
Abstract
Introduction:
Although postoperative antibiotic prophylaxis has not been shown to prevent surgical site infections, prolonged antibiotic administration is common in low- and middle-income countries. We developed a quality improvement program to reduce unnecessary postoperative antibiotics through hospital-specific guideline development and the use of a brief, multidisciplinary discussion of antibiotic indication, choice, and duration during clinical rounds. We assessed reduction in the number of patients receiving ≥24 h of antibiotic prophylaxis after clean and clean-contaminated surgery.
Methods:
We piloted the program at a referral hospital in Ethiopia from February to September 2023. After a 6-week baseline assessment, multidisciplinary teams adapted international guidelines for surgical prophylaxis to local disease burden, medication availability, and cost restrictions; stakeholders from surgical departments provided feedback. Surgical teams implemented a “timeout” during rounds to apply these guidelines to patient care; compliance with the timeout and antibiotic administration was assessed throughout the study period.
Results:
We collected data from 636 patients; 159 (25%) in the baseline period and 477 (75%) in the intervention period. The percentage of patients receiving ≥24 h of antibiotic prophylaxis after surgery decreased from 50.9% in the baseline period to 40.9% in the intervention period (p = 0.027) and was associated with a 0.5 day reduction in postoperative length of stay (p = 0.047).
Discussion:
This antibiotic stewardship pilot program reduced postoperative antibiotic prophylaxis in a resource-constrained setting in Sub-Saharan Africa and was associated with shorter length of stay. This program has the potential to reduce unnecessary antibiotic use in this population.
Introduction
The World Health Organization (WHO) has named antimicrobial resistance (AMR) one of the world’s top 10 public health threats, driven by the misuse and overuse of antimicrobials. 1 It is estimated that AMR will lead to 10 million deaths worldwide by 2050 if AMR increases at its current rate. 2 Today, the highest burden of antimicrobial resistance is in Sub-Saharan Africa.3,4 Surgical prophylaxis is one major area of antibiotic overuse; 1 in 6 prescriptions for antibiotics worldwide are for surgical prophylaxis. 5 While for some surgical pathologies, antibiotics are administered postoperatively to treat a known infection or gross contaminations, the WHO recommends against continuing antibiotic prophylaxis in the postoperative period when neither infection nor gross contamination is present, such as in clean- and clean-contaminated operations. 6 However, postoperative antibiotic prophylaxis is common, particularly in resource-limited settings where maintaining operating room sterility is challenging and surgical site infection (SSI) rates are high.7,8 During a quality improvement initiative to improve perioperative antisepsis practices in 19 low- and middle-income country hospitals, we noted that one in four patients who underwent wound class I or II operations received postoperative prophylaxis for over 24 h without any additional reduction in SSI. 9
Antibiotic stewardship practices such as continuous monitoring of antibiotic use or resistance are not always available in low resource settings due to staff shortages and infrastructure limitations. 10 To improve antibiotic stewardship, Lifebox, 11 a nonprofit committed to improving the safety of surgery globally, created a quality improvement program to develop and implement hospital-specific antibiotic stewardship guidelines in surgical patients centered on the use of an “antibiotic timeout,” a verbal checkpoint during ward rounds to motivate behavior change and reduce unindicated antibiotic use.
An antibiotic timeout was chosen to mirror existing checklist tools such as the WHO Surgical Safety Checklist, which have been used to reinforce specific aspects of medical care.12,13 The timeout process is familiar to surgical teams in Ethiopia, where the Ministry of Health introduced the Surgical Safety Checklist in operating rooms in 2016. 14 In this quality improvement program, a ward round timeout was used to standardize antibiotic stewardship practices by improving communication among surgical teams. It was identified as a teachable moment when suboptimal antibiotic prescribing habits could be corrected. However, such tools are not adequate when underlying systems remain unchanged.15,16 For this reason, developing and implementing locally contextualized guidelines was incorporated as a core part of the intervention. Standard treatment guidelines for appropriate antimicrobial use are often not available; when available, they often do not account for contextual differences, such as medication availability and infrastructure challenges, resulting in poor guideline adherence. 17 In Ethiopia, standard treatment guidelines are available but adherence to recommendations remains low.18–20 Because poor infection prevention practices combined with the low perceived risk of using broad spectrum antibiotics may contribute to antibiotic overprescribing, 21 educational workshops were developed that reinforced knowledge of resistance and also trained surgeons to address sterility concerns in the operating room.
