.31,32
The primary objective of an Antimicrobial Stewardship Program is to enhance patient care safety and quality although playing a substantial role in reducing the emergence and spread of antimicrobial resistance. 33 It also serves as a crucial component in minimizing health-care–associated infections. To ensure appropriate antibiotic usage, a recommended approach called “Start Smart-Then Focus” is advised for all antibiotic prescriptions. It is essential to understand that antibiotic agents not only treat infections but also have an impact on the microbial environment within and beyond the patient. Therefore, their usage should be accurate and cautious. Antimicrobial therapy should only be initiated when clear evidence of infection is present. 34 According to the national guideline, although the alternatives of cefazolin are gentamicin 1.5 mg/kg plus clindamycin 600 mg intravenous injection pre-operative, the physician does not use it in practice. They usually do not use gentamicin because it has a short half-life and can cause ototoxicity and nephrotoxicity. Alternatively, cefuroxime and metronidazole were prescribed. Prior studies showed that both antibiotic agents were prescribed in the case of pregnant women who have higher BMI and the presence of urinary tract infections. Almost 65% of surgical incisions in the elective cesarean section were considered to be clean surgical incisions, which are uninfected surgical incisions in which different body tracts are not entered. The rest were clean-contaminated, where the genital tract was entered under controlled conditions and without unusual contamination. Notably, there was no difference in the administered antibiotic agents or their doses in clean or clean-contaminated sections. Moreover, it was observed that comorbidities like hypertension, diabetes mellitus, anemia, or other diseases did not have any effect either on the dose of cefazolin or the addition of other drugs, as all the cases with comorbidity did not receive excess cefazolin or additional antibiotic agents. Furthermore, the multi-variable analysis showed the influence of the wound type and BMI on increasing the dose of cefazolin and the need to add additional antibiotic agents, such as cefuroxime and/or metronidazole. At the same time, the timing of administration and duration of operation do not influence cefazolin dose increment.
The main limitation of this study was that the efficacy of cefazolin as antibiotic prophylaxis in cesarean sections was not studied. Another limitation that deserves further elucidation is that the analysis of the logistic regression model demonstrates a poor model fit, indicating that other important variables were not included in the model, which could be ascribed to the restricted data and the retrospective character of the study. Therefore, the inclusion of other potential factors in future studies, such as the precise timing of antibiotic administration before operation and the presence of comorbidities, could be useful in improving the statistical model. Moreover, further prospective studies are needed to describe the efficacy of cefazolin use and compare its use with other antibiotic agents.
Conclusions
Cefazolin was frequently prescribed for prophylaxis because of its broad-spectrum effectiveness against a wide range of microorganisms suspected to be in the operation site, besides its relatively good safety profile in pregnancy. Additional antibiotic agents were added for conditions like obesity, prolonged operation duration, and excessive blood loss. Other factors like comorbidities did not affect the cefazolin regimen. Collectively, these findings indicate the effectiveness of cefazolin as a prophylactic agent in cesarean sections. In addition, it is important to consider increasing its dose and/or adding cefuroxime and metronidazole in cases of clean-contaminated surgical incisions and high BMI.
Footnotes
Authors’ Contributions
Conceptualization: M.A.M.A. and W.A.H.H. Methodology: R.A.M. and F.A.R. Software: F.B. and A.A.C. Validation: F.B. and A.A.C. Formal analysis: A.S.A.H. Investigation: R.A.M. and F.A.R. Resources: M.A.M.A. Data curation: R.A.M. and F.A.R. Writing—original draft preparation: A.S.A.H., M.A.M.A. and W.A.H.H. Writing—reviewing and editing: M.A.M.A., and W.A.H.H. Visualization: A.S.A.H. Supervision: M.A.M.A. and W.A.H.H. Project administration: W.A.H.H. Funding acquisition: M.A.M.A.
Institutional Review Board Statement
The study’s data were retrieved from the Omani Ministry of Health database through the Al Shifa platform. All the used data were analyzed after removing all identifiers. This study was approved by the Research and Ethical Committee of Oman College of Health Sciences, Sultanate of Oman (OCHS/REC/PROPOSAL-APPROVED/33/2022).
Data Availability Statement
All data generated or analyzed during this study are included in this article.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This work was supported and funded by the Deanship of Scientific Research at Imam Mohammad Ibn Saud Islamic University (IMSIU) (grant number IMSIU-RPP2023065).