We hypothesized that this quality improvement initiative could encourage awareness of and adherence to hospital-specific postoperative antibiotic stewardship guidelines and reduce the number of patients receiving ≥24 h of antibiotic prophylaxis after clean and clean-contaminated surgery.
Methods
Intervention design
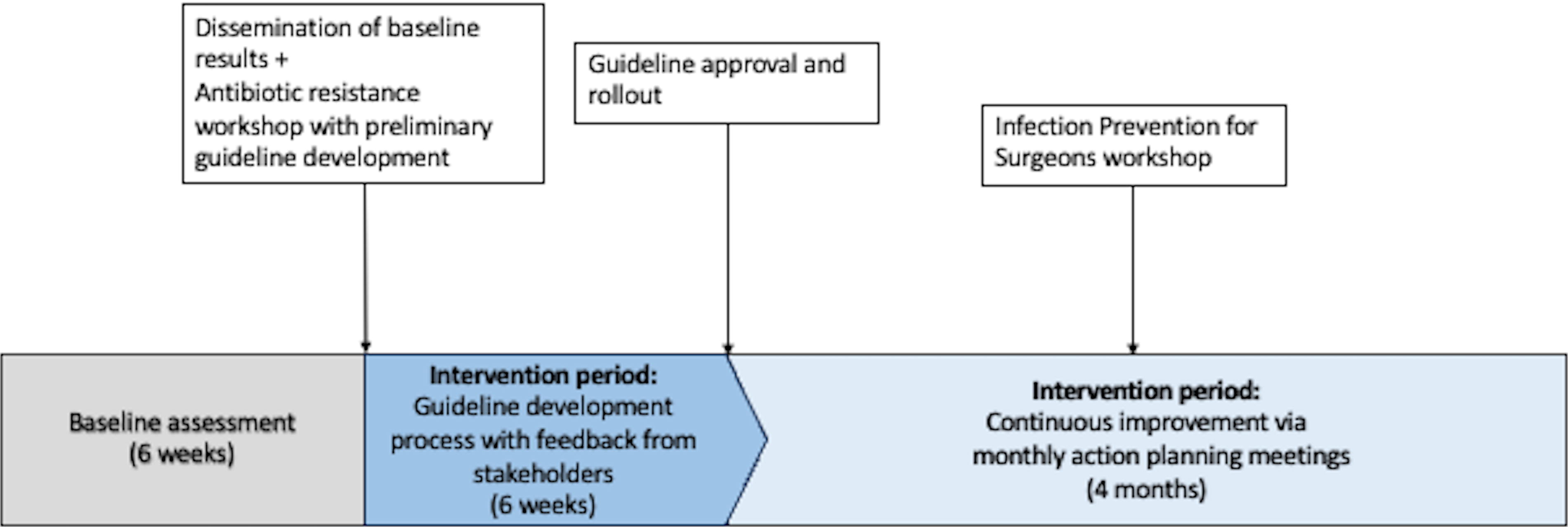
The program began with a 6-week baseline assessment of antibiotic prescribing practices and interdisciplinary communication on ward rounds based on direct observation using a structured recording form. The baseline period concluded with the dissemination of baseline data to hospital leadership and a two-day workshop to develop hospital-specific antibiotic stewardship guidelines (Fig. 1). The first day of the workshop focused on antibiotic resistance and the use of a timeout, defined as a brief, multidisciplinary discussion of antibiotic indication, choice, and duration on ward rounds, to improve team communication. On the second day, participants reviewed evidence-based antibiotic stewardship practices for the most common procedures performed at the hospital, with a focus on antibiotic prophylaxis. Participants were then divided into multidisciplinary teams to complete an exercise of adapting national and international guidelines and evidence on antibiotic cessation in surgical patients to local disease burden, medication availability, and cost restrictions. Workshop participants were encouraged to address the cessation of antibiotic prophylaxis postoperatively in clean and clean-contaminated operations where the lack of utility of postoperative prophylaxis is well-established and infection risk is lowest. 22 However, workshop participants were allowed to also address more complex cases and incorporate clinical criteria they felt were important in decision-making.
Program structure and design.
In the first six weeks of the intervention period, these adapted guidelines were shared among hospital stakeholders for several iterations of feedback and improvement. Ultimately, the guidelines were approved by hospital leadership and disseminated to the department. Clinicians were then asked to implement them on the surgical ward and incorporate a “time out” on rounds to help with adoption.
Facility feedback and process improvements
Guideline development and approval were followed by a series of monthly action planning meetings that were the foundation of the program’s plan-do-study-act (PDSA) cycles. Key stakeholders were identified by hospital leadership to continuously improve compliance with the timeout and adherence to the newly developed guidelines. At each action planning meeting, compliance data from the previous month was shared and followed by feedback from hospital staff and brainstorming of process improvements. Process improvements were then assigned to specific team members and implemented before the next action planning meeting. To address underlying concerns about operating room sterility practices, an additional half-day workshop targeted at surgeons was delivered midway through the intervention period to improve perioperative infection prevention and control (IPC) practices. The workshop focused on reinforcing infection prevention checkpoints that might be present in the operating room, such as the use of sterility indicators, and aimed to empower surgeons to address high SSI rates through improved operating room antisepsis rather than extending postoperative antibiotic prophylaxis. The workshop was led by a member of the hospital staff, an experienced nurse involved in surgical IPC practices, to improve communication between the surgeons and IPC personnel. All surgeons who admitted patients to the general surgery ward were invited to participate in training workshops, stakeholder meetings, and process improvements.
Data collection
Personnel familiar with the hospital who had backgrounds in nursing and pharmacy were trained to collect data in the operating room and ward. Intraoperatively, data collectors were asked to record patient and procedure characteristics, including patient age, comorbidities, type of operation, and wound class. On the ward, data collectors conducted a chart review to capture postoperative antibiotic prescribing practices, length of stay (LOS), and disposition. Ward data collectors were also trained to observe ward communication behaviors in order to assess compliance with the antibiotic timeout. Teams were considered compliant with the antibiotic timeout if they stated the indication, duration, and type of antibiotic aloud on rounds.
Site selection and ethical approval
The program was piloted at a single referral hospital, St. Peter’s Specialized Hospital (SPSH), in Addis Ababa, Ethiopia from February to September 2023. The institutional review board at SPSH approved the study. All patients who underwent wound class I or II operations and were admitted to the surgical ward postoperatively were enrolled. Because this was a quality improvement program to implement evidence-based practices and did not involve risk to patients, patient consent was waived.
Outcomes
The primary outcome was the proportion of patients who had clean or clean-contaminated surgery receiving postoperative antibiotic prophylaxis for ≥24 h. Secondary outcomes included compliance with the antibiotic timeout, the duration of postoperative intravenous antibiotics for prophylaxis and for treatment of infection, and LOS.
Data analysis
Patient and procedural characteristics between the baseline period and the intervention period were compared with using chi-squared tests for categorical variables and t-tests for continuous variables. Our primary outcome was assessed by comparing the percentage of patients who received ≥24 h of antibiotic prophylaxis between the baseline and intervention groups using chi-squared tests. Compliance with the antibiotic timeout was compared with between baseline and intervention groups using chi-squared tests. LOS and the duration of postoperative antibiotics were compared between the groups using two-tailed T tests. To address differences in behavior, change among different groups of surgeons, we also compared with patients who underwent general surgery, who made up the largest cohort of patients, to those who underwent subspecialty surgery, including orthopedic surgery, neurosurgery, urologic surgery, and head and neck surgery. Statistical analysis was performed in Stata/SE 16.1 (College Station, Texas, USA).
Results
A total of 636 patients who had clean or clean-contaminated surgery were enrolled in the study,159 (25%) in the baseline group and 477 (75%) in the intervention group. Patient and procedural characteristics were similar between baseline and intervention groups (Table 1).
Patient and Procedural Characteristics among All Enrolled Patients and Wound Class I and II Patients
The percentage of patients who had clean or clean-contaminated surgery receiving ≥24 h of postoperative prophylaxis decreased 19.6%, from 50.9% in the baseline period to 40.9% in the intervention period (p = 0.027) (Table 2). General surgeons appeared to drive improvements, with a 28.9% decrease in patients receiving prolonged postoperative prophylaxis among general surgeons (p < 0.001) compared with to a nonsignificant reduction of just 4.1% among subspecialty surgeons (Table 2). Rates of prolonged postoperative prophylaxis continued to improve throughout the intervention, with a pronounced reduction in prolonged prophylaxis during guideline development followed by a period of incremental improvements in the following months (Fig. 2). Compliance with the ward-based antibiotic timeout improved but failed to reach significance; 12.0% of patients had a timeout performed in the baseline period compared with 16.1% in the intervention period (p = 0.201) (Table 2). Compliance with the timeout was highest at the start of the intervention period when timeout training was delivered and guideline development was ongoing; however, compliance subsequently fell to baseline levels (Fig. 2).

Changes in the proportion of patients receiving postoperative antibiotic prophylaxis and compliance with the antibiotic timeout over time.
Changes in Compliance with the Antibiotic Timeout, Postoperative Antibiotic Prescribing Behaviors, and Length of Stay
There was a reduction in duration of antibiotics given for postoperative prophylaxis (from 2.1 to 1.5 d, p = 0.003) and for treatment of infection (from 4.9 to 3.4 d, p = 0.031). Antibiotics for treatment of infection were most often given for SSI. Overall, there was a significant reduction in LOS, from 4.0 days (3.1–4.5) in the baseline period to 3.5 days (3.3–3.7) in the intervention period (p = 0.047). By the final weeks of the intervention, LOS was approximately one day shorter than in the baseline period (Fig. 3). Trends in the mean weekly duration of postoperative prophylaxis and LOS had similar reductions over time (Fig. 3).

Trends in postoperative prophylaxis and LOS over time. LOS, length of stay.
Discussion
Developing and deploying hospital antibiotic stewardship guidelines was effective in reducing the number of surgical patients receiving postoperative prophylaxis and was associated with reductions in postoperative LOS. Although ward-based antibiotic timeout compliance improved only transiently, teams made considerable reductions in the length of postoperative antibiotic prophylaxis and continued to improve through the length of the study.
The goal of this quality improvement program was to connect available evidence to practice. While postoperative antibiotic prophylaxis is common in Ethiopia despite a lack of evidence to support its use, at the time of this intervention, the hospital had few systems to enforce antibiotic stewardship, and none for the surgical ward. We empowered changes by protocolizing antibiotic prescribing through guidelines and by creating an antibiotic timeout tool to act as a teachable moment to bring guidelines into practice. Reductions in postoperative LOS suggest this intervention may have further effects on resource utilization for both patients and hospitals.
The key component of the intervention was the development of hospital-specific antimicrobial stewardship guidelines for the surgical ward; we initiated guideline creation through delivery of a workshop, which introduced or reinforced foundational knowledge on antibiotic resistance and took the participants through a guideline development process. Although we did not insist that any particular aspect of stewardship was incorporated into the guidelines, we presented robust evidence for the cessation of postoperative prophylaxis in wound class I and II operations; for the most part, these recommendations were incorporated. However, workshop participants were not limited to focusing on the cessation of postoperative prophylaxis and included broader recommendations on the use of therapeutic antibiotics, resulting in significant reductions in the length of therapeutic antibiotics as well.
In a qualitative study of low-resource contexts where antibiotic stewardship efforts were sparse, physicians identified the need for local guidelines as an important tool. 23 In Ethiopia, as well as other African countries, adherence with both national and international guidelines remains poor, which may indicate a lack of acceptability or appropriateness of these guidelines in the local context.17,24 The guideline development process itself proved valuable in changing behavior; the six week period of guideline development was associated with the largest improvements in prescribing practices and highest compliance with the antibiotic timeout (Fig. 2, Fig. 3). Ongoing changes in prescribing practices following guideline approval may reflect the improvements made as part of PDSA cycles using monthly action planning meetings; this allowed for additional feedback and process changes led by hospital staff. For example, changes suggested during these meetings included restructuring team dynamics between surgeons and pharmacists, allowing pharmacists to take a key role in enforcing the newly created guidelines, and addressing communication failures between general practitioners, surgeons, and nurses.
General surgeons, who comprised the largest stakeholder group, made the largest improvements in reductions in postoperative prophylaxis. General surgeons were key stakeholders in program implementation as several held leadership positions within the hospital; they were key attendees at action planning meetings and workshops and held leadership roles on the implementation team. Further, while other care team members, such as nurses, general practitioners, and pharmacists, work across surgical specialties, in this setting, surgeons are often considered team leaders. The failure for antibiotic prescribing practices to improve in patients who had operations done by subspecialty surgeons suggests poor engagement of surgeons from those specialties, despite strong engagement from other members of the care team.
This study has several limitations. The study used a pre–post design which relied on data collectors observing behaviors on rounds. Direct observation may have motivated behavior change by care teams. 25 Data collectors were not blinded to the intervention but were also not necessarily involved in guideline development or process changes. As a data quality check, a member of the study team observed ward rounds several times a week to ensure data being recorded was based on actual team communication. Furthermore, it is unclear if the timeout itself mediated changes in prescribing practices. Compliance with the timeout did not reach 50% at any point during the intervention. It is possible that the improvements in team communication early in the intervention period were adequate to orient clinical teams to changes in practice. Alternatively, changes may not have been mediated through the timeout at all, but rather through the presence of a clinical pharmacist who had not previously been involved in ward round decisions on postoperative antibiotic use. Finally, these findings are limited to a single pilot site and focus on a limited scope of surgical procedures. Implementation in additional hospitals is ongoing to address whether this program can be successful in other settings and with other teams.
In the current study, we opted not to track 30-day SSI outcomes, as a number of studies have consistently shown that stopping antibiotic prophylaxis within 24 h postoperatively to be safe and not associated with higher rates of SSI in wound class I and II operations.9,22 However, following this pilot, further investigation is ongoing, which aims to demonstrate that this program reduces unnecessary antibiotic prophylaxis without increasing SSI rates, in the hopes that this reinforces the safety of implementing such this quality improvement program. In our previous work, we have also observed that a prolonged course of antibiotics was associated with longer LOS, placing additional burden both on resource-limited health systems and patients. 9 While the LOS reductions in this pilot represent data from only one hospital, the resource-utilization benefits found here warrant further study to assess generalizability to other settings as well sustainability beyond the conclusion of the program.
This intervention addressed antibiotic prescribing behaviors but did not address the underlying processes needed to prevent surgical infections. Poor infection prevention practices have been cited as a common driver of antibiotic overprescribing, resulting in higher SSI rates and higher rates of antibiotic resistance.26,27 In lower-resourced countries, antibiotics are prescribed both for the prevention and treatment of SSIs, but in one third of cases, the causative organisms are resistant to the initial antibiotic used for prophylaxis. 27 This program is built on lessons from Clean Cut, 24 a quality improvement program aimed at reducing SSI, which has been successfully piloted, scaled, and assessed for sustainability.7,28,29 High rates of prolonged postoperative prophylaxis were observed at hospitals participating in Clean Cut, prompting the need for further efforts to address antibiotic stewardship. Combined efforts at improving infection prevention processes and antibiotic stewardship may work synergistically. Ultimately this approach may benefit from being implemented in parallel to a more comprehensive perioperative infection prevention program where underlying drivers of antibiotic overprescribing are addressed.
Footnotes
Acknowledgments
The authors would like to thank the data collectors, administrators, nurses, and surgeons who made this program possible. Additionally, the authors would like to thank Kris Torgeson and Katie Fernandez, Lifebox Chief Executive Officer and Chief Programs Officer, respectively, and Dr. Metasebiya Mesfin, Dr. Ahadu Workineh, and Dr. Abreham Eshetu, St. Peter Specialized Hospital’s Chief Executive Officer, Academic and Research Director, and Medical Director, respectively, for their help and support in this program.
Authors’ Contributions
M.R.N.: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Visualization, Writing—original draft. A.T.: Conceptualization, Project administration, Investigation, Writing—review and editing. N.G. Conceptualization, Investigation, Methodology, Writing—review and editing), M.N.M. (Data curation, Resources, Writing—review and editing. I.H. Data curation, Resources, Writing—review and editing. K.B.: Project administration, Resources, Writing—review and editing. B.G.: Project administration, Resources, Writing-review and editing. N.S.: Conceptualization, Writing—review and editing. K.A.: Data curation, Resources, Writing—review and editing. Y.S.: Project administration, Resources, Writing—review and editing. S.B.A. Project administration, Resources, Writing—review and editing. T.N.M. Project administration, Supervision, Writing—review and editing. T.G.W.: Conceptualization, Supervision, Writing—review and editing.
Data Availability
De-identified data can be made available upon reasonable request to the authors.
Author Disclosure Statement
Maia Nofal and Natnael Gebeyehu are Lifebox Safe Surgery Fellows. Assefa Tesfaye is the Lifebox Clean Cut Clinical Lead. Nichole Starr is a Clinical Advisor at Lifebox. Tihitena Negussie Mammo is the Global Clinical Director at Lifebox. Senait Bitew Alemu is Lifebox’s Head of Program for East, Central, and Southern Africa. Thomas Weiser is a member of the Global Governance Council at Lifebox.
Funding Information
This study was funded in part by a grant from the Stanford Department of Surgery and the Stanford Center for Innovation in Global Health. MN and NS were supported by the NIH Fogarty International Center Global Health Equity Scholars Program NIH FIC TW010540.